Purpose
To describe 12-month changes in choroidal thickness after anti–vascular endothelial growth factor (anti-VEGF) therapy for typical age-related macular degeneration (AMD) and polypoidal choroidal vasculopathy (PCV).
Design
Prospective, consecutive, noninterventional, longitudinal case series.
Methods
This study included patients with typical AMD and PCV who received anti-VEGF therapy over a 12-month period. We used spectral-domain optical coherence tomography with enhanced depth imaging mode to measure choroidal thickness.
Results
Of the 163 patients, 77 had typical AMD and 86 had PCV. Patients with PCV were younger (67.6 vs 72.5 years, P < .01) and received fewer anti-VEGF injections (3.9 vs 5.6, P = .02) than patients with typical AMD. Baseline subfoveal choroidal thickness was not significantly different between PCV and typical AMD eyes, and was thicker in the study eye compared to fellow eye in the typical AMD group (223.1 vs 208.8 μm, P < .01). Subfoveal choroidal thickness decreased significantly in both typical AMD (213.7 μm to 190.3 μm, P < .001) and PCV (240.8 μm to 213.4 μm, P < .01) eyes, but no significant change was noted in fellow unaffected eyes. Reduction in choroidal thickness was associated with elevated C-reactive protein (odds ratio [OR]: 1.4, P = .04) and smoking (OR: 7.6, P = .03) at baseline, but not with age, refractive error, diagnosis of typical AMD or PCV, number or type of anti-VEGF injections, PDT therapy, or baseline choroidal thickness.
Conclusions
A significant reduction in subfoveal choroidal thickness was noted after anti-VEGF therapy in typical AMD and PCV. Choroidal thickness changes were similar despite differences in number of anti-VEGF treatment.
Age-related macular degeneration (AMD) is a major cause of vision impairment in the elderly population in the Western world and Asian countries. Anti–vascular endothelial growth factor (VEGF) agents have been demonstrated as highly effective treatments in exudative (“wet”) AMD. However, long-term treatment with multiple injections is required to maintain the initial visual improvement. Recently, there has been a concern as to whether long-term anti-VEGF therapy may have deleterious effects on the choroid and retinal pigment epithelium (RPE), as VEGF plays an essential role in maintenance of choroidal vascular health and function. The development of geographic atrophy in AMD patients after anti-VEGF therapy has been reported in several large series, including Comparison of AMD Treatment Trial (CATT), Inhibition of VEGF in Age-related choroidal Neovascularization (IVAN), and pHase III Active treatment-controlled study of the efficacy and safety of 0.5 mg and 2.0 mg Ranibizumab administered monthly or on an as-needed Basis in patients with subfoveal neOvasculaR AMD (HARBOR). However, whether this reflects a cause-and-effect relationship or whether this reflects natural history of AMD remains to be determined.
Choroidal thickness can now be measured by spectral-domain optical coherence tomography (OCT) with enhanced depth imaging. Choroidal thinning and atrophy may be a precursor to the development of RPE atrophy and geographic atrophy over time. To date, however, the effect of anti-VEGF therapy on changes in choroidal thickness remains unclear. Some studies suggested that choroidal thinning occurs in eyes that received multiple intravitreal injections, but others have not reported any changes. An increase in choroidal thickness, possibly reflecting increased choroidal hyperpermeability, may also be important in the pathogenesis of polypoidal choroidal vasculopathy (PCV), a subtype of AMD. To address this gap, we evaluated changes in choroidal thickness over 12 months in exudative AMD patients treated with anti-VEGF agents, and compared changes in choroidal thickness between eyes with typical AMD and PCV.
Methods
Study Population
This was a prospective, observational cohort study involving patients with exudative AMD in the Asian AMD Phenotyping Study. Detailed methodology had been published elsewhere. This study was approved by the Centralized Institutional Review Board (CIRB) of SingHealth, Singapore (protocol number R697/47/2009) and conducted in accordance with the Declaration of Helsinki. All participants provided a signed informed consent for their participation.
Clinical Examination and Diagnosis
At baseline, all patients underwent comprehensive ophthalmic evaluation including best-corrected visual acuity (BCVA) testing using logarithm of the minimal angle of resolution (logMAR), refraction, slit-lamp biomicroscopy examination, and imaging according to standardized protocol, which included color fundus photography and angiography with fluorescein and indocyanine green (TRC-50X/IMAGEnet 2000; Topcon, Tokyo, Japan or Spectralis; Heidelberg Engineering, Heidelberg, Germany). Clinical information including medical history and smoking history was recorded using a standardized clinic record form. Total cholesterol and C-reactive protein (CRP) were measured from nonfasting venous blood samples.
