Double aortic arch
Right arch dominant
Left arch dominant
Balanced double arch
Right aortic arch
Mirror image branching
Retroesophageal left subclavian artery
Circumflex aorta
Pulmonary artery sling
Innominate artery compression
Double aortic arches are further subgrouped based upon arch dominance (right dominant, left dominant, or balanced). Those vascular rings associated with a right arch are classified as right arch with mirror image branching, right arch with retro esophageal left subclavian artery, or circumflex aorta which denotes a right arch but a left-sided descending thoracic aorta. This can be associated with aortic arch hypoplasia.
Embryology
In a human embryo, there are six paired pharyngeal (aortic) arches. They arise from the aortic sac and course posteriorly to connect to the right and left dorsal aorta, respectively. After a series of regression and differentiation events, this embryonic arch system ultimately gives rise to the adult aortic arch, its branches, and the pulmonary arteries. A brief understanding of this embryonic process is helpful to appreciate the anatomy of these vascular rings and for the interpretation of radiological images.
Arches 1 and 2 regress and give rise to maxillary and stapedial arteries. In humans, the fifth arch does not form to any significant degree. The third arch forms the common carotid arteries bilaterally. The sixth arch forms the left and right pulmonary arteries respectively along with the patent ductus arteriosus. Normally, the left fourth pharyngeal arch will form a portion of the adult aortic arch (between the left carotid and left subclavian arteries) whereas the right fourth arch will regress and form the right subclavian artery. A right aortic arch results when this pattern of normal regression is reversed. Similarly, persistence of both right and left fourth arches will form a double aortic arch.
Clinical Presentation and Diagnosis
Depending on the severity of compression of both the esophagus and trachea due to a vascular ring, patients may have symptoms within the first few months of life. However, it is not unusual to see patients that present with significant symptoms at a much later date, even in adulthood. Presentation is generally dependent upon the severity of obstruction based upon the “tightness” of the ring itself. Tighter lesions, like the double aortic arch and pulmonary artery slings, usually present earlier (within 3 months of age) relative to those that are loose such as aberrant right subclavian artery that typically present at greater than 6 months of age [2].
The most common symptoms from these vascular anomalies arise from the external compression of trachea and esophagus. These symptoms include inspiratory stridor, dyspnea, cough, wheezing, and dysphagia. In addition to obstruction of airflow, tracheal compression also impedes mucociliary clearance and, as a result, many patients will also suffer with recurrent respiratory tract infections [3]. Since these symptoms are shared with many other and more prevalent childhood illnesses, these patients can have a significant delay in diagnosis. Often they will receive long-term bronchodilators in an attempt to treat asthma and multiple courses of antibiotics to treat upper respiratory infections before the actual disease is accurately diagnosed. Persistence of these symptoms, especially when they do not respond to routine treatment, should alert the pediatrician of the possibility of a vascular ring. Only a high index of suspicion will ensure these patients receive early diagnosis and appropriate therapy.
Diagnosis
With the availability of more sophisticated imaging techniques, many recent publications give only historical value to the chest radiograph findings in these patients [4]. The chest X-ray is usually the first imaging study performed in a child with airway obstruction and can frequently point toward the presence of a vascular ring. Films should be assessed for the laterality of the aortic arch and for evidence of tracheal compression at the level of the arch, often better visualized on lateral films.
Absence of an aortic knuckle on the left side suggests a right arch, and when present in a child with symptoms of airway obstruction, a vascular ring should be strongly suspected. A right aortic arch may be suspected if the distal trachea is seen slightly deviated to the left instead of the right, because of the aortic arch bowing over the right main stem bronchus instead of the left. Similarly, a double aortic arch is likely if the sidedness of the arch cannot be determined on chest X-ray. Hyperinflation of the left lung with the left hilum lower than the right may suggest a pulmonary artery sling. The location of the descending aorta can usually be determined by inspecting the paraspinal line and the azygoesophageal recess.
A barium esophagogram used to be the most extensively used imaging study for the diagnosis of a vascular ring. Contrast swallow will show a posterior indentation of the esophagus in all vascular anomalies except in the presence of a pulmonary artery sling, which will produce an anterior indentation on the esophagus and an increase in the space between the esophagus and trachea at the same level.
Upon bronchoscopy, vascular rings appear as an external compression of the trachea just above the carina. Routine bronchoscopy is not necessary in a symptomatic patient with a radiologically proven vascular ring. However, it plays an essential role in the diagnostic workup of an infant with airway obstruction and an unclear cause. Bronchoscopy may also reveal additional associated airway lesions, such as tracheomalacia, complete tracheal rings, and tracheal stenosis, which may be commonly associated with vascular anomalies. In fact, vascular rings and innominate artery compression are the most common congenital cause for secondary tracheomalacia [5]. The diagnosis of innominate artery compression is almost always based on its classical findings on bronchoscopy of anterior pulsatile compression of lower trachea.
