Rhinoplasty: Incisions, Approaches and Analysis
Grant S. Gillman
A thorough and thoughtful approach to nasal analysis is the foundation upon which a successful aesthetic and functional rhinoplasty outcome is built. A consistent strategy—routinely applied—will hone one’s analysis skills and minimize the likelihood of failing to address something that should have been recognized preoperatively. By studiously engaging in this practice preoperatively and postoperatively, one will come to better appreciate the dynamics of rhinoplasty and the anatomic and surgical correlates of one’s observations and interventions.
No doubt, aesthetic ideals will vary—from patient to patient, from culture to culture, and from surgeon to surgeon (1, 2, 3, 4, 5). Nonetheless, the “guidelines” contained in this chapter are intended to serve as a useful, practical framework upon which to evaluate nasal aesthetics and from which to move forward to surgical planning.
ANATOMIC LANDMARKS
Familiarity with the nomenclature used for the reference points of surface anatomy facilitates improved communication between colleagues and clarity of notes and the operative record. In addition, knowing how underlying structures are reflected on the surface topography enables the surgeon to more accurately analyze, diagnose, and anticipate the pathology and thereby develop a more thoughtful surgical strategy preoperatively. Accordingly, it is appropriate to begin with terminology.
The commonly accepted terms for surface nasal anatomy, as seen from the frontal, lateral, and base views, are illustrated in Figures 180.1, 180.2, 180.3 and defined below. Nasal anatomy is also covered and reviewed in greater detail in the chapter on “Surgical Anatomy of the Nose.”
Terminology
Trichion—the most anterior midline point on the hairline
Glabella—the most anterior or prominent point on the forehead (lateral view)
Nasion (aka radix)—the starting point, root, or visual takeoff of the nose, it is the deepest depression at the root of the nose in the midsagittal plane, corresponding to the nasofrontal suture. The midline junction between the frontal bone and the nasal dorsum is also known as the radix.
Rhinion—the midline junction of the nasal bones and the dorsal septum (osseocartilaginous junction)
Supratip—the point along the nasal dorsum that lies just cephalic to the nasal tip
Tip—the most anterior projecting part of the nasal profile (ideally). The tip “lobule” refers more broadly to the region bounded by the supratip superiorly, the anterior end of the alar crease laterally, and the anterior nostril margin posteroinferiorly.
Infratip lobule—the part of the nasal tip seen from the nasal base view that sits anterior to the columella and leading edge of the nares and extends to the tip-defining point
Soft tissue triangle (or soft tissue facet)—seen from the nasal base, this refers to the soft tissue skin fold that lies anterior to the apex of the nostril and just behind the caudal border of the junction of the medial and lateral crus of the lower lateral cartilage
Subnasale—midline junction of the columella and upper lip
Labrale superioris—the vermilion border of the upper lip
Stomion—the midline point at the junction of the upper and lower lips
Pogonion—the most anterior or prominent point on the chin (lateral view)
Menton—the lowest midline point on the chin
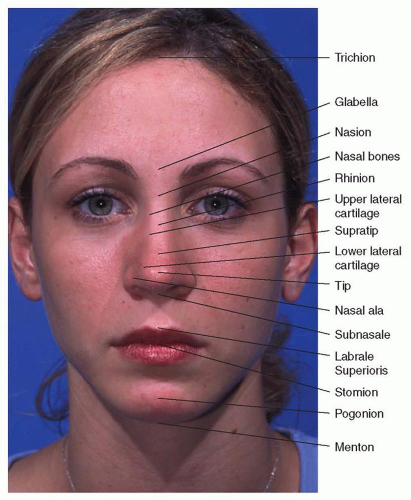 Figure 180.1 Surface anatomy nomenclature— frontal view. |
 Figure 180.2 Surface anatomy nomenclature—lateral view. |
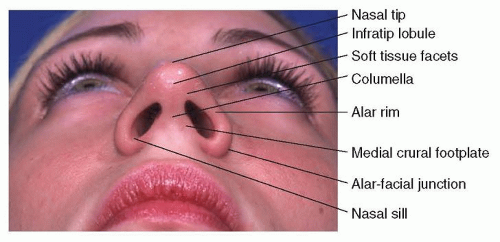 Figure 180.3 Surface anatomy nomenclature—base view. |
NASAL AND FACIAL ANGLES
The most commonly referenced angles applied to nasal analysis are the nasofrontal angle, the nasofacial angle, and the nasolabial angle. Collectively these generate information on features that have some bearing on nasal-facial proportion such as tip rotation, tip projection, and nasal length, and they are very useful when evaluating the nasal profile.
The nasofrontal angle (Fig. 180.4) is the angle measured between a line extending from the glabella through the nasion and a second line drawn from the nasion through the nasal tip-defining point. The ideal nasofrontal angle ranges from 115 to 135 degrees. The deepest point of the nasofrontal angle is known as the nasion (or radix). Perhaps more important than the actual angle measurement itself, the position (superior vs. inferior) and depth of the nasofrontal angle and nasion have significant bearing
on the overall aesthetics and proportion of the nose as it relates to the rest of the face. This is discussed in greater detail in the section on nasal analysis.
on the overall aesthetics and proportion of the nose as it relates to the rest of the face. This is discussed in greater detail in the section on nasal analysis.
