Age-Related Macular Degeneration
Allen C. Ho
Age-related macular degeneration (AMD) describes a common degenerative condition of the retina that may affect central vision. By definition, it occurs in individuals 50 years and older and is more prevalent with increasing age. Population-based surveys in the Western world vary but estimate the prevalence of AMD to be approximately 10% to 35% in individuals over the age of 50 years. AMD is divided into “dry” or nonexudative AMD and “wet” or exudative AMD.
Dry or Nonexudative Age-Related Macular Degeneration
Drusen are the clinical hallmark of dry AMD. They are subretinal pigment epithelial deposits between the basement membrane of the retinal pigment epithelium (RPE) and Bruch’s membrane (Figs. 1-1 and 1-2) or within Bruch’s membrane itself. Multiple types of drusen have been described, including large drusen (greater than 64 μm); small drusen (63 μm or smaller); calcified drusen, which are yellow and glistening; and basal laminar drusen, which are small round diffuse drusen that are more apparent on fluorescein angiography than on clinical fundus examination (Fig. 1-3). Multiple large drusen are representative of a diffuse thickening of Bruch’s membrane. Large drusen, also known as soft drusen, are a risk factor for more advanced AMD and vision loss. Small (also known as hard) drusen alone do not increase the risk for more advanced forms of AMD (Fig. 1-4).
Retinal pigment epithelial abnormalities, including nongeographic atrophy, focal hyperpigmentation, and frank geographic atrophy, are also common fundus features of dry AMD (Fig. 1-5). Granularity of the RPE may be an early feature of retinal pigment epithelial disturbance due to AMD. This may progress to areas of nongeographic atrophy (Fig. 1-6) in which there is loss of pigment of the RPE, but this is not discrete, and underlying choroidal vessels are not apparent. Geographic atrophy comprises discrete loss of RPE in a so-called cookie-cutter fashion with a minimal diameter of 250 μm
associated with underlying loss of choroidal stromal pigment and clearly visible underlying larger choroidal vessels (Fig. 1-7).
associated with underlying loss of choroidal stromal pigment and clearly visible underlying larger choroidal vessels (Fig. 1-7).
Epidemiology and Etiology
Drusen are seen increasingly with advancing age and typically are present in the sixth decade of life or later. Population-based studies estimate approximately 10% prevalence of early AMD (drusen) in the fifth decade of life, increasing to 35% in the seventh decade. Drusen may be seen in younger patients and may be heritable in these cases.
The precise source of drusen material is not completely understood, but they are thought to represent degenerative products of retinal pigment epithelial cells; they are composed of lipids and glycoproteins, and may be mineralized. Retinal pigment epithelial alterations are seen increasingly with age and are common in the seventh, eighth, and ninth decades of life.
Pathology
Transmission electron microscopy of eyes with drusen and dry AMD shows two types of deposits:
Basal laminar deposits consist of wide-spaced collagen localized between the retinal pigment epithelial plasma membrane and the retinal pigment epithelial basement membrane.
Basal linear deposits consist of lipid-rich material external to the basement membrane of the RPE in the inner collagenous zone of Bruch’s membrane.
History
Patients with drusen may be visually asymptomatic. Patients with multiple drusen and associated retinal pigment epithelial abnormalities including granularity of the RPE, atrophy of the RPE, or focal hyperpigmentation will often note fluctuating vision, including central blurring. They typically will describe a need for increased light intensity in order to read and have difficulty adapting between different lighting.
Patients with dry AMD and without evidence of geographic atrophy of the RPE or exudative AMD typically have good central vision between 20/20 and 20/60.
Clinical and Fluorescein Angiographic Signs
Fundus biomicroscopy shows subretinal pale yellow deposits that may vary in size from greater than 64 μm (large drusen) to small or hard drusen (63 μm or smaller) in diameter. Calcific drusen have a glistening appearance, and most patients with AMD have a mixture of clinical drusen types. Large drusen will often become confluent into larger drusenoid pigment epithelial detachments. Drusen should be considered fluid and dynamic structures that can appear or resolve over time (Fig. 1-8).
An irregular granular appearance to the RPE is often seen in association with drusen. Areas of nongeographic atrophy or frank geographic atrophy are often appreciated after the spontaneous resolution of drusen and, in particular, drusenoid pigment epithelial detachments. Intraretinal pigment clumps or focal hyperpigmentation represents advanced retinal pigment epithelial degeneration as well.
