Chapter 10 Reoperation for Benign Disease
 This chapter contains additional online-only content, available on expertconsult.com.
This chapter contains additional online-only content, available on expertconsult.com.
Introduction
Benign thyroid disease, either benign nodular goiter or Graves’ disease, is an extremely common endocrine disorder worldwide and affects at least 5% to 7% of the world’s population.1,2 Of these, 10% to 12% will require primary operative intervention3 (see Chapters 7, Surgery of Cervical and Substernal Goiter, and 9, The Surgical Management of Hyperthyroidism). Endocrine surgeons are becoming adept at striking the balance between removing all disease at the initial operation, thereby reducing recurrence rates, while minimizing complications. As a result, recurrent benign thyroid disease is being seen less commonly. However, when it does occur, recurrent thyroid disease represents a significant clinical and surgical challenge. Patients may present with local compressive symptoms, mandating operative intervention. The complication rates of permanent recurrent laryngeal damage and hypoparathyroidism with reoperative surgery are higher than at initial operation; therefore, surgeons must be intimately familiar with the distorted anatomy present at reexploration in an attempt to reduce the incidence of these complications.
This chapter defines the pathogenesis, clinical presentation, and preoperative management, operative strategies, and postoperative management of patients presenting with both recurrent benign nodular goiter and Graves’ disease (see Chapters 7, Surgery of Cervical and Substernal Goiter, and 9, The Surgical Management of Hyperthyroidism).
Prevalence
Palpable recurrence of nontoxic nodular goiter is documented to occur in 0.3% to 42% of patients who have had previous surgery for the same condition.4–7 Operative intervention for recurrence accounts for anywhere between 5% to 25% of all thyroid surgery performed.8,9 However, since the early 1990s there has been a shift away from conservative primary operations such as bilateral subtotal thyroidectomy, and this should begin to be mirrored by declining recurrence rates. Not surprisingly, there appears to be a trend toward longer times to recurrence from the initial surgical intervention. The documented rate of recurrence in our unit is 0.32% following a total thyroidectomy as an initial operation.10
Management of Recurrent Nodular Goiter
• The patient underwent an initial thyroid lobectomy for what was a clinically solitary nodule but final pathology revealed a dominant nodule in a multinodular goiter, and nodular recurrence subsequently developed in the contralateral lobe.
• The patient underwent an initial inadequate resection for nodular goiter. This may have been many decades previously when such minimalist approaches were more acceptable and commonly will have consisted of either a simple nodule excision, a partial lobectomy, or a “front shave” where just the anterior components of each lobe were resected. Subsequently, bilateral nodular change has progressed in what is essentially an intact thyroid gland albeit with some anterior scarring.
• The patient underwent a formal bilateral subtotal thyroidectomy or total lobectomy and contralateral subtotal lobectomy and has now developed recurrent disease in the residual posterior remnant(s).
• The patient has had a “total” thyroidectomy but has developed recurrent disease in one of the embryologic thyroid remnants not recognized at the initial operation.
• The patient has had a complete, meticulous total thyroidectomy but has underlying aggressive, albeit benign, nodular disease and develops nodular recurrence in miniscule remnants of residual tissue. This scenario may occur even with suppressive thyroxine therapy.
The surgical approach to each of these situations is different and will be outlined in this chapter.
