Retinal Vascular Disease
Gary C. Brown
Cotton-Wool Spots
Cotton-wool spots describe the retinal change resulting from acute blockage of blood flow within a terminal retinal arteriole.
Epidemiology and Etiology
The prevalence is uncertain. Cotton-wool spots are seen in over 40% of cases of diabetic retinopathy and also with acute systemic arterial hypertension.
No hereditary pattern is known.
Pathophysiology
Embolic
Hypertensive arteriolar necrosis
Inflammatory
See Diagnostic Evaluation below
Clinical Signs
Visual acuity: Central visual acuity is usually unaffected, although patients may note the sudden appearance of corresponding blind spots.
Pupillary changes: An afferent pupillary defect is usually absent.
Fundus changes: Cotton-wool spots appear in the posterior pole of the fundus (not the peripheral retina) as superficial areas of retinal opacification that characteristically measure less than one quarter disc area in size (Fig. 4-1). When associated with diabetes mellitus, systemic arterial hypertension, and retinal venous obstruction, they are generally seen concomitantly with retinal hemorrhages. Cotton-wool spots usually resolve over 5 to 7 weeks but may remain longer when present in conjunction with diabetic retinopathy.
Differential Diagnosis
Inflammatory retinitis may occur from entities such as toxoplasmosis or cytomegalovirus.
Retinal hemorrhages are typically present with the latter.
There are also usually vitreous cells present with inflammatory conditions, but not with cotton-wool spots alone.
Diagnostic Evaluation
Intravenous fluorescein angiography is minimally helpful. It reveals areas of relative hypofluorescence corresponding to the cotton-wool spots.
Systemic workup (similar to that of acute central retinal artery obstruction, unless the obvious causes of diabetic retinopathy, systemic arterial hypertension, and retinal venous obstruction are present):
Diabetic retinopathy: Cotton-wool spots are present in 44% of cases.
Systemic arterial hypertension: Diastolic blood pressure of 105 to 110 mm Hg or more is usually necessary to induce cotton-wool spot formation in adults.
Retinal vein obstruction: Central, branch.
Embolic: Carotid and cardiac.
Inflammatory: Giant cell arteritis, Wegener’s granulomatosis, polyarteritis nodosa, systemic lupus erythematosus, scleroderma, orbital mucormycosis, toxoplasmosis retinitis.
Coagulopathies: Sickle cell disease, homocysteinuria, lupus anticoagulant syndrome, protein S deficiency, protein C deficiency, antithrombin III deficiency, and the factor V Leiden mutation.
Miscellaneous: Migraine, Lyme disease, hypotension, acquired immunodeficiency syndrome (AIDS), interferon therapy, metastatic carcinoma, intravenous drug abuse (chronic), papilledema, acute pancreatitis, severe anemia, radiation retinopathy, leptospirosis, Purtscher’s retinopathy.
Prognosis and Management
The visual prognosis for central vision is good unless there are innumerable cotton-wool spots as with entities such as systemic lupus erythematosus, pancreatitis, Purtscher’s retinopathy, or intravenous drug abuse. Associated damage from entities that cotton-wool spots accompany (e.g., diabetic retinopathy or retinal venous obstruction) can lead to severe visual loss.
There is no consistently proven treatment to ameliorate the visual acuity. When known diabetic retinopathy and retinal vein obstruction are excluded as causes, a serious associated systemic disease can be found in 95% of cases. Thus, it is critical to undertake a systemic workup if there is no appreciable underlying cause, even if only one cotton-wool spot is present.
 Figure 4-1. Cotton-wool spots. Multiple cotton-wool spots (inset) in the fundus of a patient with human immunodeficiency virus (HIV) infection. |
Hypertensive Retinopathy
Hypertensive retinopathy refers to the retinal vascular changes associated with systemic arterial hypertension. Hypertensive choroidopathy may also accompany the acute phases of hypertensive retinopathy. Blood pressure can vary throughout the day, as can coverage with hypertensive medications. Thus, having a patient measure blood pressure at home three times a day for 3 to 4 days gives the clinician and the patient greater confidence that the blood pressure is either stable or not.
Epidemiology
Hypertensive retinopathy can be divided into chronic and acute phases. The most commonly used classification is the Keith–Wagener–Barker classification. The grades of hypertensive retinopathy are as follows:
Grade 1: Retinal arterial narrowing (Fig. 4-2)
Grade 2: Retinal arteriovenous nicking (Fig. 4-3)
Grade 3: Retinal hemorrhages, cotton-wool spots, hard exudates (Fig. 4-4)
Grade 4: Grade 3 changes plus optic disc swelling (Fig. 4-5)
Grades 1 and 2 are commonly seen in practice. Grade 3 and 4 changes are much less frequently seen.
