Rhytidectomy (Face-Lift)
Russell W. H. Kridel
Zahi Abou Chacra
The principal role of rhytidectomy is to elevate facial tissues that have descended with the aging process. Although skin excision is performed in a face-lifting procedure, contrary to the once predominant common belief, it is often not the dominant or sole goal one should try to achieve. Most current face-lift techniques rely on resuspension of the superficial musculoaponeurotic system (SMAS), whether through a SMAS or deep plane approach, with redraping and removal of skin without tension. The authors are witness to a steady evolution of technical and anatomical advances producing a new generation of facelifts. Presently, the authors continue to evaluate these newer techniques in search of the ideal procedure, which will give our patients a long-term, natural correction with rapid recovery and few complications.
GENERAL CONSIDERATIONS AND ADJUNCTIVE PROCEDURES
Aging face patients requesting consultation for a face-lift generally seek a youthful, more rested appearance. These patients have a well-developed self-image and do not want to look different. Rather they desire a natural-appearing result that turns back the hands of time to a more youthful version of themselves. For the surgeon, the goal is to determine what physical characteristics of the face are contributing to the impression of aging, which stigmata are reversible, and by what means. Ideally, the surgeon brings to this consultation a thorough understanding of the processes that lead to an aged appearance and is familiar with a wide variety of medical and surgical interventions appropriate for addressing the clinical problem. As with all elective facial plastic surgery, it is imperative for the surgeon to achieve a balanced, harmonious result. The patient who presents with an interest in face-lift who also has brow ptosis and four-quadrant dermatochalasis can be poorly served if the incongruity is not discussed prior to proceeding with the surgery. Moreover, oftentimes these patients will be left with more stigmata of a lifted appearance should they only address the lower face due to this incongruity. For these reasons, in addition to the face-lift, it is important to discuss the potential benefits of browlift, blepharoplasty, skin resurfacing (laser, chemical peel, and dermabrasion), as well as adjunctive procedures such as soft tissue fillers (like hyaluronic acid and calcium hydroxyapatite), fat injection, alloplastic implants, or muscle-paralyzing agent injections like Botox and newly approved Dysport. These are adjunctive procedures that complement face-lifting surgery and address the general theme of facial rejuvenation, which sometimes face-lifting cannot achieve alone.
A recent paradigm shift among many authors is volume preservation and restoration in the aging face, rather than just resuspension of deep tissues. This paradigm shift is partly demonstrated by the increasing use of biologic and synthetic injectable fillers in facial plastic surgery. Other commonly used volume-augmenting strategies for facial rejuvenation include fat injections and alloplastic implants. Proponents of such techniques argue that fat and tissue atrophy happen along with gravitational changes. Recently, Lambros (1) compared pictures taken up to 50 years apart and studied the effect of aging on the midface and periorbital complex. He concluded that there was little ptosis at the lid-cheek junction and that the aged appearance was partly due to volume loss. In another of his papers, he proposed how the addition of volume may give better results than traditional surgical methods (2). He emphasized that a face that has enough tissue volume is the best predictor of a face-lift outcome. It is our opinion and the one of many other surgeons that volume restoration is an important adjunct but does not replace the need for a surgical lift. The authors do, however, recognize that for some patients with volume loss as well as tissue descent, both problems must be addressed to produce natural, harmonious, and complimentary results.
The term face-lifting is sometimes a misleading term to patients, as it does not spell out which structures will be lifted. It says nothing about the neck, which is a main area of most lifting procedures, and on the other hand, it implies that the upper third of the face will be lifted, which most surgeons consider another procedure that they would address separately, such as with a forehead lift.
Most patients undergoing today’s typical face-lift are really getting a lower face- and neck lift. To lift the upper third of the face, for instance, one should rely on a forehead lift. In his recent publication, McCollough stresses that the term face-lift is often inadequately used. He describes five progressive stages of aging and proposes a classification that helps matching the specific aging stage with the appropriate rejuvenation treatment (3). His system describes procedures based on anatomic locations such as temple lift, forehead lift, cheek lift, and neck lift, diminishing confusion around the more generic widely used face-lift term. This chapter focuses only on the anatomy and clinical considerations of the present-day rhytidectomy procedure.
