Purpose
To evaluate the incidence of remission among patients with intermediate uveitis; to identify factors potentially predictive of remission.
Design
Retrospective cohort study.
Methods
Involved eyes of patients with primary noninfectious intermediate uveitis at 4 academic ocular inflammation subspecialty practices, followed sufficiently long to meet the remission outcome definition, were studied retrospectively by standardized chart review data. Remission of intermediate uveitis was defined as a lack of inflammatory activity at ≥2 visits spanning ≥90 days in the absence of any corticosteroid or immunosuppressant medications. Factors potentially predictive of intermediate uveitis remission were evaluated using survival analysis.
Results
Among 849 eyes (of 510 patients) with intermediate uveitis followed over 1934 eye-years, the incidence of intermediate uveitis remission was 8.6/100 eye-years (95% confidence interval [CI], 7.4–10.1). Factors predictive of disease remission included prior pars plana vitrectomy (PPV) (hazard ratio [HR] [vs no PPV] = 2.39; 95% CI, 1.42–4.00), diagnosis of intermediate uveitis within the last year (HR [vs diagnosis >5 years ago] =3.82; 95% CI, 1.91–7.63), age ≥45 years (HR [vs age <45 years] = 1.79; 95% CI, 1.03–3.11), female sex (HR = 1.61; 95% CI, 1.04–2.49), and Hispanic race/ethnicity (HR [vs white race] = 2.81; 95% CI, 1.23–6.41). Presence/absence of a systemic inflammatory disease, laterality of uveitis, and smoking status were not associated with differential incidence.
Conclusions
Our results suggest that intermediate uveitis is a chronic disease with an overall low rate of remission. Recently diagnosed patients and older, female, and Hispanic patients were more likely to remit. With regard to management, pars plana vitrectomy was associated with increased probability of remission.
Uveitis, as the fifth- or sixth-leading cause of blindness in Western populations, accounts for a large amount of visual disability in the United States, striking at a younger age than most of the other leading causes of blindness, and thus leading to more years of potential vision lost per case of blindness than conditions striking at a later age. Intermediate uveitis (IU), as defined by the Standardization of Uveitis Nomenclature (SUN) Working Group, is a subset of uveitis in which the primary site of inflammation is in the vitreous, particularly the anterior vitreous and vitreous overlying the ciliary body and peripheral retina–pars plana complex. Clinically, inflammation predominantly affects the vitreous, often forming “snowbanks” and/or “snowballs” in association with vitreous cells and inflammatory debris. A small retrospective cohort study providing population-based natural history data suggests that while the majority of intermediate uveitis patients do relatively well, with 75% maintaining visual acuity of 20/40 or better at 10 years, the course can vary widely. Possible vision-threatening sequelae of intermediate uveitis include but are not limited to macular edema, epiretinal membrane formation, cataract, retinal neovascularization, vitreous cellular opacification, and retinal detachment.
The probability of remission of intermediate uveitis, and predictive factors for remission, are unclear. Vidovic-Valentincic and associates studied 29 patients with unilateral or bilateral intermediate uveitis and found that one-third of patients achieved remission for longer than 1 year, with a mean time to remission of 8.6 years. An additional study conducted by Smith and associates in 1973 reported a remission rate of cyclitis, a term previously used for intermediate uveitis, to be 5% in patients with variable follow-up ranging from 4 to 26 years.
With regard to treatment options to induce remission of intermediate uveitis, a “4-step” approach proposed by Kaplan in 1984 suggests a trial of (local/systemic) corticosteroids, followed by peripheral retinal ablation, pars plana vitrectomy, and, finally, immunomodulatory therapy for refractory cases. However, this approach has not been universally accepted; with increasing evidence of safety and effectiveness, many clinicians are using immunosuppressive therapy at an earlier stage. Remission of ocular inflammatory diseases in general seems to be infrequent with antimetabolite or cyclosporine therapy, but fairly common with alkylating agent therapy. However, alkylating agent therapy generally is reserved for very severe cases, because of an apparently increased risk of cancer. Therefore, with the treatment approaches typically used, clinicians often are aiming to suppress inflammation in the hope that remission will occur during the period of suppression.