Pathophysiology
Grades 1 and 2: Hyalinization and thickening of the retinal arterial walls is seen, leading to the straightened vessels in grade 1 and the indentation (arteriovenous nicking) of the retinal veins by the arteries in grade 2 hypertensive retinopathy. Arteriovenous nicking of a retinal vein does not occur at an arteriovenous crossing unless the retinal artery is located anterior to the retinal vein, a phenomenon which occurs in approximately two-thirds of the arteriovenous crossings in the posterior pole.
Grade 3: The systemic diastolic blood pressure in an adult with grade 3 hypertensive retinopathy is typically at least 105 to 110 mm Hg. At this point, the retinal arteries lose their ability to autoregulate the blood flow, and the high pressure is passed distally to the retinal arterioles and capillary bed. This same clinical signs can be seen in children when the systolic blood is in the nineties.
Grade 4: The systemic diastolic blood pressure in an adult with grade 4 hypertensive retinopathy is usually at least 130 to 140 mm Hg. With both grades 3 and 4 hypertensive retinopathy, the increased blood pressure can damage the blood vessel wall, leading to fibrinoid necrosis (the presence of fibrin thrombi within the vascular lumina). A similar process occurs with hypertensive choroidopathy, leading to necrosis of the overlying retinal pigment epithelium (Elschnig spot).
Clinical Signs
Grade 1 and 2 changes are chronic, whereas grade 3 and 4 changes indicate acute retinal vascular decompensation.
Hypertensive choroidopathy (Elschnig spots) may accompany grade 3 and 4 changes. Elschnig spots are round and yellow acutely, eventually changing to pigmented lesions.
Differential Diagnosis
Diabetic retinopathy, radiation retinopathy, venous occlusive disease, carotid artery occlusive disease (ocular ischemic syndrome), and collagen vascular diseases can all mimic the changes of hypertensive retinopathy.
Diagnostic Evaluation
Measurement of the systemic blood pressure is critical when the diagnosis is suspected. If the acute changes (grades 3 and 4) are classic and the blood pressure is not elevated at the time of measurement, consideration should be given to the possibility that the blood pressure has been uncontrolled recently or is uncontrolled at other times during the day.
Prognosis and Management
Vision is typically unaffected with grades 1 and 2 hypertensive retinopathy and may be mildly decreased with grade 3 retinopathy.
With grade 4 retinopathy, vision can be markedly decreased due to retinal edema, hard exudates in the central macula (macular star) and/or the presence of a serous retinal detachment.
The treatment for hypertensive retinopathy is to correct the underlying condition by normalizing the blood pressure. This causes resolution of the fundus abnormalities over a period of weeks to months in eyes with grade 3 and 4 changes, but often does not affect the changes seen with grades 1 and 2 hypertensive retinopathy.
Laser therapy has not been shown to be of benefit in treating the visual loss associated with grade 3 and 4 hypertensive retinopathy. Correcting the blood pressure after grade 4 retinopathy can lead to visual improvement, although there may be residual, permanent visual loss due to vascular shutdown in hypertensive choroidopathy, hypertensive retinopathy, hypertensive optic neuropathy. Oral nifedipine has been suggested for the treatment of acute grade 4 hypertensive retinopathy.
Theoretically, intravitreal VEGF-A inhibitor therapy with ranibizumab and/or bevacizumab could stabilize the walls of retinal of vessels with grade 3 or 4 systemic arterial hypertension changes. As of this writing, data on the treatment of hypertensive retinopathy with these interventions are lacking.
If the blood pressure associated with grade 4 hypertensive retinopathy is untreated, the 18-month mortality rate is 94%.
