Purpose
To investigate the relationship between the choroidal thickness and choroidal blood flow in healthy young subjects.
Design
Retrospective, cross-sectional study.
Methods
We examined 25 eyes of 25 healthy young Japanese subjects. The subfoveal choroidal thickness was measured by enhanced depth imaging optical coherence tomography (EDI-OCT). The total choroidal blood flow and subfoveal choroidal blood flow were evaluated by pulsatile ocular blood flow using Langham OBF computerized tonometry and the choroidal blood flow using laser Doppler flowmetry. The refractive error, intraocular pressure, and axial length were also measured.
Results
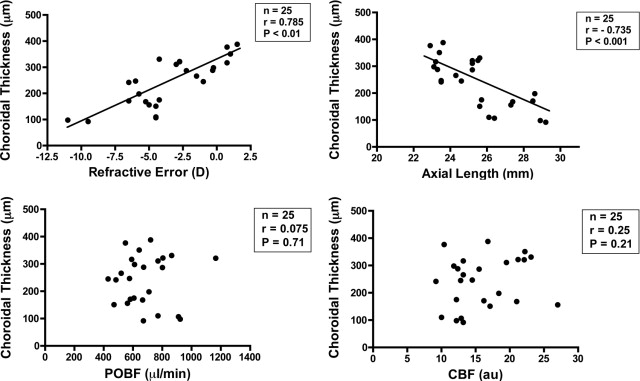
The mean refractive error was −3.4 ± 3.1 diopters, mean intraocular pressure 15.3 ± 1.7 mm Hg, and axial length 25.4 ± 2.0 mm. The subfoveal choroidal thickness was correlated positively (r = 0.785, P < .01) with the refractive error and negatively (r = −0.735, P < .001) with the axial length. No significant correlation was found between the subfoveal choroidal thickness and the pulsatile ocular blood flow or choroidal blood flow.
Conclusion
Our results suggested that there were no significant correlations between the subfoveal choroidal thickness and the total choroidal blood flow and the subfoveal choroidal blood flow in healthy young subjects; however, decreased subfoveal choroidal thickness was associated with decreased refractive error and axial length.
Choroidal blood flow accounts for most of the ocular blood flow and is the major source of oxygen and nutrients for the choroid and the outer retina. Impaired choroidal blood flow is associated with various ocular diseases, for example, tissue hypoxia, which results in formation of choroidal neovascularization (CNV) in patients with pathogenic myopia and age-related macular degeneration (AMD). In addition, decreased choroidal blood flow has been associated with retinitis pigmentosa, glaucoma, and aging. We reported previously that the total choroidal blood flow measured by pulsatile ocular blood flow decreased in patients with AMD.
Recently, the subfoveal choroidal thickness has been measured noninvasively using enhanced depth imaging optical coherence tomography (EDI-OCT), which can obtain much clearer choroidal images than conventional time-domain (TD) OCT. Recent clinical studies have shown the changes in choroidal thickness, increased choroidal thickness (central serous chorioretinopathy and Vogt-Koyanagi-Harada disease ), or decreased choroidal thickness (high myopia, age-related choroidal atrophy, and retinal dystrophy ).
Although the relation between the choroidal thickness measured by EDI-OCT and choroidal blood flow seems to be important, no report has mentioned this relation. In the current study, we investigated for the first time the relation between the choroidal thickness and the choroidal circulation by measuring the subfoveal choroidal thickness and choroidal circulation in healthy young volunteers.