Initial Thyroid Lobectomy for a Clinically Solitary Thyroid Nodule
The most common pathology seen in a clinically solitary nodule is, in fact, a dominant colloid nodule in a multinodular goiter. Other pathologies may include the benign follicular adenoma, thyroid cyst, or nodular change in Hashimoto’s thyroiditis. For a clinically solitary nodule, the standard approach is a formal thyroid lobectomy leaving the opposite side intact. Careful selection of patients will, of course, minimize recurrence rates. Patients selected should have predominantly unilateral nodularity with minimal clinical disease evident on the contralateral side. Typically, these patients have a strong aversion to the lifelong use of thyroxine replacement and are therefore willing to accept the associated small risk of recurrence from this type of conservative surgery. In a study from this unit, we demonstrated that among patients who had a hemithyroidectomy for an apparently clinically solitary thyroid nodule that subsequently was shown to be part of a multinodular goiter, only 12% (n = 28/229 patients) required further surgery for recurrent disease.11 Formal hemithyroidectomy therefore appears to be adequate treatment for these patients, as few will require future treatment for a clinically significant recurrence if such patients are selected well. When recurrent nodular goiter does occur, it is important initially to obtain accurate imaging of both sides of the neck. While in expert initial hands, recurrence on the operated side should be close to zero; this needs to be excluded prior to any planned contralateral surgery. Completion thyroidectomy comprising a second thyroid lobectomy on the side with recurrent nodular change has minimal risk of complications. However, it is vital for an indirect laryngoscopy to be performed in all cases of recurrent nodular goiter preoperatively. An undiagnosed, well-compensated, recurrent laryngeal nerve palsy from the initial operation could lead to the disastrous complication of a tracheostomy arising from even a temporary neuropraxia on the second side. Likewise, the approach to the parathyroid glands should mirror that taken in an initial total thyroidectomy, as there is no guarantee, nor any way of ascertaining, if there is any residual parathyroid tissue on the initial operated side.
Initial Inadequate/Atypical Resection for Nodular Goiter
Inadequate or atypical initial operations, such as isthmusectomy, nodule enucleation, or subtotal lobectomy, have been identified as increasing the likelihood of recurrence even where there is an isolated thyroid nodule.5,12,13 In many cases of such inadequate or atypical initial procedures, the operation had been performed several decades ago, at a time where the principal motivation of many surgeons was to avoid complications by staying away from any posterior dissection near the recurrent laryngeal nerves or parathyroid glands. Given this lack of posterior dissection, the surgical approach at revision surgery may well be very straightforward, with virgin tissues posteriorly once the initial anterior scarring has been dissected free. Nonetheless, considerable care is still required throughout the revision procedure until the anatomy has been fully displayed because, in part, of the uncertainty of what was actually undertaken at the initial operation. This uncertainty may remain even after a review of the first operative note, should it be available. Bilateral recurrent nodular goiter should have a formal total thyroidectomy to reduce the chance of yet a further recurrence in any residual tissue left behind with a less than total procedure.
Initial Bilateral Subtotal Procedure for Multinodular Goiter
However, in recent years there have been two evidenced-based reviews and 15 publications offering comparative data between subtotal and total thyroidectomy for benign multinodular goiter,4,8,10,14–25 which challenge these findings. Most of these studies are retrospective in nature and unfortunately vary widely in their definitions regarding primary disease and recurrence, treatment groups, the length of follow-up, and the actual recurrence rates. Comparison is therefore difficult and performing a meta-analysis almost impossible.
However Agarwal et al. concluded that grade B recommendations can be made from the available evidence regarding subtotal thyroidectomies. First, they are associated with an increased risk of recurrence (2.5% to 42%) when compared to a total thyroidectomy. Second, it provides little added safety in terms of recurrent laryngeal nerve damage and permanent hypoparathyroidism, over a total thyroidectomy. Finally, it may leave a small number of incidentally detected carcinomas inadequately treated. The review identified a rate of incidentally detected carcinoma of between 3% and 16.6%.15 Although the majority of these were micropapillary or microinvasive follicular cancers, about a third were clinically significant follicular or papillary cancers. These results were confirmed by Pappalardo’s group from Italy,4 who undertook the largest prospective randomized controlled trial comparing subtotal to total thyroidectomy for multinodular goiter within a single institution. One hundred and forty-one patients were included in the study group. They demonstrated that there was a 14% recurrence rate in the group who underwent a subtotal versus 0% who had a total thyroidectomy at a mean follow-up of 14 years. These rates are consistent with the range of recurrences from the pooled data of the other studies and demonstrate that recurrence following total thyroidectomy is essentially nonexistent.8,10,14–25
The only real argument against total thyroidectomy is the potential for an increased rate of postoperative complications. There is, however, evidence to suggest that with increasing experience, the use of appropriate surgical technique and, most important, the quality training of surgical residents, total thyroidectomy can be performed with minimal complications.26,27 The available evidence does not demonstrate an increased rate of either temporary (1% to 10% versus 0.9% to 6%) or permanent (0% to 1.3% versus 0% to 1.4%) recurrent nerve damage when comparing total thyroidectomy to subtotal.4,19,20,22,23,28–30 Although a total thyroidectomy may have a slightly increased rate of temporary hypoparathyroidism, requiring calcium supplementation, this does not translate into an increase in permanent hypoparathyroidism (see Chapters 45, Pathophysiology of Recurrent Laryngeal Nerve Injury, 46, Management of Recurrent Laryngeal Nerve Paralysis, and 47, Non-Neural Complications of Thyroid and Parathyroid Surgery).