 Figure 4-2. Hypertensive retinopathy, grade 1. The retinal arteries are markedly narrowed and straightened. Small retinal hemorrhages are present, not due to hypertension but due to background diabetic retinopathy. |
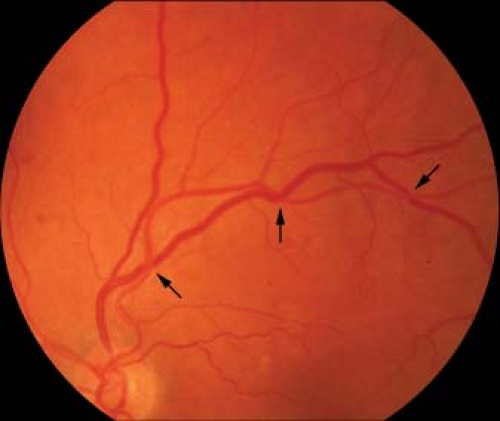 Figure 4-3. Hypertensive retinopathy, grade 2. Prominent arteriovenous nicking (arrows) is seen. Small retinal hemorrhages are present, not due to hypertension, but due to diabetic retinopathy. |
 Figure 4-4. Hypertensive retinopathy, grade 4. Cotton-wool spots, retinal hemorrhages, a macular star composed of intraretinal lipid exudates, and a serous detachment of the macula are all present. The optic nerve head is swollen, the feature that separates grade 3 and grade 4 hypertensive retinopathy. |
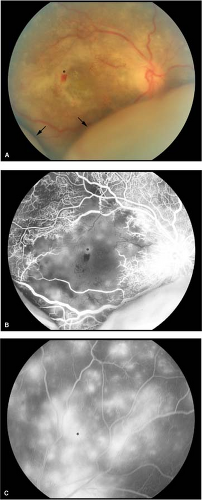 Figure 4-5. Hypertensive retinopathy, grade 4. A. Retinal hemorrhages are present, the optic disc is swollen, and an exudative retinal detachment (arrows) is present inferiorly. Yellow Elschnig spots (asterisk) are present in the macula. B. Fluorescein angiogram corresponding to A. Profound retinal capillary nonperfusion is present in the macula (macular ischemia), and foci of hyperfluorescence corresponding to the Elschnig spots (asterisk) are also seen in the macula. Hypertensive retinopathy, grade 4. C. Fluorescein angiogram of the superior fundus of the eye shown in A. Numerous foci of hyperfluorescence corresponding to Elschnig spots (asterisk) can be seen. |
Cilioretinal Artery Obstruction (Occlusion)
Cilioretinal artery obstruction is the acute blockage of blood flow within a cilioretinal artery.
Epidemiology and Etiology
Cilioretinal artery obstruction typically occurs in patients aged 65 years and older but can be seen at any age.
It is seen in approximately 1:100,000 outpatient ophthalmology visits.
The abnormality is unilateral in over 99% of cases. No hereditary pattern is known.
Pathophysiology
Embolic
Hypertensive arterial necrosis
Inflammatory (e.g., giant cell arteritis)
Hemorrhage under an atherosclerotic plaque
Associated with central retinal vein obstruction
Clinical Signs
Visual acuity: Generally, there is a history of acute, unilateral, painless visual field loss occurring over several seconds. Approximately 10% of those affected have a history of transient visual loss (amaurosis fugax) in the affected eye prior to the central retinal arterial obstruction.
Pupillary changes: An afferent pupillary defect may present immediately, depending on the area of distribution of the obstruction.
Fundus changes: Three variants occur:
Cilioretinal artery obstruction alone (Fig. 4-6): Superficial retinal whitening, usually located within the papillomacular bundle, but which may take hours to develop
Cilioretinal artery obstruction associated with central retinal vein obstruction
Cilioretinal artery obstruction associated with acute anterior ischemic optic neuropathy (Fig. 4-7): Must be particularly concerned about underlying giant cell arteritis
Retinal intra-arterial emboli: Prevalence is uncertain.
Cholesterol (Hollenhorst plaque named after Robert Hollenhorst at the Mayo Clinic): Glistening yellow and typically arises from the carotid arteries. The most likely scenario follows:
Atherosclerosis causes turbulent flow.
Turbulence causes damage to the carotid endothelium.
Plaque is dislodged from the underlying, exposed carotid atherosclerosis. The plaque travels to lodge in the central retinal artery or branch retinal artery.
A fibrin–platelet thrombus may or may not be the nidus for the development of a platelet–thrombin. Thus, a larger embolus may cause a more severe occlusion.
Eventually, the endothelium repairs the damage and the plaque is not exposed to blood.
Turbulence
Calcific: Large, white plaque generally originating from the cardiac valves
Fibrin–platelet: Longer and dull white; may originate from the carotids or cardiac valves
Differential Diagnosis
Inflammatory retinitis from entities such as toxoplasmosis or cytomegalovirus. Retinal hemorrhages are typically present with the latter.
There are also usually vitreous cells present with inflammatory conditions but not with acute cilioretinal artery obstruction.
Diagnostic Evaluation
Intravenous fluorescein angiography: Cilioretinal arteries normally fill with fluorescein dye during the early choroidal filling phase of a fluorescein angiogram. A cilioretinal artery obstruction typically shows nonperfusion of dye in the affected vessel through the retinal arteriovenous phase.