PHYSIOLOGY OF THE AGING FACE
To understand the present-day rhytidectomy procedure, the surgeon must have full knowledge not only of the underlying surgical anatomy but also of the aging physiology of the face, which leads patients to seek rejuvenation surgery. In general, the aging face presents five landmarks that are points of interest to patients and surgeons alike. These areas include (a) the jowl, (b) the deepened nasolabial folds and lateral perioral jowling, (c) the platysma banding and submental fullness in the neck region, (d) the orbicularis oculi and malar fat pad ptosis, and (e) the aging skin itself (Fig. 188.1A).
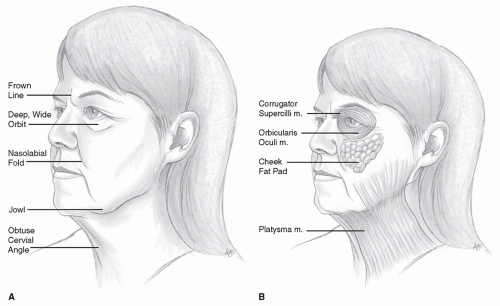 Figure 188.1 A: Topographic changes seen in the face with aging. B: Underlying soft tissue and muscular changes seen in the aging face. (Adapted from Zimbler MS, Kokoska MS, Thomas JR. Anatomy and pathophysiology of facial aging. Facial Plast Surg Clin North Am 2001;9:179-187.) |
In youth, the facial skin is maintained in normal anatomic position by retaining “ligaments” that run from deep facial structures to the dermis itself (4). With aging, attenuation of these “ligamentous” supports then results in malar soft tissue descent. The result of this descent is not only deepening of the melolabial folds but also jowling of the platysma and soft tissue between the masseteric and mandibular ligaments at the jawline. Moreover, this descent of the malar fat pad along with ptosis of the orbicularis oculi also results in hollowing in the infraorbital region. Finally, loss of platysma muscle tone results in anterior banding and the classically pictured “turkey gobbler” neck (5) (Fig. 188.1B).
Separate from the described underlying soft tissue changes, the surgeon must note the cumulative effects of the inherent aging process coupled with the effects of environmental exposure on the skin itself. While a comprehensive review of the changes associated with aging skin is beyond the scope of this chapter, it is important for the surgeon to have a fundamental understanding of
these changes. In this regard, it is convenient to think of skin aging in terms of extrinsic and intrinsic factors, affecting both the epidermis and the dermis (6). Extrinsic factors refer to environmental insults such as sun-induced damage (photodamage). Intrinsic aging refers to the natural effects of time and is generally characterized by tissue atrophy and descent and reduction in skin cellular and protein components. In fact, chronologically aged skin has reduced epidermal thickness, flattening of the dermal-epidermal junction, atrophy of the dermis, and a general decline in a variety of cell populations including melanocytes and Langerhans cells (7). This epidermal thinning then makes the skin more susceptible to damage from shearing-type forces (6). Moreover, Yousif and Mendelson (8) showed how habitual facial expressions lead to coarse skin wrinkling and deep folds. However, Kligman et al. (9) noted that in point of fact, there are no histologic features that distinguish the various types of wrinkles from the surrounding skin. He noted that instead there is a configurational change that results from mechanical stress acting on lax, excessive skin, especially in actinically damaged regions.
these changes. In this regard, it is convenient to think of skin aging in terms of extrinsic and intrinsic factors, affecting both the epidermis and the dermis (6). Extrinsic factors refer to environmental insults such as sun-induced damage (photodamage). Intrinsic aging refers to the natural effects of time and is generally characterized by tissue atrophy and descent and reduction in skin cellular and protein components. In fact, chronologically aged skin has reduced epidermal thickness, flattening of the dermal-epidermal junction, atrophy of the dermis, and a general decline in a variety of cell populations including melanocytes and Langerhans cells (7). This epidermal thinning then makes the skin more susceptible to damage from shearing-type forces (6). Moreover, Yousif and Mendelson (8) showed how habitual facial expressions lead to coarse skin wrinkling and deep folds. However, Kligman et al. (9) noted that in point of fact, there are no histologic features that distinguish the various types of wrinkles from the surrounding skin. He noted that instead there is a configurational change that results from mechanical stress acting on lax, excessive skin, especially in actinically damaged regions.