Patients were classified as typical AMD and PCV based on fundus fluorescein angiogram and indocyanine green (ICG) angiogram. The typical AMD is graded based on the modification from the Macular Photocoagulation Study. Presence or absence of choroidal neovascularization (CNV) is graded. On the other hand, PCV is diagnosed if there is presence of at least 1 of the following criteria: protruded orange-red elevated lesions observed by fundus examination; characteristic polypoidal lesions seen in ICG.
Participants received treatment according to standard of care, and treatment was not altered by entering into the study. Patients were followed up prospectively according to clinical need, but minimum reviews, including BCVA and OCT imaging, were repeated at months 3, 6, and 12. All patients with typical AMD were treated with intravitreal anti-VEGF based on a pro re nata (PRN) regimen. Retreatment with additional anti-VEGF injections was made in the presence of persistent or recurrent subretinal or intraretinal fluid or hemorrhage. In cases of PCV, anti-VEGF was recommended where there was significant fluid or hemorrhage subfoveally. In addition, photodynamic therapy (PDT) was added for extensive PCV lesions.
Choroidal Thickness Measurement
For the current analysis, we only included eyes in which spectral-domain OCT with enhanced depth imaging mode (Heidelberg Retina Angiography, Spectralis; Heidelberg Engineering, Heidelberg, Germany) was available since 2012. A minimum of 25 B-scans per volume scan of 20 × 20 degrees was used. Each scan was averaged with 9 frames per B-scan with a distance of 240 μm between each B-scan, centering at the fovea.
Two trained graders measured the choroidal thickness independently at the subfoveal region and at 1.5 mm nasal and temporal to the center of the fovea. Choroidal thickness was defined as the distance between the hyperreflective line corresponding to the Bruch membrane beneath the retinal pigment epithelium and choroidal-scleral interface, as used in previous studies. The choroidal measurements from both graders were averaged. Both graders were masked to the patients’ information.
Statistical Analysis
The primary outcome was the change in subfoveal choroidal thickness from baseline to month 12. The data obtained from all patients were analyzed with frequency and descriptive statistics. We analyzed the categorical variables using paired t test while the generalized linear mixed models were used to assess the effect of anti-VEGF on choroidal thickness and BCVA at months 3, 6, and 12. We also stratified our analysis based on diagnosis of typical AMD vs PCV. All data were expressed as mean ± standard deviation, and a P value < .05 was considered to be statistically significant. For risk factor analysis, we defined significant choroidal thinning as ≥16 μm, as this value represents 10 times the reported annual choroidal thinning rate (1.56 μm/year) from previous study. We performed a multiple-adjusted risk factor analysis to evaluate the influence of age, sex, refractive error, baseline diagnosis (typical AMD or PCV), baseline choroidal thickness, photodynamic therapy, number of anti-VEGF injections, CRP, and vascular risk factors (hypertension, total cholesterol, and current smoking). All statistical analyses were performed using SPSS version 21 (SPSS, Chicago, Illinois, USA).
Results
Of the 163 patients presenting with exudative AMD, 86 patients (52.7%) had PCV while 77 (47.3%) had typical AMD. After excluding 8 fellow eyes (4 typical AMD and 4 PCV patients) that developed exudative AMD during the follow-up period, 155 fellow eyes were also included in this analysis.
The baseline demographics and baseline choroidal thickness are summarized in Table 1 . Patients with PCV were significantly younger than patients with typical AMD (67.6 vs 72.5 years, P < .01). Presenting visual acuity was similar between the 2 groups. Patients with PCV generally had thicker baseline choroidal thickness at all 3 measured locations across the macula than typical AMD patients in both the affected eye and the fellow eye. However, the difference was not statistically significant after adjusting for age and sex. Subfoveal choroidal thickness was significantly greater in study eyes compared to the fellow eyes in the typical AMD group (223.1 vs 208.8 μm, P < .01) ( Table 1 ). In contrast, in PCV patients, the difference in baseline subfoveal choroidal thickness between study eye and fellow eye was not statistically significant (245.0 vs 234.9 μm, P = .18).