Systemic workup: This is similar to that of acute central retinal artery obstruction.
Emboli: Carotid and cardiac
Inflammatory: Giant cell arteritis, Wegener’s granulomatosis, polyarteritis nodosa, systemic lupus erythematosus, orbital mucormycosis, toxoplasmosis retinitis
Coagulopathies: Sickle cell disease, homocystinuria, lupus anticoagulant syndrome, protein S deficiency, protein C deficiency, antithrombin III deficiency
Miscellaneous: Fibromuscular hyperplasia, Sydenham’s chorea, Fabry’s disease, migraine, Lyme disease, hypotension
Prognosis and Management
With isolated cilioretinal artery obstruction, 90% of eyes return to 20/40 vision or better. With central retinal vein occlusion, 70% of eyes return to 20/40 vision or better. With anterior ischemic optic neuropathy, vision often remains counting fingers to hand motions.
There is no consistently proven treatment to ameliorate the visual acuity. Because of the relatively good prognosis for central vision, digital massage and anterior chamber paracentesis are not typically undertaken.
Despite the lack of an effective ocular treatment, a systemic workup should be undertaken. Although giant cell arteritis likely only accounts for 1% to 2% of cases, the possibility should be actively investigated because the fellow eye can be involved by retinal arterial obstruction within hours to days.
 Figure 4-6. Cilioretinal artery obstruction. Isolated cilioretinal artery obstruction. Note the retinal whitening indicating ischemic retinal edema (inset). |
 Figure 4-7. Cilioretinal artery obstruction and ischemic optic neuropathy. Cilioretinal artery occlusion associated with anterior ischemic optic neuropathy. Note the associated disc edema and pallor. |
Branch Retinal Artery Obstruction (Occlusion)
Branch retinal artery obstruction is the acute blockage of blood flow within a branch retinal artery.
Epidemiology and Etiology
Branch retinal artery obstruction typically occurs in patients aged 65 years and older but can be seen at any age.
It is seen in approximately 1:15,000 to 20,000 outpatient ophthalmology visits.
The abnormality is unilateral in 99% of cases. No hereditary pattern is known.
Pathophysiology
Embolic
Hypertensive arterial necrosis
Inflammatory (e.g., giant cell arteritis)
Hemorrhage under an atherosclerotic plaque
Clinical Signs
Visual acuity: Generally, there is a history of acute, unilateral, painless visual field loss occurring over several seconds. Approximately 10% of those affected have a history of transient visual loss (amaurosis fugax) in the affected eye.
Pupillary changes: An afferent pupillary defect may present immediately, depending on the area of distribution of the obstruction.
Fundus changes: Superficial retinal whitening (Fig. 4-8A) can take hours to develop. Retinal intra-arterial emboli (prevalence uncertain):
Differential Diagnosis
Inflammatory retinitis may occur from entities such as toxoplasmosis or cytomegalovirus. Retinal hemorrhages are typically present with the latter.
There are also usually vitreous cells present with inflammatory conditions but not with acute branch retinal artery obstruction.
Diagnostic Evaluation
Intravenous fluorescein angiography: Reveals a delay in retinal arterial and venous filling in the area of obstruction versus the normal remaining fundus (see Fig. 4-8A). There may be staining of the ischemic retinal vasculature (see Fig. 4-8C).
Systemic workup: This is similar to that of acute central retinal artery obstruction.
Embolic: Carotid and cardiac
Inflammatory: Giant cell arteritis, Wegener’s granulomatosis, polyarteritis nodosa, systemic lupus erythematosus, orbital mucormycosis, toxoplasmosis retinitis
Coagulopathies: Sickle cell disease, homocysteinuria, lupus anticoagulant syndrome, protein S deficiency, protein C deficiency, antithrombin III deficiency
Miscellaneous: Fibromuscular hyperplasia, Sydenham’s chorea, Fabry’s disease, migraine, Lyme disease, hypotension
Prognosis and Management
Most patients improve to 20/40 or better vision without treatment, although a field defect corresponding to the area of obstruction usually persists.
There is no consistently proven treatment to ameliorate the visual acuity. Because of the relatively good prognosis for central vision, digital massage and anterior chamber paracentesis are not typically undertaken.
Despite the lack of an effective ocular treatment, a systemic workup should be undertaken. Although giant cell arteritis likely only accounts for 1% to 2% of cases, the possibility should be actively investigated because the fellow eye can be involved within hours to days.
