(1)
Department of Pathology, Duke University Medical Center, Durham, NC, USA
Abstract
The retina is a complex tissue lining the inner surface of the eye. It receives images from the outside world and transmits signals to the visual cortex in the occipital pole of the brain.
The retina is basically neuroglial tissue, composed of ganglion cells (neurons) and glia (astrocytes within the nerve fiber layer and ganglion cell layer and Müller radial glia which extend from the inner limiting membrane to the outer limiting membrane). Axons from the retinal ganglion cells form the nerve fiber layer which courses posteriorly to become the optic nerve.
This chapter will review the histology of the normal retina and introduce the pathology of some common retinal disorders, the best known of which is retinoblastoma.
The retina is a complex tissue lining the inner surface of the eye. It receives images from the outside world and transmits signals to the visual cortex in the occipital pole of the brain.
Let us begin by reviewing the normal histology of the retina. The retina is basically neuroglial tissue, composed of ganglion cells (neurons) and glia (astrocytes within the nerve fiber layer and ganglion cell layer, and Müller radial glia which extend from the inner limiting membrane to the outer limiting membrane). Axons from the retinal ganglion cells form the nerve fiber layer which courses posteriorly to become the optic nerve.
The retina has two main components:
1.
The neurosensory retina
2.
The retinal pigmented epithelium (RPE)
The histological layers of the neurosensory retina are listed here, from inner to outer; “inner” refers to being closer to the vitreous, and “outer” refers to being closer to the sclera:
Inner limiting membrane
Nerve fiber layer
Ganglion cell layer
Inner plexiform layer
Inner nuclear layer
Outer plexiform layer
Outer nuclear layer
Outer limiting membrane
Photoreceptors (rods and cones)
What Is the Macula, and Why Is It Important?
The macula is where you examine for the pathology of age-related macular degeneration (AMD), the leading cause of blindness in the USA.
The macular region of the retina is located slightly temporal to the optic nerve head, and it can be identified histologically because the ganglion cell layer is more than one cell layer thick (Fig. 6.1). In the peripheral retina, the ganglion cells form a single layer (Fig. 6.2).
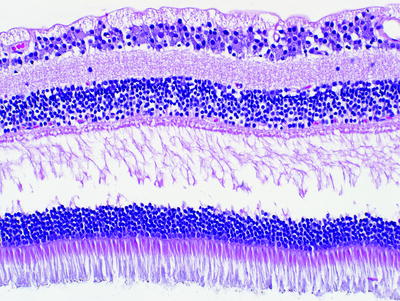
Fig. 6.1
Neurosensory retina showing (from the top of the image to the bottom of the image) the nerve fiber layer, a multilayered ganglion cell layer, the inner plexiform layer, the inner nuclear layer, the outer plexiform layer, the outer nuclear layer, and the photoreceptors. The multilayered ganglion cell layer confirms this as the macular region of the retina
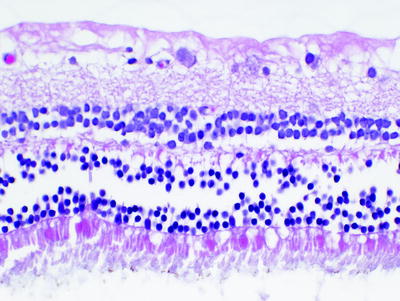
Fig. 6.2
Peripheral retina showing a single layer of ganglion cells
The fovea is the center of the macula; this is where sharp central vision and most color vision occurs because of the high concentration of cone photoreceptors (Fig. 6.3).
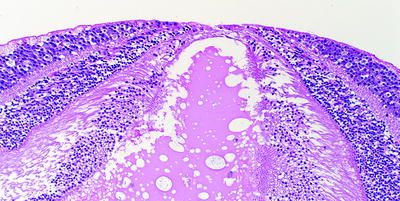
Fig. 6.3
Section through the macula at the region of the fovea. The fovea (top center of the image) is where light travels directly to the photoreceptors with no intervening retinal tissue. In this section, the retina is detached and distorted appearing
The macular region is best seen when the eye is sectioned in the horizontal plane. A fortuitous section is usually needed to visualize the fovea.
Retinal Detachment
A true retinal detachment (Fig. 6.4) can be discerned from a false detachment (Fig. 6.5) by the presence of eosinophilic subretinal fluid. Almost every enucleation specimen will exhibit a false detachment secondary to prosection of the globe.