| Affected eyes | Overall (n = 163) | Typical AMD (n = 77) | PCV (n = 86) | P Value a |
|---|---|---|---|---|
| Age (y) | 69.9 (9.60) | 72.5 (8.54) | 67.6 (9.96) | <.01 |
| Sex, female | 76 (46.6) | 32 (41.6) | 44 (51.2) | .41 |
| Smoking status | 25 (15.8) | 14 (18.2) | 11 (13.6) | .46 |
| Spherical equivalent | −0.28 (2.32) | −0.43 (2.29) | −0.14 (2.36) | .44 |
| Best-corrected visual acuity (logMAR) | 0.861 (0.508) | 0.854 (0.510) | 0.868 (0.509) | .80 |
| Affected eyes | Typical AMD (n = 77) | PCV (n = 86) | ||
|---|---|---|---|---|
| Baseline choroidal thickness (μm) (n = 163) | ||||
| Subfoveal | 234.7 (88.4) | 223.1 (84.4) | 245.0 (91.1) | .66 |
| Nasal | 196.5 (86.6) | 177.2 (76.6) | 213.7 (91.8) | .10 |
| Temporal | 221.0 (85.9) | 210.1 (83.3) | 230.7 (87.6) | .78 |
| Fellow eyes | Typical AMD (n = 73) | PCV (n = 82) | ||
|---|---|---|---|---|
| Baseline choroidal thickness (μm) (n = 155) | ||||
| Subfoveal | 222.6 (95.4) | 208.8 (84.7) | 234.9 (103.0) | .46 |
| Nasal | 192.3 (92.9) | 182.0 (86.9) | 201.5 (97.6) | .83 |
| Temporal | 215.1 (88.7) | 201.8 (85.9) | 227.0 (90.0) | .31 |
a P value calculated using Student t test, with adjusted age and sex.
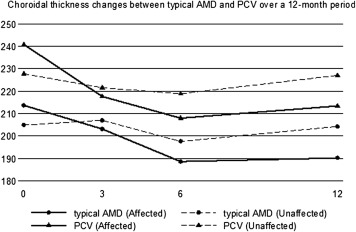
A significant reduction in subfoveal choroidal thickness was noted at month 12 compared to baseline in 104 patients (typical AMD: 43; PCV: 61) who had completed 12 months follow-up (typical AMD: 214 μm to 190 μm, P < .001, representing 11.2% reduction from baseline; PCV: 241 μm to 213 μm, P < .01, representing 11.6% reduction from baseline) ( Table 2 ). Similar choroidal thickness reduction was found in nasal and temporal regions for both typical AMD and PCV patients ( Table 2 ). There was no significant thinning in subfoveal choroidal thickness detected in the fellow unaffected eyes ( Table 2 ). In addition, there was no significant difference in the percentage change from baseline at each time point between the typical AMD and PCV group (data not shown). We repeated the analysis, including patients treated with bevacizumab only, and the results remained unchanged ( Table 3 ). Figure 1 shows the subfoveal choroidal thickness of typical AMD (affected vs fellow eyes) and PCV (affected vs fellow eyes) patients who had completed the study ( Figure 1 ). An example of the choroidal thickness changes in typical AMD and PCV over a 12-month period is shown in Figure 2 . In the subgroup analysis for PCV patients only, the reduction in subfoveal choroidal thickness between the monotherapy (anti-VEGF) and the combination therapy (anti-VEGF and photodynamic therapy) was not statistically significant (33 μm vs 27 μm, P = .87).
| Baseline Mean (Standard Deviation) | Month 3 Mean (Standard Deviation) | P Compared to Baseline | Month 6 Mean (Standard Deviation) | P Compared to Baseline | Month 12 Mean (Standard Deviation) | P Compared to Baseline | |
|---|---|---|---|---|---|---|---|
| Typical AMD (affected) (n = 43) | |||||||
| Mean cumulative number of anti-VEGF injections | 0 | 2.60 (0.79) | 3.88 (1.33) | 5.60 (2.12) | |||
| Best-corrected visual acuity | 0.936 (0.60) | 0.662 (0.48) | .03 | 0.713 (0.43) | .07 | 0.766 (0.45) | .16 |
| Choroidal thickness (μm) | |||||||
| Subfoveal | 213.7 (83.7) | 203.2 (71.0) | .08 | 188.6 (80.6) | <.01 | 190.3 (83.0) | <.001 |
| Nasal | 176.4 (79.0) | 175.6 (80.0) | .61 | 162.5 (87.3) | .07 | 166.7 (86.1) | .05 |