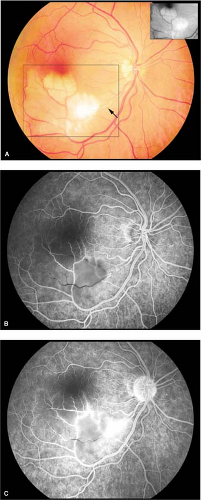 Figure 4-8. Branch retinal artery obstruction. A. Retinal whitening (inset) due to branch retinal artery obstruction. Note the proximal intra-arterial platelet fibrin thrombus (arrow). Branch retinal artery obstruction. B. Fluorescein angiogram corresponding to A reveals retinal arteriolar and capillary nonperfusion in the distribution of the occluded vessel. C. Staining of the inferotemporal branch retinal artery is present in the area of occlusion. |
 Figure 4-9. Branch retinal artery obstruction, calcific plaque. Intra-arterial calcific plaque (arrow) associated with branch retinal artery occlusion. |
Central Retinal Artery Obstruction (Occlusion)
Central retinal artery obstruction is the acute blockage of blood flow within the central retinal artery.
Epidemiology and Etiology
Central retinal artery obstruction typically occurs in patients aged 65 years and older but can be seen at any age.
It is seen in approximately 1:10,000 outpatient ophthalmology visits.
The abnormality is unilateral in 99% of cases.
No hereditary pattern is known.
Pathophysiology
Embolic
Hypertensive arterial necrosis
Dissecting aneurysm within the central retinal artery
Inflammatory (e.g., giant cell arteritis)
Hemorrhage under an atherosclerotic plaque
Vasospasm
Clinical Signs
Visual acuity: Generally, there is a history of acute, unilateral, painless visual loss occurring over several seconds. Approximately 10% of those affected have a history of transient visual loss (amaurosis fugax) in the affected eye.
Pupillary changes: An afferent pupillary defect is usually present immediately.
Fundus changes
Superficial retinal whitening: Can take hours to develop
Cherry red spot in the foveola (Fig. 4-10)
Cilioretinal arterial sparing of central fovea (Fig. 4-11): Present in 10% of cases
Retinal intra-arterial emboli: Present in 20% of cases
Cholesterol (Hollenhorst plaque): Glistening yellow (Fig. 4-12) and typically originates from the carotid arteries
Calcific: Large, white plaque generally originating from the cardiac valves
Fibrin–platelet: Longer and dull white; may originate from the carotids or cardiac valves (see Fig. 4-8A)
Differential Diagnosis
Acute ophthalmic artery obstruction (cherry red spot absent)
Tay–Sach’s disease (cherry red spot present, but in infants less than 1 year of age and with severe neurologic dysfunction)
Diagnostic Evaluation
Intravenous fluorescein angiography: Reveals delay in retinal arterial and venous filling (normally, the vein of the temporal vascular arcade should completely fill within 11 seconds after dye enters the corresponding retinal arteries.
Electroretinography: Normal a-wave amplitude, but diminished b-wave amplitude.
Systemic workup
Embolic: Carotid and cardiac
Inflammatory: Giant cell arteritis, Wegener’s granulomatosis, polyarteritis nodosa, systemic lupus erythematosus, orbital mucormycosis
Coagulopathies: Sickle cell disease, homocysteinuria, lupus anticoagulant syndrome, protein S deficiency, protein C deficiency, antithrombin III deficiency
Miscellaneous: Fibromuscular hyperplasia, Sydenham’s chorea, Fabry’s disease, migraine, Lyme disease, hypotension
Vasospastic: Migraine
Prognosis and Management
The visual prognosis is typically poor, with most patients retaining counting finger to hand motions vision and a small temporal island of vision remaining. If a cilioretinal artery spares the central fovea, 80% of eyes will return to 20/20 to 20/50 vision over a period of 2 weeks. Nevertheless, in the latter instance there is typically severe visual field loss. Approximately 18% of eyes will progress to develop iris neovascularization within 4 to 6 weeks after the acute obstruction.
There is no consistently proven treatment to ameliorate the visual acuity. Digital massage of the globe and anterior chamber paracentesis has been advocated but has minimal benefit. Treatment with fibrinolytic agents is still considered investigational.
Despite the lack of a consistently effective ocular treatment, a systemic workup should be undertaken. Although giant cell arteritis likely only accounts for 1% to 2% of cases, the possibility should be actively investigated because the fellow eye can be involved within hours to days. In regard to systemic workup, it should be noted that patients with acute central artery obstruction have a high death rate from cardiac vascular disease.
If iris neovascularization develops, laser panretinal photocoagulation (PRP) should be considered to help prevent neovascular glaucoma. It causes resolution of the new iris vessels in approximately two-thirds of the treated cases.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