 Please see the Expert Consult website for more discussion of this topic.
Please see the Expert Consult website for more discussion of this topic.
The policy in our unit regarding the management of benign multinodular goiter changed in the early 1980s from a bilateral subtotal thyroidectomy to a total thyroidectomy. At that stage, surgery for recurrent nodular goiter comprised over 25% of the volume of work for the unit. With this change in policy, which was adopted progressively by essentially all thyroid surgeons across Australia, there has been a significant reduction in the number of operations for recurrent disease to less than 5% of the unit’s workload.22
Revision surgery for bilateral nodular recurrence following previous subtotal thyroidectomy can be a significant challenge, more so if an experienced thyroid surgeon performed the initial procedure. Under those circumstances, it is likely that both recurrent laryngeal nerves will have been fully dissected and may well be encased in scar. Likewise any previous formal bilateral subtotal thyroidectomy, if done properly, will have involved the dissection of both the upper and lower poles. Hence, the anatomy of the parathyroid gland blood supply will have been significantly disturbed, and the glands themselves may well be encased in scar tissue. Of more concern, however, is that there is no way of predicting how many parathyroid glands may have been inadvertently removed or devascularized at the initial procedure—the patient may well be maintaining his or her entire parathyroid hormone (PTH) secretion from a single tenuous parathyroid gland located anteriorly in scar tissue on the surface of the residual lobe with recurrent nodular change. Despite these challenges, with care and appropriate technique, bilateral reoperative surgery can be performed safely. In this unit for reoperative bilateral surgery, the complication rate of permanent recurrent laryngeal nerve damage is 0.3% and permanent hypoparathyroidism is 0.6%, respectively.7
Initial “Total” Thyroidectomy but Recurrent Disease in an Embryologic Remnant
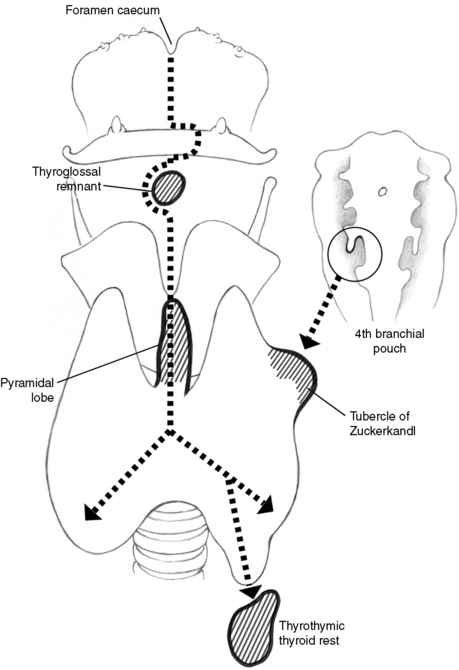
A well-documented source of recurrent benign nodular goiter is embryologic remnants left in situ at the primary operation. Thyroid primordial cells develop from the pharyngeal ectoderm, forming a visible medial anlage by 16 to 17 days of gestation. This diverticulum migrates caudally to reach the level of the cricoid cartilage. During this period it is attached to the base of the tongue by the thyroglossal duct tract (Figure 10-1). By the end of the seventh week, the gland has assumed its adult shape and orthotopic location. At this stage it has lost its communication with the tongue as the thyroglossal duct tract degenerates and the cells begin to express markers of mature thyrocyte differentiation.31,32 There is also contribution to orthotopic thyroid parenchyma derived from lateral embryologic components that contribute to posterior elements known as the tubercle of Zuckerkandl. Although the exact etiology of aberrant thyroid tissue is not clearly defined, it would seem logical that it represents either arrested or excessive descent of the medial or lateral elements of the thyroid along its embryologic path (see Chapter 2, Applied Embryology of the Thyroid and Parathyroid Glands.