On the other hand, photoaged epidermis is characterized by striking variability: in its thickness, with alternating areas of atrophy and hyperplasia; in pigmentation, with alternating lentigines and depigmented areas; in the degree of nuclear atypia; and in orderliness of keratinocytes maturation (10). In the past, sun-damaged epidermis was thought to be characterized by a reduction in structural elements, leading to skin wrinkling. In fact, the most striking feature of photodamaged skin is the presence of large quantities of thickened, poorly organized degraded elastic fibers, which degenerate into an amorphous mass, better known as elastosis. This loss of elastin decreases skin elasticity, defined as the loss of the ability of the skin to recoil and redrape once pulled away from the deep tissues (11). The result is aged skin, which does not retain moisture and which loosens and hangs. The ground substance component of the dermal connective tissue matrix is greatly increased. In the dermal cell population, photodamaged skin shows numerous, hyperplastic fibroblasts and abundant, partially degranulated mast cells, which result in a chronic low-grade inflammation termed heliodermatitis. Finally, photodamaged skin shows extensive changes in the microcirculation, which can affect flap viability. Along with skin changes, atrophy of underlying soft tissue and fat have also been described. Skeletal changes pertaining to both bone loss and bone remodeling also occur with aging.
Overall the aging face can be viewed as a coupling of redistributed ptotic underlying soft tissue with overlying skin changes. Together, these changes combine to contribute to the overall impression of the aging face. For most aging face patients, this means that facial rejuvenation will necessitate the surgeon concentrating on five points of interest: (a) the jowl, (b) the deepened melolabial and nasolabial folds, (c) the neck, (d) the malar region, and (e) the skin itself.
SURGICAL ANATOMY
The last 20 years have brought about numerous improvements in the face-lift surgery. These new advances have largely come about through better anatomical understanding as well as an understanding of how the aging process alters these anatomical components throughout the face and neck. Certain salient points of the facial anatomy for rhytidectomy, including vascular supply, details of the SMAS and its relation to the facial nerve, as well as the presence of retaining “ligaments,” are described here.
The facial skin is supplied by branches of the external carotid artery. Specifically, the superficial temporal artery, facial artery, transverse facial artery, and infraorbital artery anastomose with one another in the subdermal plexus. The internal carotid artery also contributes to the facial skin centered around the radix and the glabella through branches of the ophthalmic artery. However, this area is not routinely addressed during face-lifting. The elevated subcutaneous flap is based solely on the subdermal plexus, which is supplied by muscular cutaneous arteries arising from branches of the facial and infraorbital arteries. Unfortunately, the standard subcutaneous and SMAS two-layered face-lift effectively divides the skin from its underlying perforating branches. A recent study comparing the vascular anatomy of basic skin flaps in the subcutaneous and SMAS rhytidectomy, the composite rhytidectomy, and the subperiosteal rhytidectomy found, not surprisingly, that the best blood supply was found in subperiosteal dissection while the most tenuous supply was in the subcutaneous flap (12). However, outside of smokers and those patients with small vessel disease, one must consider that each of these techniques has been used for many years with minimal low flap perfusion rate complications (5).
Perhaps the first, and most important, development in the evolution toward the present-day rhytidectomy was the description of the SMAS. In fact, while the precise boundaries of the SMAS continue to be a source of debate, the significance of this fascial layer in relation to present-day rhytidectomy is unquestionable. The SMAS, which is a fibromuscular fascial layer, invests and interlinks the muscles of facial expression. Moreover, in this function it maintains consistent relationships with the facial nerve and major vessels within the facial region. For the operating surgeon, mastery of these relationships and planes of dissection are therefore critical (13).
The regional variations that are found in the relationship between the SMAS and the neurovascular structures are most profound when examining the SMAS and the facial nerve above the zygoma versus below the zygoma (14). Specifically, in the temporal region above the zygoma, the superficial temporal artery and frontal branch course through the SMAS (also called temporoparietal fascia). Below the zygoma, the SMAS fans out over the parotid gland and then above the masseter muscle before it surrounds the facial mimetic muscles. Therefore, in the lower face, the facial nerve branches are always deep to the SMAS and innervate the facial mimetic muscles on their undersurface (Fig. 188.2).
However, there are three exceptions to that rule. The levator anguli oris, buccinator, and mentalis muscles lie in a somewhat deeper plane making their innervation from the facial nerve from their superficial surface, rather than their undersurface. It should be noted that even in the deep plane and composite lifts, the dissection medial to the zygomaticus major and minor is actually above the SMAS because the SMAS thins out over this region. Moreover, it should be noted that a significant, distinct myofascial layer superficial to the parotid fascia is not always clinically apparent. In fact, Jost and Levet (15) have suggested that the SMAS overlying the parotid includes what the authors have otherwise distinguished as the parotid fascia.