Because remission would be a more desirable outcome than suppression, we evaluated the incidence of remission in a large retrospective cohort of patients with intermediate uveitis, and evaluated potentially modifiable and nonmodifiable factors potentially predictive of remission.
Methods
Study Population
Patients with a diagnosis of intermediate uveitis were identified from the Systemic Immunosuppressive Therapy for Eye Disease (SITE) Cohort Study, a retrospective cohort study of noninfectious ocular inflammatory disease patients at US tertiary ocular inflammation subspecialty centers, the methods of which have been described previously. The institutional review boards of the University of Pennsylvania (IRB#1), the Massachusetts Eye & Ear Infirmary (Human Subjects Committee), the Johns Hopkins School of Medicine (JHM-IRB 3), the National Eye Institute (NEI/IRB) and Oregon Health & Sciences University (OHSU Institutional Review Board) approved the study, including waiver of informed consent for this chart review study, which involved no contact with the human subjects. The study was conducted adhering to the tenets of the Declaration of Helsinki, and was compliant with all relevant laws.
Intermediate uveitis had been identified in charts in a manner very similar to that adopted by SUN Group standards, as the leaders of the SUN Group were leading clinicians in the SITE Cohort Study. Those patients identified in medical records as having intermediate uveitis but who also had iris synechiae and/or a formal secondary diagnosis of anterior uveitis or some other inflammatory syndrome were excluded, in order to limit the population to classic intermediate uveitis—the population that makes up the study cohort reported here. This population includes “pars planitis” as well as other forms of intermediate uveitis, as described in the SUN consensus manuscript, whether or not a systemic disease was associated.
Data Collection
Data were obtained and entered in a computerized database entry system (Microsoft Access, Redmond, Washington, USA) with built-in quality assurance measures allowing for correction of errors in real time. Data used for the current analysis included demographic data, the presence of systemic diseases, the presence of HLA-B27 and HLA-A29 haplotypes (when available), time between intermediate uveitis diagnosis and presentation, inflammatory findings at every visit, and treatments used throughout follow-up. Collected patient demographic data included age, sex, race/ethnicity (White, Black, Hispanic, “Other”), and smoking status. The systemic inflammatory diseases evaluated are summarized in the Table . Use of peripheral ablation (cryotherapy or laser) and pars plana vitrectomy were noted.
| Characteristics | Characteristic Value | Total Eyes | Remissions Observed | Eye-Years | Incidence Rate (95% CI) | Crude HR of Remission (95% CI) | Adjusted HR of Remission a |
|---|---|---|---|---|---|---|---|
| Number of eyes | 849 | 167 | 1934.4 | 0.086 (0.074–0.10) | |||
| Age | Age <18 | 154 | 34 | 419.31 | 0.081 (0.056–0.11) | 1.18 (0.68–2.04) | 0.95 (0.53–1.70) |
| 18 ≤ age <30 | 211 | 35 | 550.85 | 0.064 (0.044–0.088) | 0.96 (0.54–1.68) | 0.82 (0.46–1.46) | |
| 30 ≤ age <45 | 271 | 43 | 596.42 | 0.0721 (0.052–0.097) | Reference group | Reference group | |
| Age ≥45 | 213 | 55 | 367.79 | 0.15 (0.11–0.19) | 2.00 (1.21–3.30) | 1.79 (1.03–3.11) | |