 Please see the Expert Consult website for more discussion of this topic.
Please see the Expert Consult website for more discussion of this topic.
The genetic control of thyroid descent is now reasonably clearly understood, with a number of the transcription factors involved in the process having been identified. TTF-1 appears at the earliest stages of thyroid development and regulates the expression of thyroperoxidases and thyroglobulin. Pax-8 has similar actions and is also expressed in the embryonic thyroid during descent. Both of these genes are regulated by TTF-2, and disruption is associated with thyroid dysgenesis.33–35 HoxA3 regulates a number of diverse embryonic processes, and disruption of this gene in mice results in thyroid hypoplasia. Genetic abnormalities in any of these genes therefore appear to lead to either impaired thyroid descent or development.
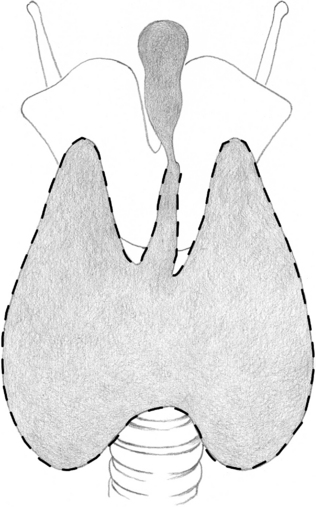
We believe that the presence of these embryologic remnants has considerable clinical importance, especially in the development of recurrent thyroid disease. There are three common sites of embryologic recurrence (or persistence) of nodular goiter: (1) within the pyramidal lobe, (2) within thyroid rests in the thyrothymic tract, or (3) within posterior remnants associated with the tubercle of Zuckerkandl. The pyramidal lobe is the embryologic remnant of the thyroglossal tract, the pathway taken by the thyroid as it descends from the foramen cecum, its place of origin, at the base of the embryologic tongue to its final position in the neck base overlying the second and third tracheal ring. The pyramidal lobe is variable both in incidence and form (typical pyramidal, stringlike, nodular, and inverted Y). The incidence of a pyramidal lobe is between 15% and 75% in anatomic works, and it should essentially be considered a normal part of the thyroid gland.36 It appears to have a slightly male predominance and more commonly arises from the isthmus on the left-hand side.37 Its relevance lies in the fact that it may not be readily identified on preoperative scanning and therefore unless specifically examined for at the primary operation may be missed. Recurrence in this area is best avoided by routine dissection of the midline up to the notch of the thyroid cartilage and careful examination of this anterior cervical region. It is important to appreciate that the pyramid may become very small and attenuated at the level of the cricothyroid membrane, expanding again with a significant volume of thyroid tissue at the level of the notch of the thyroid cartilage, the most common site of recurrent disease (Figure 10-2). Nodular recurrence in the pyramidal lobe will commonly present with an unsightly midline mass. Provided it is the sole site of recurrence, reoperative surgery is very straightforward, requiring only local excision of the pyramidal tract. Care needs to be taken in the region of the cricothyroid membrane, as this may be scarred and thin and the larynx may be inadvertently entered. As for the primary operation, central neck dissection, as we have mentioned, needs to continue up and beyond the notch of the thyroid cartilage to ensure complete removal of any residual tissue in this area.