However, there are three exceptions to that rule. The levator anguli oris, buccinator, and mentalis muscles lie in a somewhat deeper plane making their innervation from the facial nerve from their superficial surface, rather than their undersurface. It should be noted that even in the deep plane and composite lifts, the dissection medial to the zygomaticus major and minor is actually above the SMAS because the SMAS thins out over this region. Moreover, it should be noted that a significant, distinct myofascial layer superficial to the parotid fascia is not always clinically apparent. In fact, Jost and Levet (15) have suggested that the SMAS overlying the parotid includes what the authors have otherwise distinguished as the parotid fascia.
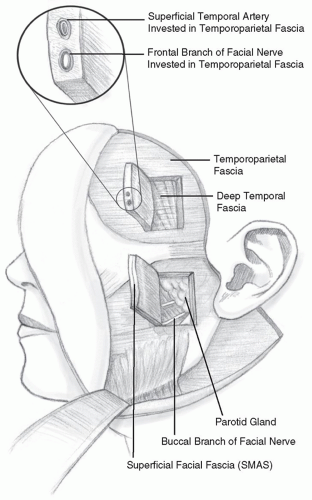 Figure 188.2 In the temporal region, above the zygoma, the frontal branch travels through the SMAS. In the lower face, below the zygoma, the facial nerve branches lie deep to the SMAS and innervate the facial mimetic muscles from their deep surface. (Adapted from Stuzin JM. The relationship of the superficial and deep facial fascias: relevance to rhytidectomy and aging. Plast Reconstr Surg 1992;89(3):441-449.) |
Finally, as previously alluded to, the SMAS has been noted to have a number of “ligamentous” supports, which make it adherent at specific points to the overlying dermis and underlying muscular/osseous attachments. Specifically, four ligaments support the soft tissues of the cheek: (a) the parotidomasseteric ligament, (b) the platysmal auricular ligament, (c) the zygomatic ligament (McGregor patch), and (d) the mandibular ligament (Fig. 188.3). Although not true ligaments, these fascial condensations are especially important in the deep plane and composite rhytidectomy (16). Release of these ligaments is important and will allow the surgeon to achieve a better pull to redrape the tissue. However, this task must be undertaken with extreme caution as branches of the facial nerve are in close proximity.
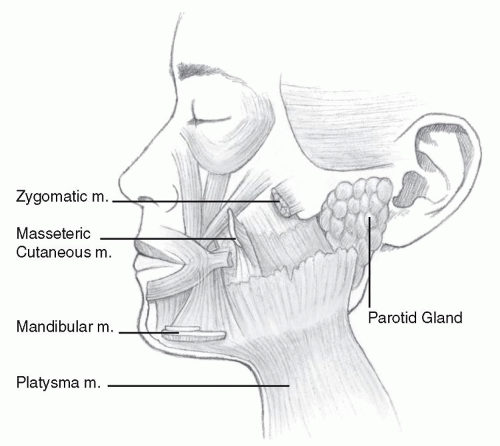 Figure 188.3 The four retaining ligaments of the cheeks. |
SURGICAL EVOLUTION: A HISTORICAL PERSPECTIVE
A steady evolution of anatomically derived technical advances has occurred in the rhytidectomy procedure since the early days of simple skin flap advancement. Reports of face-lifting attempts date back to the very first years of the 20th century and consisted primarily of skin excision and direct closure. This technique was utilized for over 50 years before the first major contribution to advance face-lifting was provided by Skoog. Sometime in the mid-1960s, Skoog began to elevate a “complex morphologic unit” in the cervical region and advance it posteriorly (17). It was observed that this “two-layered shift” of the cervical fascia corrected the anterior banding of the neck and the redundant skin of the cervical region. Skoog subsequently followed this with his description in 1974 of his technique of superficial rhytidectomy of the face and neck based on a subfascial dissection. The new era in face-lift surgery had begun (18,19,20).