Both computed tomography (CT) and magnetic resonance imaging (MRI) are extremely useful techniques in the diagnosis of a vascular compression of the airway. The greatest advantage of these imaging modalities is their capability to completely delineate the anomaly along with their relationship to the adjacent structures. Both provide post-processed 3D images that can be very helpful in planning a surgical intervention. However, a limitation common to both these techniques is their inability to directly visualize obliterated structures. Even so, based on branching patterns, the laterality of the arch, and compression of the airway, a diagnosis of vascular ring can usually be reached. There are advantages as well as disadvantages to both modalities. We feel that CT provides excellent tracheal images at a minimal risk of ionizing radiation. MRI, on the other hand, provides a superior assessment of cardiac anatomy and function in the case that additional information is helpful. Yet, scan times are much longer thus requiring sedation and anesthesia in most infants and toddlers.
Echocardiogram can easily identify branching patterns and sidedness of the arch. It can also identify a double aortic arch when both the arches are patent. However, it is not useful to identify an obliterated lumen. It is helpful in the identification of congenital heart disease commonly associated with vascular rings such as the association between right aortic arch and tetralogy of Fallot, the incidence of which can be as high as 30 %.
Before CT and MRI were widely available, angiography was very frequently used to diagnose vascular rings. Since MRI and CT can provide essentially the same information noninvasively, a cardiac catheterization is now very infrequently utilized, unless needed for an associated cardiac disease.
Double Aortic Arch
This is the most common symptomatic vascular ring present in 0.05–0.3 % of the population and results from the persistence of both right and left fourth primordial arches. Two aortic arches arise from the ascending aorta and pass on either sides of trachea and esophagus to meet the descending aorta posteriorly, forming a complete ring. The right and left carotid and subclavian arteries arise from their respective arch. In almost 70 % patients, the right arch is larger (dominant), posterior, and more cephalad than the left, in about 25 % the left arch is dominant and in about 5 % patients both arches are balanced (Fig. 1).
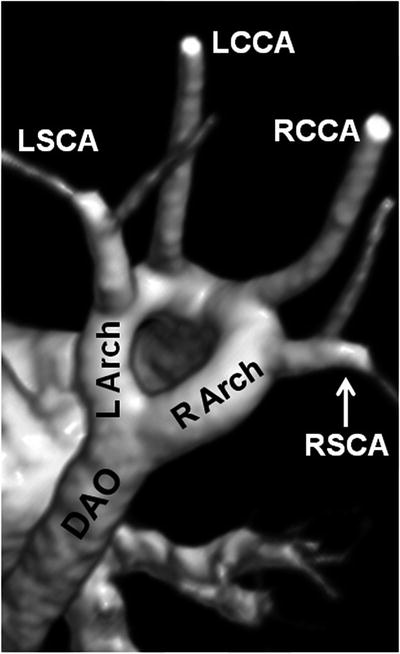
Fig. 1
Magnetic resonance angiogram of an unobstructed double aortic arch viewed from right posterior oblique with cranial angulation. Note that the right aortic arch is slightly larger. Descending Aorta (DAO), Left-Sided Arch (L Arch), Left Common Carotid Artery (LCCA), Left Subclavian Artery (LSCA), Right-Sided Arch (R Arch), Right Common Carotid Artery (RCCA), Right Subclavian Artery (RSCA)
A double aortic arch will usually cause significant narrowing and anterior bowing of thoracic trachea, and this can occasionally be seen on a lateral chest radiograph.
The surgical treatment of a double aortic arch consists of division of the lesser of the two arches.
For most patients, the approach is through a left posterolateral thoracotomy. In rare circumstances, a right thoracotomy is utilized in patients with a dominant left arch. After adequate exposure via thoracotomy, the ligamentum arteriosum, both arches, neck vessels, and descending aorta are clearly identified and both the ligamentum as well as the lesser of the two aortic arches are divided between vascular clamps, usually where the arch joins the descending aorta posteriorly. The divided ends are then oversewn using polypropylene sutures. Frequently, there will be an atretic segment in the lesser aortic arch in which case this site is then ideally suited for division.
Intraoperatively, it is useful to have pulse oximetry and/or pressure monitoring available for both upper and lower limbs. With balanced arches, blood pressure is checked in the lower limbs, while the clamps are alternately applied to each arch. The arch associated with a lesser fall in blood pressure in the lower limbs is then divided. If no appreciable difference is noted, it is preferable to divide the right arch, as its anatomical location poses a higher risk of continued compression of the trachea.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