| Temporal | 205.9 (76.7) | 202.7 (79.7) | .60 | 193.2 (87.8) | .56 | 188.4 (81.6) | .01 |
| PCV (affected) (n = 61) | |||||||
| Mean cumulative number of anti-VEGF injections | 0 | 2.28 (0.95) | 3.20 (1.76) | 3.92 (2.29) | |||
| Best-corrected visual acuity | 0.921 (0.63) | 0.705 (0.58) | <.01 | 0.659 (0.52) | <.0001 | 0.597 (0.46) | <.0001 |
| Choroidal thickness (μm) | |||||||
| Subfoveal | 240.8 (92.9) | 217.6 (89.0) | <.001 | 208.0 (97.7) | <.0001 | 213.4 (98.5) | <.01 |
| Nasal | 211.0 (95.1) | 200.1 (104.2) | .13 | 186.8 (101.7) | <.0001 | 186.6 (99.7) | <.001 |
| Temporal | 231.4 (91.2) | 212.7 (83.6) | .01 | 201.5 (87.0) | <.0001 | 198.8 (82.5) | <.001 |
| Typical AMD (fellow) (n = 41) | |||||||
| Choroidal thickness (μm) | |||||||
| Subfoveal | 204.9 (83.3) | 207.0 (84.3) | .87 | 197.6 (82.0) | .57 | 204.3 (78.0) | .90 |
| Nasal | 181.5 (82.3) | 180.7 (82.8) | .36 | 167.1 (77.4) | .07 | 173.1 (80.5) | .03 |
| Temporal | 190.0 (74.2) | 192.4 (66.9) | .66 | 188.9 (77.0) | .68 | 186.0 (66.3) | .50 |
| PCV (fellow) (n = 58) | |||||||
| Choroidal thickness (μm) | |||||||
| Subfoveal | 227.8 (104.0) | 221.5 (97.0) | .32 | 218.8 (102.7) | .16 | 227.0 (111.1) | .90 |
| Nasal | 189.1 (93.7) | 193.1 (96.9) | .22 | 184.7 (98.6) | .52 | 189.1 (103.0) | .99 |
| Temporal | 222.0 (89.4) | 211.7 (90.3) | .08 | 219.9 (103.2) | .88 | 217.1 (93.2) | .44 |
| Baseline Mean (Standard Deviation) | Month 3 Mean (Standard Deviation) | P Compared to Baseline | Month 6 Mean (Standard Deviation) | P Compared to Baseline | Month 12 Mean (Standard Deviation) | P Compared to Baseline | |
|---|---|---|---|---|---|---|---|
| Typical AMD (affected) (n = 24) | |||||||
| Mean cumulative number of bevacizumab injections | 0 | 2.75 (0.53) | 4.04 (1.30) | 5.38 (2.20) | |||
| Best-corrected visual acuity | 0.831 (0.50) | 0.615 (0.44) | .05 | 0.603 (0.41) | .04 | 0.639 (0.43) | .17 |
| Choroidal thickness (μm) | |||||||
| Subfoveal | 227.2 (76.9) | 207.7 (75.8) | .04 | 194.6 (85.5) | <.0001 | 190.5 (73.1) | <.001 |
| Nasal | 181.2 (76.1) | 171.0 (63.0) | .34 | 169.7 (83.7) | .28 | 167.4 (86.1) | .04 |
| Temporal | 215.5 (77.8) | 196.3 (77.3) | .03 | 204.5 (85.7) | .59 | 193.8 (66.0) | <.01 |
| PCV (affected) (n = 18) | |||||||
| Mean cumulative number of bevacizumab injections | 0 | 2.67 (0.77) | 3.61 (1.50) | 4.06 (2.07) | |||
| Best-corrected visual acuity | 0.984 (0.58) | 0.658 (0.33) | <.01 | 0.502 (0.37) | <.01 | 0.580 (0.41) | <.01 |
| Choroidal thickness (μm) | |||||||
| Subfoveal | 261.7 (92.7) | 233.7 (106.3) | .09 | 213.9 (104.8) | <.01 | 235.1 (101.7) | .04 |
| Nasal | 243.4 (90.3) | 249.1 (137.9) | .78 | 208.7 (98.5) | <.01 | 213.3 (108.4) | .03 |
| Temporal | 247.9 (102.1) | 238.7 (98.8) | .44 | 201.5 (87.1) | <.01 | 209.3 (75.2) | <.01 |
| Typical AMD (fellow) (n = 23) | |||||||
| Choroidal thickness (μm) | |||||||
| Subfoveal | 209.8 (76.1) | 206.7 (76.7) | .52 | 196.6 (67.6) | .09 | 206.4 (68.8) | .46 |
| Nasal | 178.2 (73.2) | 171.8 (71.0) | .27 | 167.8 (74.2) | .26 | 167.7 (72.4) | .04 |
| Temporal | 195.0 (71.6) | 194.8 (54.9) | .57 | 193.1 (70.7) | .90 | 192.8 (63.5) | .76 |
| PCV (fellow) (n=17) | |||||||
| Choroidal thickness (μm) | |||||||
| Subfoveal | 251.8 (112.4) | 251.4 (116.8) | .99 | 250.0 (125.2) | .72 | 257.7 (125.9) | .46 |
| Nasal | 222.8 (103.4) | 240.9 (121.2) | .17 | 217.7 (117.5) | .81 | 226.7 (118.6) | .75 |
| Temporal | 245.9 (103.8) | 240.4 (116.5) | .39 | 239.4 (121.6) | .75 | 237.2 (103.9) | .51 |