| Sex | Male | 315 | 44 | 790.67 | 0.056 (0.040–0.075) | 1.00 | 1.00 |
| Female | 534 | 123 | 1143.7 | 0.11 (0.089–0.13) | 1.82 (1.18–2.81) | 1.61 (1.04–2.49) | |
| Race | White | 731 | 151 | 1665.0 | 0.0907 (0.077-0.11) | Reference group | Reference group |
| Black | 43 | 5 | 138.59 | 0.036 (0.012-0.084) | 0.46 (0.13-1.61) | 0.53 (0.14-2.04) | |
| Hispanic | 34 | 9 | 31.14 | 0.29 (0.13-0.55) | 2.39 (0.96-5.95) | 2.81 (1.23-6.41) | |
| Other | 41 | 2 | 99.64 | 0.020 (0.0024–0.073) | 0.24 (0.05–1.07) | 0.26 (0.06–1.19) | |
| Any systemic disease b | Yes | 94 | 14 | 266.60 | 0.053 (0.029–0.088) | 0.62 (0.30–1.24) | 0.59 (0.29–1.22) |
| Juvenile idiopathic arthritis | Yes | 8 | 5 | 29.61 | 0.17 (0.055–0.39) | 2.25 (0.70–7.22) | 1.50 (0.39–5.83) |
| Sarcoidosis | Yes | 43 | 9 | 116.21 | 0.077 (0.035–0.15) | 0.94 (0.40–2.21) | 0.63 (0.23–1.70) |
| Multiple sclerosis | Yes | 40 | 7 | 84.50 | 0.083 (0.033–0.17) | 0.89 (0.42–1.90) | 0.73 (0.30–1.73) |
| Smoking status | Never smoker | 425 | 97 | 1001.6 | 0.097 (0.079–0.12) | Reference group | Reference group |
| Former smoker | 70 | 24 | 176.14 | 0.14 (0.087–0.20) | 1.37 (0.79–2.40) | 0.97 (0.54–1.76) | |
| Current smoker | 216 | 32 | 443.45 | 0.072 (0.049–0.10) | 0.71 (0.43–1.16) | 0.79 (0.46–1.35) | |
| Unknown | 138 | 14 | 313.19 | 0.045 (0.024–0.075) | 0.43 (0.21–0.87) | 0.41 (0.20–0.86) | |
| Number of years since diagnosis of uveitis | ≤1 year | 415 | 42 | 137.45 | 0.31 (0.22–0.41) | 3.81 (1.94–7.48) | 3.82 (1.91–7.63) |
| >1–5 years | 264 | 70 | 715.55 | 0.098 (0.076–0.12) | 1.55 (0.91–2.65) | 1.50 (0.87–2.60) | |
| Over 5 years | 170 | 55 | 1081.4 | 0.051 (0.038–0.066) | Reference group | Reference group | |
| Bilateral uveitis | Yes | 771 | 150 | 1774.7 | 0.085 (0.072–0.099) | 0.82 (0.48–1.39) | 0.73 (0.43–1.23) |
| Snowballs at enrollment | Yes | 234 | 40 | 427.89 | 0.094 (0.067–0.13) | 1.04 (0.69–1.56) | 0.98 (0.66–1.46) |
| Peripheral ablation c | Yes | 44 | 9 | 83.23 | 0.11 (0.049–0.21) | 1.31 (0.67–2.55) | 1.71 (0.84–3.45) |
| Pars plana vitrectomy | Yes | 81 | 23 | 123.64 | 0.19 (0.12–0.28) | 2.84 (1.76–4.58) | 2.39 (1.42–4.00) |
a Adjusted values are adjusted for age, sex, race, smoking status, presence of snowballs at the initial visit, the number of years since uveitis diagnosis, and whether or not peripheral ablation or pars plana vitrectomy were performed.
b There were no cases of reactive arthritis, psoriatic arthritis, polyarteritis nodosum, Wegener, Takayasu, scleroderma, Sjogren, dermatomyositis, polymyositis, relapsing polychrondritis, Cogan, or familial systemic granulomatosis. There was no association observed between intermediate uveitis remission and spondylarthropathy (ie, ankylosing spondylitis), Behçet disease, systemic lupus erythematosis, rheumatoid arthritis, Crohn disease, ulcerative colitis, HLA-B27+ status, or HLA-A29+ status; however, available power often was limited to detect such associations, if they in fact exist.
c Peripheral retina/pars plana ablation using either cryotherapy or scatter photocoagulation.
Study Outcomes
The primary outcome of this study was remission of intermediate uveitis among eyes (as opposed to patients). Intermediate uveitis remission was defined as the complete absence of inflammatory signs in an eye across all visits spanning a period of at least 90 days, in the absence of any ocular or systemic anti-inflammatory treatment.