Methods
Twenty-five eyes of 25 healthy young Japanese subjects (14 men, 11 women) were enrolled in the study. The characteristics of the study subjects are shown in the Table . Patients were excluded if they were smokers or had diabetes, heart disease, impaired renal function, hypercholesterolemia, hypertension, ocular disease, or a history of ophthalmic surgery.
| Variable | Mean ± SE |
|---|---|
| Age (years) | 30.1 ± 2.8 |
| IOP (mm Hg) | 15.3 ± 1.7 |
| Refractive error (D) | −3.4 ± 3.1 |
| Axial length (mm) | 25.4 ± 2.0 |
| Systolic BP (mm Hg) | 74.2 ± 3.7 |
| Diastolic BP (mm Hg) | 122.1 ± 6.2 |
| SCT (μm) | 241.3 ± 91.4 |
| POBF (μL/min) | 682.5 ± 167.8 |
| CBF (au) | 15.9 ± 4.7 |
We examined the subfoveal choroidal thickness using EDI-OCT, which has been reported previously. Briefly, choroidal images were obtained using spectral-domain (SD) OCT (Spectralis OCT, Heidelberg Engineering, Heidelberg, Germany). The instrument was sufficiently close to the eye to create an inverted image near the top of the display. Using this technique, choroidal images can be obtained clearly. The subfoveal choroidal thickness was measured vertically from the outer border of the retinal pigment epithelium (RPE) to the inner border of the sclera. The subfoveal choroidal thickness was measured retrospectively using the planimetric scale software in the device.
We evaluated the total choroidal blood flow by measuring the pulsatile ocular blood flow using Langham OBF computerized tonometry (Langham Ophthalmic Technologies, Timonium, Maryland, USA) with the subjects in the sitting position. Data were collected from each subject and the mean measurements were calculated from 5 representative pulses.
To evaluate the choroidal blood flow of the foveal region, determinations of the relative choroidal blood flow value were obtained using a method based on laser Doppler velocity flowmetry, the details of which have been published previously. Briefly, a diode laser (670 nm) with an intensity of 20 mW was delivered through a fundus camera. The diameter of the probing laser beam was about 200 mm. The velocity was expressed in hertz, and volume and flux were expressed in arbitrary units (au). Subjects fixated on the probing laser beam to determine the foveal choroidal blood flow. During blood flow measurements, proper fixation was ascertained by direct foveal observation through the fundus camera. All measurements were performed twice for each patient with the patients in a dark room. The choroidal circulation was measured continuously in each participant for about 30 seconds. All flow parameters then were averaged over 2 periods of 30 seconds.
The refractive error and intraocular pressure (IOP) were measured with the Tonoref RKT-7000 autorefractometer (Nidek Inc, Aichi, Japan). The axial length was measured with the IOL Master 500 (Carl Zeiss Meditec Inc, Jena, Germany). Systolic and diastolic blood pressures (BP) were measured using a sphygmomanometer (Omron Inc, Japan) with subjects in the sitting position.
Independent observers measured the subfoveal choroidal thickness, pulsatile ocular blood flow, and choroidal blood flow. A masked observer (T.N.) analyzed the data to determine the correlation between the subfoveal choroidal thickness and the other parameters.
Statistical Analysis
All data are expressed as the mean ± standard error of the mean. To examine the relationship between the subfoveal thickness and axial length, pulsatile ocular blood flow, and choroidal blood flow, the Spearman correlation test was performed. P < .05 was considered significant.
Results
The patient clinical characteristics are shown in the Table . The mean patient age was 30.1 ± 2.8 (mean ± standard error) years (range, 25−34 years), mean refractive error −3.4 ± 3.1 diopters (D) (range, −11.00 to 1.00 D), mean intraocular pressure 15.3 ± 1.7 mm Hg, mean axial length 25.4 ± 2.0 mm, mean subfoveal choroidal thickness 241.3 ± 91.4 μm, mean pulsatile ocular blood flow 682.5 ± 167.8 μL/min, and choroidal blood flow 15.9 ± 4.7 au.
The subfoveal thickness was positively significantly ( P < .01) correlated with the refractive error ( Figure , Top left) and negatively correlated with the axial length ( Figure , Top right). In contrast, there were no significant correlations between the subfoveal choroidal thickness and the pulsatile ocular blood flow or choroidal blood flow ( Figure , Bottom left and Bottom right). The subfoveal thickness did not have correlation except refractive error and axial length by multiple comparison.