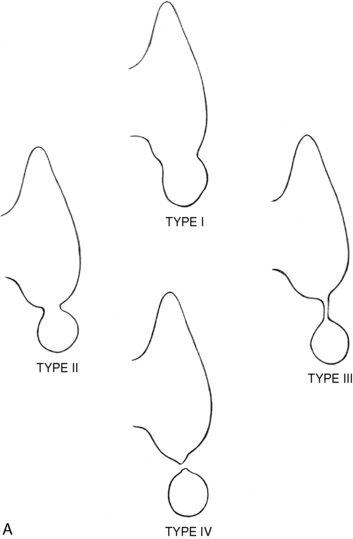
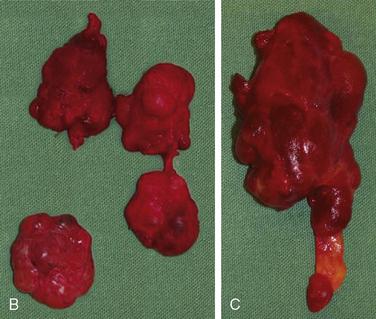
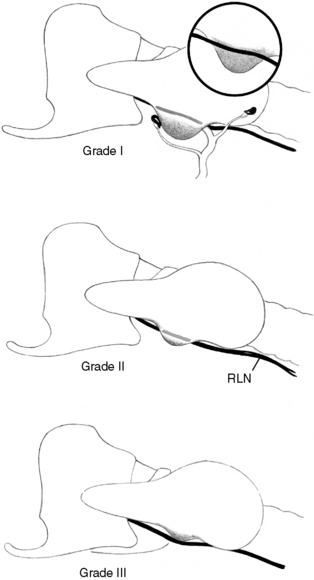
Thyroid rests are defined as small rests or protuberances of normal thyroid tissue that lie in the line of the thyrothymic tract at the lower pole of the thyroid. They are common, with an incidence over 50% of individuals undergoing thyroid surgery, and are presumably an extension of the normal embryologic thyroid descent.38 They are graded as I to IV, according to their relationship to the thyroid gland. Grade I thyroid rests consist of a protrusion of thyroid tissue arising from the inferior aspect of the thyroid gland in the region of the thyrothymic tract, distinctly recognizable from the lower border of the thyroid gland itself. Grade II rests include thyroid tissue lying within the thyrothymic tract and attached to the thyroid by a narrow pedicle of thyroid tissue. Grade III rests are similar but are only attached by a thin fibrovascular core. Grade IV have no connection to the thyroid gland (Figure 10-3).
 Please see the Expert Consult website for more discussion of this topic.
Please see the Expert Consult website for more discussion of this topic.
About 20% to 30% of thyroid rests will be grade III or IV and will be easily missed at primary surgery if the thyrothymic tract is not dissected out. A relatively small nodule of thyroid tissue in this location may continue to grow postoperatively and present with a retrosternal recurrence following presumed total thyroidectomy. Indeed, in our unit 12 patients have presented in such a manner and required further surgery.10 Four of these patients had their original surgery within this unit. Consequently, as thyroid rests are common, we recommend routine examination of the thyrothymic fatty tissue adjacent to the inferior pole to ensure removal of all thyroid tissue at the primary operation. Nodular recurrence in a thyrothymic thyroid rest may present with a recurrent mass low in the neck or in the suprasternal notch (see Figure 10-3). More commonly, however, it presents with a retrosternal recurrence that is not clinically apparent. Such lesions may be diagnosed on chest film or computed tomography (CT) scan performed to assess unrelated symptoms, or they may present with local obstructive symptoms related to tracheal or esophageal compression. Cervical thyrothymic recurrence is readily managed by local excision, although the inferior parathyroid glands will always be at risk. Additionally, the recurrent laryngeal nerve needs to be carefully searched for, as it may be caught in scar tissue and lie more anteriorly than would normally be anticipated. Retrosternal recurrence after a previous cervical thyroidectomy presents a major surgical challenge. Although most retrosternal goiters can be safely delivered through a cervical approach, the dissection and scarring from the previous total thyroidectomy significantly impede the ability to obtain safe access through the neck. Additionally, it is likely that further aberrant vascular supply will have developed following the removal of the cervical component, adding to the dangers of attempted cervical removal. Therefore, we feel the majority of patients with retrosternal recurrence following previous total thyroidectomy will thus likely require a planned median sternotomy for safe removal.