Fluorescein angiography typically demonstrates a patchy hyper- and hypofluorescence without leakage of dye. Drusen may show early or late hyperfluorescence, depending on the integrity of the overlying RPE and the histochemistry of the drusen themselves. Large soft drusen typically show early
hypofluorescence and late hyperfluorescence (Fig. 1-9). This angiographic pattern is inconsistent, however, because some drusen, even those that are large, will show earlier hyperfluorescence (Fig. 1-10). Geographic atrophy shows discrete hyperfluorescence with stable boundaries throughout the angiogram (Fig. 1-11).
Associated Clinical Signs
When drusen are noted in patients over the age of 50, other features of AMD are often observed, including granularity and atrophy of the RPE. Drusen that are associated with subretinal fluid, hemorrhage, or lipid exudation due to choroidal neovascularization (CNV) are characteristics of exudative AMD.
Differential Diagnosis
Drusen are subretinal and should be distinguished from intraretinal processes such as intraretinal lipid, retinal emboli, and cotton-wool spots. The borders of drusen may be more distinct in smaller hard drusen and less distinct with large drusen.
Other yellow macular lesions can be included in the differential diagnosis of drusen, including the following:
Pattern dystrophy: Presents in younger patients; lesions show geographic shape.
Best’s disease: Round or oval lesions may show different stages.
Adult foveomacular dystrophy: Yellowish green subfoveal lesion; may simulate CNV on fluorescein angiography.
Diagnostic Evaluation
Patients with a sudden change in vision or new blur or distortion of central vision may be evaluated with fluorescein angiography to rule out exudative AMD.
Careful fundus biomicroscopy is important to rule out subtle signs of exudative AMD.
Optical coherence tomography (OCT) is an essential diagnostic tool in the evaluation of AMD patients and can help establish the presence of early exudative AMD and help determine the response to therapy.
Prognosis and Management
Patients with drusen are counseled that they have the dry form of AMD and that most patients with drusen will not develop vision loss due to more advanced forms of AMD (exudative AMD and CNV or geographic atrophy). Patients with multiple large drusen are at a higher risk of developing CNV, particularly if the fellow eye has previously developed exudative AMD (Table 1-1). The 5-year risk of developing CNV in fellow eyes of patients with exudative AMD ranges between 40% and 85%. Management includes counseling regarding the importance of monitoring central vision in each eye with a test object such as the Amsler grid (Fig. 1-12).
Table 1-1. Risk of Choroidal Neovascularization (CNV) for Eyes with Drusen (Fellow Eye with Exudative CNV)
Overall estimate is 10% of patients per year with unilateral drusen will develop CNV. The Macular Photocoagulation Study Group has established risk factors that increase the risk of CNV:
Multiple large drusen
Focal hyperpigmentation
Hypertension
Smoking
Information from the age-related eye disease study (AREDS) demonstrates that micronutrient and antioxidant supplementation (vitamin C, 500 mg; vitamin E, 400 IU; beta carotene, 15 mg; zinc, 80 mg as zinc oxide; and copper, 2 mg as cupric oxide) can effect a modest but definite reduction in clinical progression of AMD and moderate visual loss in patients with dry AMD and at least one large druse of 125 μm or larger. Data were not significant for patients with mild or borderline dry AMD (multiple small drusen or nonextensive intermediate drusen of 63 to 124 μm, pigment abnormalities, or any combination of these).
Patients with focal hyperpigmentation have a higher risk of developing more advanced forms of AMD associated with vision loss and, in particular, CNV. Some believe that this clinical feature may represent a sign of early, ill-defined CNV in many cases. If there is a suspicion of early exudative AMD, then fluorescein angiography and OCT imaging may be performed. Since early retinal pigment epithelial abnormalities and granularity of the RPE may lead to nongeographic atrophy and frank geographic atrophy, they may be harbingers of vision loss.
There are numerous clinical trials investigating potential therapies for dry AMD including other nutritional supplements such as omega 3 fatty acids, lutein and zeaxanthin carotenoids (AREDS 2 Study), visual cycle inhibitors, anti-inflammatory or complement inhibitors and stem cell therapies. An intraocular implantable telescope has been approved for patients with geographic atrophy based on clinical trial evidence.