Statistical Analyses
Follow-up time was the sum of the time eyes at “risk” of remission were followed (until occurrence of remission, or cessation of follow-up owing to censoring or the end of the study). An eye-year is 365.25 such days. The incidence of intermediate uveitis remission was calculated as the number of events per eye-year among those still under observation who had not yet had remission at presentation; 95% confidence intervals assumed a Poisson distribution. Factors potentially predictive of remission were evaluated using survival analysis. Cox regression (with 95% confidence interval [CI] bounds indicated as subscripts before and after the estimates) was used to generate crude and adjusted hazard ratios (HRs) for each factor, with final models selected based on associations observed in the crude analyses, and the factors of specific scientific interest. Final multiple regression models adjusted for age, sex, race, smoking status, presence of snowballs at the initial visit, the number of years since uveitis diagnosis, and whether or not peripheral ablation or pars plana vitrectomy were performed. Kaplan-Meier curves were constructed for selected variables to display the relationship with incidence of uveitis remission as a function of time. Analyses were performed using Stata 11 (StataCorp, College Station, Texas, USA) and SAS v9.1 (SAS Corporation, Cary, North Carolina, USA) software.
Results
The Table summarizes the characteristics of the 849 eyes (of 510 patients) with intermediate uveitis meeting eligibility criteria. These had been followed over 1934 eye-years at the participating centers. The majority of eyes belonged to female patients (63%) and persons of white race (86%), and half to known nonsmokers (50%). All age groups were represented; 18% were less than 18 years old, 25% were between 18 and 30 years of age, 32% were between 30 and 45 years of age, and 25% were 45 years of age or older. The majority (91%; 82% of patients) experienced bilateral intermediate uveitis at some point during their clinical course. There were 43 eyes of patients with sarcoidosis (5.1%) and 40 eyes of patients with multiple sclerosis (4.7%).
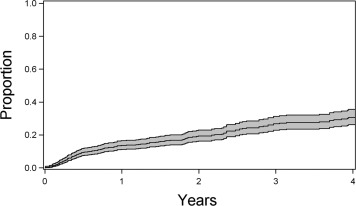
A total of 167 remissions of disease activity, spanning at least 90 days in the absence of any anti-inflammatory medication, were observed. The calculated incidence rate for intermediate uveitis remission was 8.6/100 eye-years (95% CI, 7.4–10.1/100 eye-years; Figure 1 ).
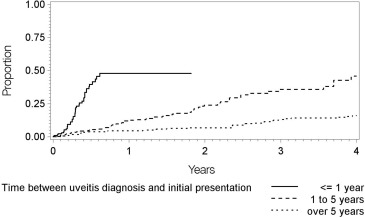
The relationship of potentially predictive factors to intermediate uveitis remission is given in the Table . Demographic characteristics associated with greater incidence of remission included age 45 years or greater (incidence = 15.0 per 100 eye-years, adjusted HR [vs 30 ≤ age < 45 years] = 1.79; 95% CI, 1.03-–3.11), female sex (incidence = 10.8 per 100 eye-years, adjusted HR [vs male sex] = 1.61; 95% CI, 1.04–2.49), and Hispanic race/ethnicity (incidence = 28.9 per 100 eye-years, adjusted HR [vs white race/ethnicity] = 2.81; 95% CI, 1.23–6.41). Few cases meeting eligibility criteria were observed in Black or other races/ethnicities. Diagnosis of intermediate uveitis within the last year also was associated with a greater incidence of remission (incidence = 30.6 per 100 eye-years, adjusted HR = 3.82; 95% CI, 1.91–7.63) with respect to longstanding cases diagnosed more than 5 years previously ( Figure 2 ). The incidence of remission was 10/100 eye-years for cases diagnosed with intermediate uveitis 1-5 years prior to presentation, and 5/100 eye-years for cases diagnosed over 5 years previously. Associated systemic diseases were not associated with significant differences in the incidence of remission, nor were bilaterality of uveitis or the presence or absence of vitreous snowballs at the initial examination.