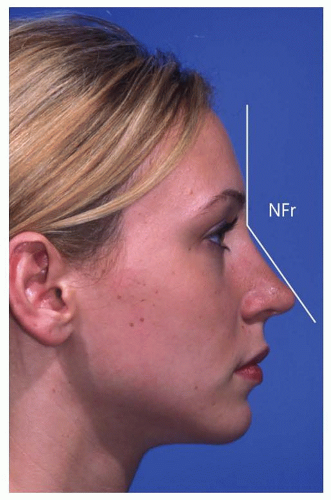 Figure 180.4 Nasofrontal angle—the normal angle measures 115 to 135 degrees. |
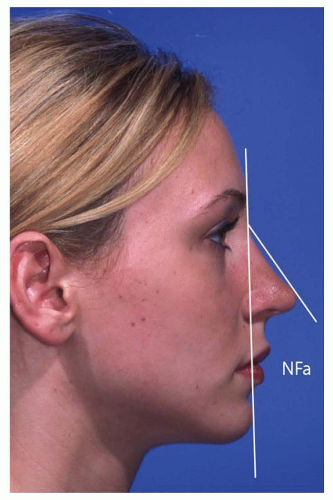 Figure 180.5 Nasofacial angle—the normal angle measures 30 to 40 degrees. |
The nasofacial angle (Fig. 180.5) is formed by a line from the glabella through the pogonion, intersecting with a line from the nasion through the nasal tip-defining point. The ideal nasofacial angle ranges from 30 to 40 degrees (ideal 36 degrees). A larger (more obtuse) angle reflects a relative increase in tip projection whereas the nasal tip would appear less projected with a more acute nasofacial angle.
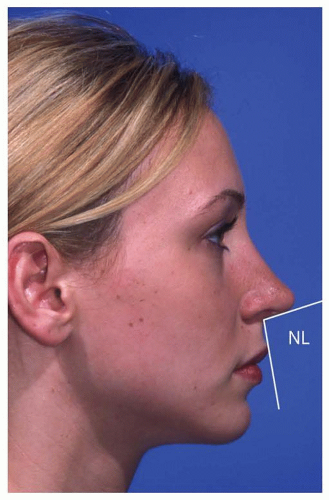 Figure 180.6 Nasolabial angle—the normal angle measures 90 to 115 degrees. |
The nasolabial angle (Fig. 180.6) is the angle formed between the upper lip (from subnasale to labrale superioris) and the plane of the columella through the subnasale. The ideal nasolabial angle ranges from 90 to 115 degrees. Males typically have a more acute nasolabial angle (90 to 105 degrees) consistent with less tip rotation, while the ideal nasolabial angle in females ranges from 100 to 115 degrees in keeping with more tip rotation.
SURGICAL INCISIONS AND APPROACHES
An important distinction is made between surgical approaches and incisions.
A surgical approach refers to the means of exposing the structures of interest. The approach that is chosen will then dictate the incisions that are used to enable that approach. The surgical approach chosen for nasal surgery will vary with the training, comfort level, experience, and preference of the operating surgeon as well as the complexity of the case. While there are a variety of surgical approaches and the preferred approach may vary from surgeon to surgeon, as a general rule, the more severe or complicated the nasal deformity in question, the more likely the surgeon is to benefit from broader exposure.
Surgical approaches can be broadly categorized into external or endonasal approaches. Endonasal approaches can be subdivided into approaches to the nasal dorsum, the nasal septum, or the nasal tip, and endonasal tip approaches can then be further divided into delivery and non-delivery approaches (Fig. 180.7).
Although no absolute indication exists for either an external or endonasal approach and multiple factors will play into the choice of the operating surgeon as noted earlier, a reasonable set of guidelines for each, which may be of benefit to the less experienced surgeon, is outlined in Table 180.1.
Incisions
Surgical incisions are made to facilitate surgical exposure, but the incisions in and of themselves, properly made, have little or no impact on the ultimate dorsal contour, tip shape, or septal position. The surgical incisions most commonly used or referred to in the literature include
The marginal (aka infracartilaginous) incision (Fig. 180.8)—an incision of variable length made along the caudal margin of the lower lateral cartilage. It may be along the caudal border of the lateral crus only in certain
circumstances, the medial crus only, or along the entire caudal edge of the lateral crus.
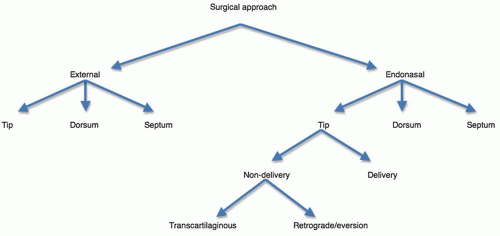
Figure 180.7 Surgical approaches to the nose.
The transcolumellar incision (Fig. 180.8)—an incision made transversely across the short axis (width) of the columella, joining bilateral marginal incisions at its lateral end to facilitate the external approach to the nose. It is typically sited over the medial crura about midway back along the columella and is generally irregularized (nonlinear) in some fashion for better camouflage and less scar contracture.
The intercartilaginous incision (Fig. 180.8)—an incision made at the junction of the caudal border of the upper lateral cartilage and the cephalic border of the lower lateral cartilage (hence “inter”-cartilaginous). Alone it can provide access to the upper two-thirds of the nasal vault (bony and cartilaginous dorsum, nasal sidewall) as well as retrograde access to the lateral crura of the lower lateral cartilages. When combined with marginal incisions, it allows the surgeon to release and “deliver” the lower lateral cartilage as a bipedicled chondrocutaneous flap, pivoting inferiorly in a bucket-handle fashion to enable tip contouring in endonasal rhinoplasty using a delivery approach.
TABLE 180.1 GUIDELINES FOR SELECTION OF SURGICAL APPROACH
Endonasal Rhinoplasty
External Approach Rhinoplasty
Dorsal reduction

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access