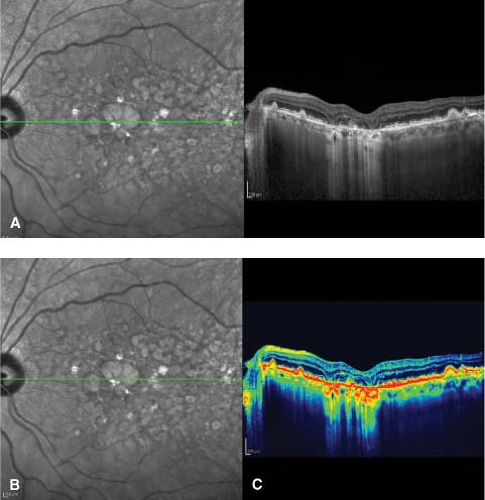 Figure 1-1. Large drusen. A. Fundus photograph demonstrating predominantly large drusen, some of which are confluent (inset). Visual acuity was 20/25. B and C. Red free fundus image and OCT image of drusen at the level of Bruch’s membrane and the retinal pigment epithelium. Note the irregular elevation of the retinal pigment epithelium caused by drusen. |
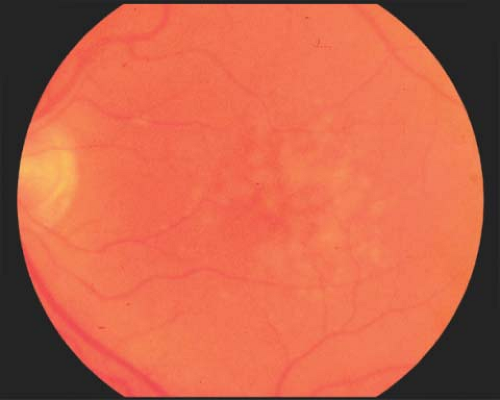 Figure 1-2. Confluent drusen. Fundus photograph demonstrating multiple large, predominantly confluent drusen. Confluence is greatest temporal to the fovea. Confluent drusen are a risk factor for exudative age-related macular degeneration (AMD). |
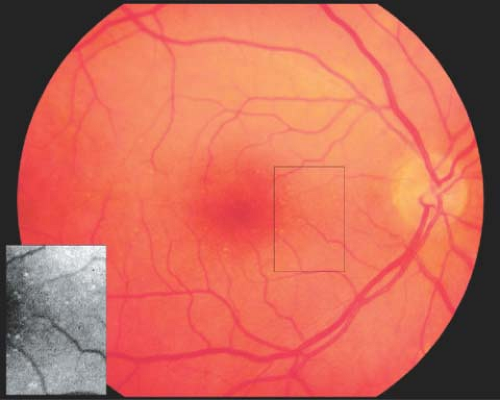 Figure 1-3. Basal laminar drusen. Fundus photograph demonstrating multiple small, round, diffuse drusen (inset) with large areas of confluence in the posterior pole and midperipheral retina. Basal laminar drusen may be more apparent with fluorescein angiography than clinically. |
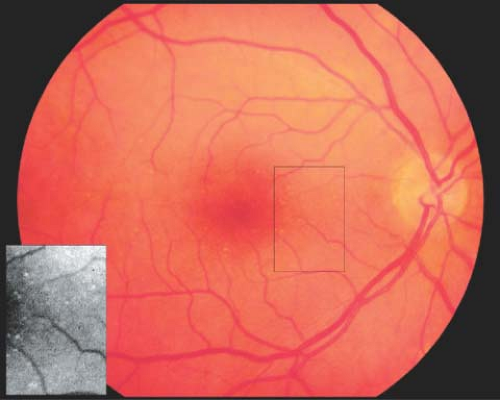 Figure 1-4. Hard drusen. Hard drusen (inset) are small (63 μm or smaller) and are not a risk factor for more advanced forms of AMD. |
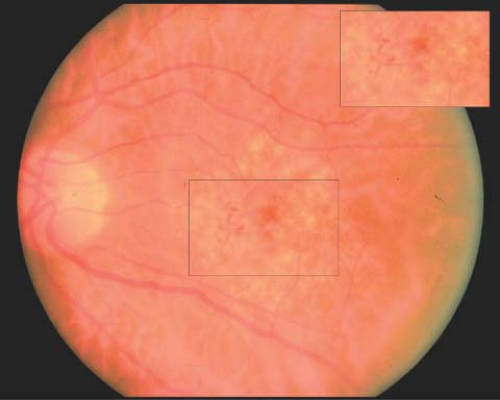 Figure 1-5. Focal hyperpigmentation. Fundus photograph showing multiple drusen with retinal pigment epithelial alterations (inset). Focal hyperpigmentation is noted in the fovea and just nasal to the fovea. Focal hyperpigmentation is a risk factor for more advanced forms of AMD associated with vision loss.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|