It would take until 1976 before Mitz and Peyronie (21) defined the “complex morphologic unit” referred to by Skoog as the SMAS. The SMAS lift approach, which then became vogue, was a significant step in the evolution of the
present-day rhytidectomy. However, some surgeons, in pursuit of the ideal lift, still found the results of the SMAS lift to be short-lived and complicated by perioperative problems. For some surgeons, the SMAS lift did not appear to sufficiently address the ptotic midface and melolabial fold region. In an effort to enhance midface tissue, Faivre (22) described in 1988 the deep temporal face-lift in the sub-SMAS plane. That same year, Psillakis et al. (23) described the subperiosteal midface lift to correct ptotic malar fat pad. In 1990 and 1992, Hamra (24) published his techniques on deep plane face-lift and composite face-lift, respectively (25). In the deep plane face-lift, Hamra innovates on the Skoog technique by adding a superolateral elevation of the malar fat pad. The composite lift added dissection and resuspension of the orbicularis oculi muscle superomedially, thus effacing what the author has termed as the malar crescent, in an effort to rejuvenate the periocular complex and better create harmony with the lower parts of the face.
present-day rhytidectomy. However, some surgeons, in pursuit of the ideal lift, still found the results of the SMAS lift to be short-lived and complicated by perioperative problems. For some surgeons, the SMAS lift did not appear to sufficiently address the ptotic midface and melolabial fold region. In an effort to enhance midface tissue, Faivre (22) described in 1988 the deep temporal face-lift in the sub-SMAS plane. That same year, Psillakis et al. (23) described the subperiosteal midface lift to correct ptotic malar fat pad. In 1990 and 1992, Hamra (24) published his techniques on deep plane face-lift and composite face-lift, respectively (25). In the deep plane face-lift, Hamra innovates on the Skoog technique by adding a superolateral elevation of the malar fat pad. The composite lift added dissection and resuspension of the orbicularis oculi muscle superomedially, thus effacing what the author has termed as the malar crescent, in an effort to rejuvenate the periocular complex and better create harmony with the lower parts of the face.
Recently, many “newly named” face-lift techniques have been heavily marketed: the mini-lift, weekend lift, short flap lift, S lift, and lunchtime lift. Most of these lifts rely on a short skin flap and sometimes a minimal SMAS suspension. These less invasive procedures have the advantages of decreasing associated complications and substantially minimizing patient recovery time. However, in most cases their indications are limited to patients with limited signs of aging, and results from such techniques may be shortlived or less than ideal. Webster had explored short flap face-lifting in 1983, which many later abandoned (26).
To date, it is uncertain what percentage of surgeons are performing the extended sub-SMAS lifts versus the traditional SMAS plication/imbrication techniques. Moreover, questions remain as to the superiority of the results that are achieved in the deep plane versus plication techniques. In fact, while anecdotal reports abound to this effect, it will be very difficult to accomplish the study that can definitively answer this and a whole host of other questions. Proponents of deep plane rhytidectomy claim an improved nasolabial fold in comparison to the traditional SMAS suspension techniques (27). Adamson et al. (28) found a twofold improvement with deep plane measured by the degree of increased volume at the malar eminence and by the amount of effacement of the fold. Becker and Bassichis (29) concluded that results from a deep plane face-lift were not superior to those from SMAS plication in patients that are younger than 70 years old. Baker (30) and Kamer (31) maintain reservations regarding the superiority of the results from the deep plane lifts, especially when these “implied benefits” are weighed in relation to the added risks to the facial nerve. Baker and Conley (32) notes that a review of the world literature in 1979 found an incidence of 0.01% permanent facial nerve injury in deep plane cases. He notes in a later paper (30) that the published articles on the new deep dissection techniques conjure concern as they report a relatively high incidence of facial weakness in the hands of extremely qualified surgeons. He questions what happens when these procedures are attempted by less experienced surgeons. Time and experience are still needed before the authors will know if the added work and increased potential risk for complication is worth the improved aesthetic results. In a recent systematic review of 39 articles comparing the efficacy and complication rate of different face-lift techniques, Chang concluded there was a lack of quality data to be objectively compared (33). It is also important to note that results will always vary from surgeon to surgeon due to skills and expertise.
ASSESSING CANDIDACY
With an understanding of the physiologic and anatomical changes that present with facial aging, the surgeon is ready to determine whether the patient is a candidate for facial rejuvenation surgery in general and rhytidectomy in particular. This evaluation includes surgical, medical, and psychological components.
The surgical criterion to be addressed is whether rhytidectomy will create physical changes in the patient’s face that will contribute meaningfully to a more youthful appearance. In making this determination, it is helpful to divide the stigmata of facial aging into two categories: those that are improved by repositioning of facial tissues and those that require changes in the structure of the tissues themselves. In the first category, one would include ptosis in the jowl, submentum, and anterior neck leading to a disruption of the ideal youthful contours of the jawline, cervicomental angle, and neck, respectively. These are the primary areas improved by rhytidectomy. Malar ptosis will experience modest improvement as well.