The tubercle of Zuckerkandl is also an embryologic site with the potential for persistent or recurrent disease. The tubercle of Zuckerkandl is a poorly known and variable anatomic feature of the thyroid gland, first described by Zuckerkandl in 1902 as the “processus posterior glandulae thyroidea.”39,40 Nodular change in the tubercle is more common than has been appreciated, being present in over 50% of patients having initial surgery for nodular goiter.41 Its significance lies in the fact that enlargement and nodule change in the tubercle may be primarily retroesophageal and not appreciated at initial surgery, such that the posterior component is left behind, leading to posterior persistence or recurrence (Figure 10-4).
Accessory thyroid glands were initially described in 1965 and can be categorized into three groups depending on their location (cranial, caudal, and lateral).37,42 A normal thyroid gland may be present or absent. The cranial glands usually lie inferior to the hyoid bone on the thyrohyoid membrane or the thyroid cartilage. Caudal accessory glands are located between the lower border of the thyroid and the aortic arch. Lateral glands arise from a failure of the lateral anlage of the thyroid to fuse with its median counterpart during embryologic development and lie in the lateral compartment of the neck in any of anatomic levels I to V.43 In practice, these rare accessory glands are an uncommon cause of recurrent goiter, and indeed we do not routinely look for them during primary procedures.
Underlying Aggressive Benign Nodular Disease Causing Recurrence
 Please see the Expert Consult website for more discussion of this topic.
Please see the Expert Consult website for more discussion of this topic.
Underlying Aggressive Benign Nodular Disease Causing Recurrence
Occasionally, despite meticulous initial total thyroidectomy, small remnants of residual thyroid tissue can grow and present with clinical recurrence. This occurs most commonly in the setting of a previous “near-total” thyroidectomy where a small remnant, often less than 1 gm of tissue, has been left behind to protect a parathyroid gland or the recurrent laryngeal nerve. Occasionally despite a meticulous total thyroidectomy, such small thyroid remnants can regrow and present as clinical recurrence despite thyroxine medication because of an aggressive, albeit benign, process such as dyshormonogenesis.10 This pathologic process differs from that of a benign multinodular goiter (BMNG). Benign multinodular goiter results from heterogeneity of the thyroid-stimulating hormone (TSH) receptor resulting in nodular change admixed with areas of degeneration. Dyshormonogenetic goiter, on the other hand, results from chronic stimulation of the TSH receptor due to a disturbance in the feedback system of thyroid hormone synthesis.44 Dyshormonogenetic goiters are characterized by hypercellular nodules that are solid and microfollicular. Nuclei may be enlarged, irregularly shaped, and often bizarre and can be difficult to distinguish from thyroid carcinoma.45,46
The pathogenesis of multinodular goiter formation and recurrence remains poorly understood.47 Chronic stimulation of TSH receptors may lead to recurrence even if there are minimal numbers of thyroid cells left behind following a total thyroidectomy. It is clear that long-standing goiters develop considerable structural and functional heterogeneity of the TSH receptors, which is accompanied by the formation of multiple nodules. Advances in molecular biology have allowed for the recognition of differing clonal variations in primary and recurrent disease. A study by Harrer showed that most nodules within a recurrent multinodular goiter were polyclonal, suggesting a de novo proliferation of cohorts of differing thymocytes because of, as of yet, unknown growth-stimulating molecular events.48,49 Recurrent disease may become independent from the normal regulatory pathways, partly because of the stimulation from insulin-like growth factors and their binding proteins, rather than from TSH.3,48,49 Thus, through a variety of stimulatory pathways, recurrent benign goiters that clinically manifest share a characteristic high intrinsic growth rate and may therefore form from quite small volumes of residual thyroid tissue.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