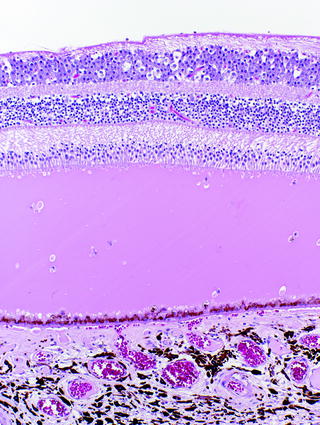
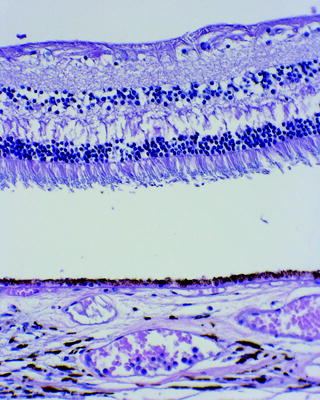
Fig. 6.4
Low-magnification view showing the eosinophilic subretinal fluid in a true retinal detachment. The ganglion cell layer is multilayered, and therefore, this is the macular region. The retinal pigmented epithelium layer and choroid are seen at the bottom of the image
Fig. 6.5
Photomicrograph showing artifactual retinal detachment. There is no subretinal fluid between the detached neurosensory retina and the underlying retinal pigment epithelium and choroid. The RPE is closely apposed to the underlying choroid, in contrast to the buildup of products seen in age-related macular degeneration (compare with Fig’s 6.26–6.29)
What Are Some of the Main Pathologies Involving the Retina?
Neoplastic:
Retinoblastoma
Lymphoma
Hemangioblastoma
Adenomas and adenocarcinomas of the retinal pigment epithelium
Retinoinvasive melanoma
Nonneoplastic:
Age-related macular degeneration (AMD)
Diabetes-related retinopathy
Glaucoma
Cytomegalovirus (CMV) retinitis
Toxoplasmosis retinitis (may also involve the choroid and may be termed retinochoroiditis or chorioretinitis)
Retinitis pigmentosa
Retinoblastoma
Retinoblastoma is the most common intraocular tumor of childhood.
The classic clinical presentation of patients with retinoblastoma is leukocoria.
Leukocoria is an abnormal white reflection seen through the pupil.
Leukocoria is not specific for retinoblastoma and can be seen in other conditions including Coats’ disease, Toxocara endophthalmitis, persistent hyperplastic primary vitreous, cataract, retinopathy of prematurity, and others.
Retinoblastomas may be unilateral or bilateral:
Unilateral tumors are typically sporadic (nonfamilial/noninherited).
Bilateral tumors are typically familial/inherited.
Bilateral familial tumors typically present at a younger age than nonfamilial tumors, and they may present simultaneously or with a time lag.
When prosecting an eye with retinoblastoma, it is important to do two things to evaluate for histopathologic high-risk features (Fig. 6.6):
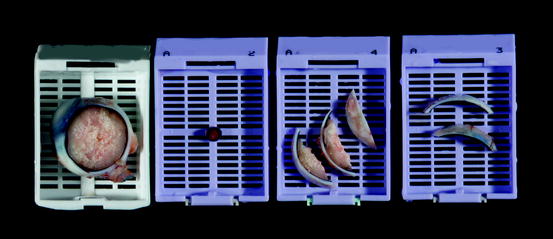
Fig. 6.6
Examination of an eye with retinoblastoma should include (from left to right) the main section of the globe, the optic nerve margin, and the superior and inferior calottes (the calottes are submitted on edge to evaluate for invasion of the choroid by tumor)
1.
Submit the optic nerve margin. Tumor can extend via the optic nerve and subarachnoid space into the orbit and intracranial cavity resulting in metastatic disease of the brain and spinal cord.
2.
Submit the calottes (the side pieces) on edge to evaluate for choroidal invasion.
Then, evaluate and document the following prognostic features:
Get Clinical Tree app for offline access
1.
Does tumor invade into the optic nerve or not (Fig. 6.7)?
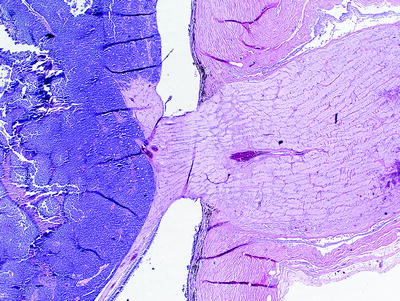




Fig. 6.7
Low-magnification view of retinoblastoma without invasion of the optic nerve
If tumor does invade the nerve, document the relationship of the tumor to the lamina cribrosa (the lamina cribrosa is a sievelike partition at the optic nerve head. Pre-laminar axons from the retinal nerve fiber layer are not myelinated, and post-laminar axons are myelinated).< div class='tao-gold-member'>Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