On the other hand, intrinsic changes in the tissues themselves are not well addressed by rhytidectomy. As noted earlier, concomitant with the ptosis described above, aging brings about many changes in the skin itself. Fine lines and deeply etched wrinkles in the skin are the grossly visible correlates of crevices in the dermis and subcutaneous tissues formed over time as a result of actinic damage, senescence of connective tissues, and habitual facial expressions. These cosmetic defects will be minimally improved, at best, by rhytidectomy. Instead, they can be addressed more directly by resurfacing techniques, including both chemical and laser exfoliation. In the situation in which such intrinsic properties of the skin comprise a significant portion of the aesthetic problem, the patient should be encouraged to consider skin resurfacing as an adjunct or, in some cases, an alternative to rhytidectomy.
Once the surgeon has determined that a rhytidectomy will address the patient’s aesthetic concerns appropriately, it is imperative to assess medical candidacy for the procedure. Most patients who seek cosmetic surgery are in good health, so medical contraindications to the proposed procedure are rarely seen. Vigilance is essential for avoiding disaster. Facelift candidates—people who feel young inside and want their outward appearance to mirror that vitality—are exactly the same people who tend to minimize medical complaints and even may forget to relate serious medical problems
unless questioned directly. Significant bleeding diatheses and American Society of Anesthesiologists (ASA) class IV or V, in which a patient has a dangerously compromising medical condition, should he considered absolute medical contraindications to rhytidectomy. A patient in ASA class III, in which a medical condition impairs the patient’s activities to some degree, should be approached with great caution. The severity of the condition and its potential impact on the safe conduct of the operation should be explored in detail. Conditions that may adversely affect healing including uncontrolled diabetes, diseases requiring chronic steroid therapy, or connective tissue abnormalities like the Ehlers-Danlos syndrome should be considered strong relative contraindications to face-lift surgery. Consultation with the primary care physician may be necessary to coordinate prescription medication regimens and facilitate the management of relevant medical conditions.
unless questioned directly. Significant bleeding diatheses and American Society of Anesthesiologists (ASA) class IV or V, in which a patient has a dangerously compromising medical condition, should he considered absolute medical contraindications to rhytidectomy. A patient in ASA class III, in which a medical condition impairs the patient’s activities to some degree, should be approached with great caution. The severity of the condition and its potential impact on the safe conduct of the operation should be explored in detail. Conditions that may adversely affect healing including uncontrolled diabetes, diseases requiring chronic steroid therapy, or connective tissue abnormalities like the Ehlers-Danlos syndrome should be considered strong relative contraindications to face-lift surgery. Consultation with the primary care physician may be necessary to coordinate prescription medication regimens and facilitate the management of relevant medical conditions.
On the other hand, there are no age limitations for facelift surgery, and age should not be a reason to deny surgery if the patient is in otherwise good health. A healthy patient in his or her late 70s or early 80s may have 15 or 20 more years of quality life ahead, and the desire to have an improved appearance is indeed valid.
Finally, but not least important, an accurate assessment of the patient’s psychological status is central to determining patient candidacy. The surgeon should determine patient motivation and attempt to ascertain whether the patient might fail to view a successful surgical outcome favorably or might react inappropriately to any aspect of the surgery. A thorough discussion of the patient’s goals and objectives should provide important clues to his or her psychological profile (34). Although many patients are unaware of exactly what surgery can and cannot accomplish, others have clearly unreasonable expectations, which can include looking exactly as they did 10 or 20 years ago, having surgery without scars, requesting an unnaturally tight lift, or attempting to obtain promises and guarantees. Patients who are excessively occupied with minute flaws also may be poor surgical candidates. Moreover, patients who have recently undergone a major change in their personal status, such as the death of a loved one or divorce, may be subject to depression or psychological unevenness and may require special care.
PREOPERATIVE EVALUATION AND PLANNING
General Considerations
Once a patient is deemed an appropriate candidate for rhytidectomy, they need to be educated clearly before surgery. They must understand that rhytidectomy helps with excessive skin and jowling and provides for redraping of the skin, but it does not change the quality of the skin itself. If fine or deep rhytids are present preoperatively, they will be present postoperatively as soon as the swelling goes down. In severely sun-damaged patients, full-face deep chemical peeling with phenol solution or CO2 laser resurfacing is often necessary as an adjunct and can be done several weeks after the initial face-lift surgery. If there are significant rhytids limited to the perioral or periorbital areas, these cosmetic units may be safely peeled or removed by laser simultaneously with the rhytidectomy as long as these areas are not undermined during the procedure. Undermined areas are partly devascularized in the immediate postoperative period and further skin insult by laser resurfacing could lead to skin necrosis.
To assess further the overall improvement possible with rhytidectomy, the underlying structure of the face must be critically evaluated. Patients who had a good bony structure of the cheekbones, chin, and jaw during their youth will have the best results, as the redraping of skin will help to highlight these attractive bony structures. Therefore, patients who have a thinner, angular face and good bony definition are generally much better candidates than patients with rounder faces, low cheekbones, or a short mandible (Figs. 188.4, 188.5, 188.6).
Adjunctive chin and submalar cheek augmentation may be necessary in conjunction with a face-lift to achieve the desired result. Patients who have a retrusive chin cannot get desired cervicomental definition without a chin implant, even after a face-lift. Also, because the aging process sometimes causes a hollow-cheek deformity due to the atrophy of soft tissue and fat with ptosis of the fat pads, older patients sometimes require submalar augmentation or resupport of the fat pads simultaneously with the face-lift. Redraping the skin alone will not replace soft tissue cheek hollowness.
As the underlying structures of the face dictate the aesthetic results possible above the jawline, those in the neck similarly limit the outcome there. In particular, the position of the hyoid bone relative to the mandible varies from patient to patient. This relationship defines the course of the suprahyoid musculature of the floor of the mouth and limits the maximum improvement possible in the cervicomental angle. A relatively high and posterior hyoid is ideal, allowing maximum elevation of the submental contour and the greatest definition between the submentum and neck in profile. A relatively low and anterior hyoid limits the possible improvement in this area to a predictable degree. It is mandatory, therefore, that hyoid position be assessed and its effects on the possible outcome discussed with the patient in a way that is easily understood. The authors have found the use of diagrams illustrating hyoid position to be very helpful in their practices (Fig. 188.7).
A full evaluation of the facial nerve and muscles should be done preoperatively, particularly noting any asymmetries, especially around the mouth. Sometimes patients have asymmetric smiles or may inadvertently elevate the brow. There may be static asymmetries as well, ranging from minor unilateral cheek or jowl fullness to generalized asymmetry as in hemifacial microsomias. Any asymmetry should be documented, photographed, and discussed with the patient before surgery, or the patient may attribute their asymmetry to the surgery (35). Further, it gives the surgeon the opportunity to
point out that minor asymmetry is normal and that perfect symmetry cannot be a surgical goal. The surgeon also should note any traumatic facial and neck lacerations, sites of previous biopsies, acne scars, facial or neck scars, subcutaneous depressions, surface irregularities, and focal lesions.
point out that minor asymmetry is normal and that perfect symmetry cannot be a surgical goal. The surgeon also should note any traumatic facial and neck lacerations, sites of previous biopsies, acne scars, facial or neck scars, subcutaneous depressions, surface irregularities, and focal lesions.
 Figure 188.4 Excellent candidate for a face-lift: little fat, good bone structure, and not too much skin. |
Generally, the older patient who presents with voluminous sagging skin or the patient with a fat face and neck would not be as good a candidate as the thinner 40- to 50-year-old patient because postoperative skin re-draping with such excess is less satisfactory, especially if elastosis is present. Such patients should be advised that for a better result, a tuck procedure may be necessary 6 months to 1 year after all the retraction has occurred from the original face-lift (36). If liposis is limited to the submental area, the patient will be a better candidate than one who has a full, rounded face with fat throughout. Liposuction in conjunction with a face-lift exerts its maximal effect in the submental area.
Similarly, if a patient contemplates a weight loss of more than 10 pounds, it may be better to postpone surgery until afterward. The authors discourage patients who have a history of repeated weight gain and loss from considering face-lift surgery because repeated stretching of the facial skin may cause a premature return of skin laxity.
Smoking history is also particularly relevant. Rees and Aston (37) noted that smokers have 12 times greater risk of skin slough than nonsmokers, possibly secondary to vasoconstriction, and also have a higher incidence of hematoma formation. Postoperative coughing may contribute to this complication. Smoking has long-term effects on the skin that cannot be completely erased by simple cessation perioperatively. If the patient stops smoking for 1 month before and after surgery, many potential complications associated with smoking can be limited. However, even with smoking cessation 1 month prior to surgery, superficial epidermolysis in the preauricular area is not infrequent. Moreover, these patients very likely would be better candidates for a deep plane face-lift in order to limit these possible complications.
 Figure 188.5 Postoperative views of same patient after face-lift and upper eyelid blepharoplasty. |
Patients with a history of excessive alcohol intake may have characteristic nutritional or liver deficiencies that may lead to poor surgical healing. They also may be uncooperative in the perioperative period, when alcohol consumption is not allowed. Be alert for physical findings associated with excessive alcohol use and hepatic insufficiency.
PREOPERATIVE PREPARATION
Full-disclosure informed consent for surgery and photographs are obtained. The patient is given a packet that includes preoperative and postoperative instructions and a
description of what to expect during recovery. Having the patient fill all prescriptions in advance serves two purposes: It removes the distraction of a rushed visit to the pharmacy for the patient and caretakers in the early postoperative period when even simple things can be difficult. Also, it allows the patient to take antibiotics the night before surgery to assist in preventing infection and provides the patient with sedatives should sleep be difficult the night before surgery.
description of what to expect during recovery. Having the patient fill all prescriptions in advance serves two purposes: It removes the distraction of a rushed visit to the pharmacy for the patient and caretakers in the early postoperative period when even simple things can be difficult. Also, it allows the patient to take antibiotics the night before surgery to assist in preventing infection and provides the patient with sedatives should sleep be difficult the night before surgery.
 Figure 188.6 A less-than-ideal candidate for a face-lift: excessive skin and fat and rounded bony contours. |
 Figure 188.7 Schematic representation of the limits of improvement in the cervicomental contour imposed by the underlying hyoid bone and suprahyoid musculature. A high posterior hyoid is most favorable for face-lifting (A), and a low anterior hyoid is least favorable (B); most patients fall somewhere in between (C). (Reprinted from Conley J. Face-lift operation. Springfield, IL: C. Thomas, 1968:40-41, with permission.) |
The patient is urged to stop smoking 1 month prior to surgery. All medications containing aspirin, steroids, nonsteroidal anti-inflammatory agents, and vitamin E, as well as all herbal medications, should be discontinued at least 2 weeks before surgery. If there is a history consistent with a bleeding diathesis, however tenuous, preoperative bleeding time, platelet count, prothrombin time, and partial thromboplastin time or other coagulation studies should be ordered. The goal is avoidance of hematoma, the most common complication of rhytidectomy.
SURGICAL PLANNING
Successful face-lift surgery is achieved through thoughtful planning and execution of every aspect of the procedure (38). The amount of actual skin excised, the tightness and completeness of the lift in the cheeks, the ability to contour and resuspend the neck, the smoothness of the submental region, and the degree to which the incisions can be camouflaged all are important considerations in achieving a natural, nonoperated appearance. Rhytidectomy is an operation of compromises.
Anesthesia
The authors prefer to perform face-lifts with the patient under general anesthesia in a hospital ambulatory setting or outpatient surgical center (39). Many patients prefer the idea of complete somnolence and amnesia and are relieved of any anxiety concerning positional discomfort or surgical pain. The presence of an anesthesiologist permits monitoring of the patient’s vital signs and status and allows the surgeon to concentrate on the events in the operative field. Communicating any special needs with the anesthesia professionals greatly facilitates the entire operative and postoperative course. The draped endotracheal tube can be moved side to side and does not interfere with the procedure. The anesthesia team strives for rapid, effective anesthesia with a smooth and deep emergence phase coupled with a relatively rapid recovery. Smooth extubation must be guaranteed, as bucking on the endotracheal tube may predispose the patient toward hematoma formation. No long-acting muscle-relaxing agents are permitted, to allow proper intraoperative facial nerve monitoring. Pre-dissection infiltration of local anesthesia with epinephrine is utilized for improved hemostasis. The authors prefer to have the patient emerge from anesthesia after the dressing is in place: this seems to facilitate dressing placement and allows optimal gentle pressure on the skin flaps to decrease the risk of hematoma formation further.
Marking
With the patient in the sitting position, the surgeon better appreciates the descended tissues and the effects of gravitational forces. This helps prevent judgmental errors regarding the amount of fat removal, the degree of laxity, and the amount of SMAS suspension required (40




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
