Reconstruction of the Tympanic Membrane and Ossicular Chain
John L. Dornhoffer
Michael B. Gluth
Seeking knowledge and expertise in the art of tympanoplasty and ossiculoplasty can be a difficult task, in part due to the overwhelming number of techniques that have been described, but also because of the plethora of dogma and surgical tradition that circulates throughout the otologic surgery community. In the following chapter, the authors seek not to champion a particular set of techniques, but to provide a broad overview of this topic with a focus on fundamental principles that apply globally. This information is delivered under the assertion that it is wise for otologists to acquire a working mastery of several techniques that may be applied in a customized manner based on pathology and conditions at hand.
DEFINITION OF TERMS
Canalplasty refers to surgical modification of the bony external auditory canal. This is often used as an adjuvant procedure in tympanoplasty to improve surgical access.
Meatoplasty refers to surgical modification of the cartilaginous external auditory canal and external auditory meatus. This is often used as an adjuvant procedure in tympanoplasty to provide improved postoperative access or to attain consistent lateral-to-medial ear canal size matching following canalplasty. Myringoplasty refers to surgical repair of the tympanic membrane that involves work confined to the drumhead only.
Ossiculoplasty refers to surgical modification of the ossicular chain, including reconstruction and mobilization. Tympanoplasty refers to surgical repair of the tympanic membrane in combination with work within the tympanic cleft, such as ossiculoplasty, middle ear exploration, or lysis of tympanic adhesions. Traditionally, elevation of the annulus within a tympanomeatal flap has served as a practical boundary that differentiates tympanoplasty from myringoplasty.
TYPES OF TYMPANOPLASTY AND OSSICULAR RECONSTRUCTION
Tympanoplasty techniques were classically outlined by Zollner (1) and Wullstein (2). Subsequent modifications of Wullstein’s classification have been based on the underlying properties of acoustic mechanics associated with each tympanoplasty type as opposed to classification based on underlying tympanic and ossicular pathology. Understanding this classification system is helpful not only for purposes of grasping a global and historical view of tympanic membrane and ossicular chain reconstruction, but also for understanding basic principles of middle ear acoustic mechanics.
Type I Tympanoplasty
This procedure involves repair of the tympanic membrane in the setting of an intact native ossicular chain. At most, manipulation of the ossicular chain is limited to interventions aimed at improving mobility, such as lysis of tympanic adhesions or removal of tympanosclerotic foci.
Type II Tympanoplasty
This procedure involves repair of the tympanic membrane in combination with any type of ossiculoplasty procedure that preserves the integrity of the malleoincudal lever mechanism. The most common example of this is repair of a dysfunctional (eroded) incudostapedial articulation. Tympanoplasty with delayed staged ossiculoplasty consisting of an incus-grip stapedotomy could also be considered a subgroup within this category. It is perhaps worth noting that these modern depictions of type II tympanoplasty differ somewhat from the classic description that was devised to deal with the uncommon scenario of isolated malleus erosion, wherein tympanic membrane grafting is applied directly upon the intact long process of the incus.
Type III Tympanoplasty
This procedure involves repair of the tympanic membrane in combination with any type of ossiculoplasty procedure that does not preserve the integrity of the malleoincudal lever mechanism. Type III tympanoplasty includes the vast majority of techniques described for routine ossicular chain reconstruction. Accordingly, type III tympanoplasty classification has been further subdivided according to ossiculoplasty technique.
Stapes Columella Subtype
This type III tympanoplasty involves placement of a tympanic membrane graft directly onto the superstructure of the stapes without the use of a prosthesis or any other substantial interpositional material.
Minor Columella Subtype
This involves the use of an interpositional graft or prosthesis to establish continuity between the tympanic membrane and the superstructure of the stapes. Examples of this include the use of a synthetic partial ossicular replacement prosthesis (PORP) or sculpted ossicular (incus or malleus head) autograft. Interpositional ossiculoplasty techniques that employ a lateral contact point with the malleus manubrium also fall within this subtype.
Major Columella Subtype
This procedure is exactly the same as the minor columella subtype except that the stapes superstructure is absent; thus, with a major columella subtype the interpositional graft or prosthesis is set upon the stapes footplate. An example of this is use of a synthetic total ossicular replacement prosthesis (TORP). Tympanoplasty with delayed staged ossiculoplasty that consists of a malleus-grip stapedotomy could also be considered to fall within this subtype.
Type IV Tympanoplasty
This procedure involves repair of the tympanic membrane in such a manner that the boundary between the mucosalized middle ear space and the epithelialized lateral compartment (external auditory canal, open mastoid cavity, epitympanum) is shifted in a way that renders the stapes footplate externalized as part of the latter. As a result, the tympanic cavity is divided into a smaller-than-normal aerated space in continuity with the eustachian tube, termed the cavum minor, in which the round window is acoustically shielded, and an external component in which the mobile stapes footplate is covered by a thin epithelial layer and is directly exposed to incoming sound energy.
Type V Tympanoplasty
This procedure is the same as the type IV tympanoplasty, except that it also includes the need to address an underlying immobile stapes footplate and, therefore, is generally performed in a staged manner once active infectious disease is controlled. Historically, fenestration of the lateral semicircular canal was described as part of this procedure to counteract stapes fixation; however, total footplate removal and a soft tissue seal have generally replaced fenestration.
PHYSIOLOGY: MECHANISMS OF GAIN
The modern view of middle ear acoustic science involves two basic pathways by which sound is able to stimulate the inner ear (3, 4). The first involves transmission of sound pressure through the tympanic membrane and ossicular chain via the oval window. This is known as ossicular coupling. This mechanism is the primary means by which the state of impedance mismatch that exists between the air in the ear canal (low impedance) and the fluid within the cochlea (high impedance) is overcome. In such a state, sound pressure is deflected during passage through the air-fluid interface, resulting in a loss of gain in the realm of 30 dB. The coupling effect of the tympanic membrane and ossicles almost overcomes this loss.
Ossicular coupling has been attributed to the collective effect of three characteristics of the tympanoossicular mechanism traditionally known as the acoustic transformer theory (5). The first and most significant of these characteristics is the hydraulic lever effect that results from the difference between the surface area of the tympanic membrane relative to that of the oval window (usually a ratio of nearly 21:1). This effect results in compression of sound energy and increase in force at the oval window, equating to a theoretic approximate increase in gain of 26 dB. The second characteristic is the malleoincudal lever effect that results from the difference in length between the malleus manubrium relative to that of the long process of the incus along the axis of ossicular rotation (a ratio of 1.3:1). However, this effect only accounts for an additional 2 dB theoretical increase in gain. The final factor is the so-called catenary lever effect that is generated by the elastic stretching of the tympanic membrane from the annulus to the malleus manubrium—somewhat akin to the stretched strings across a tennis racquet. The specific degree of acoustic benefit derived from the catenary effect is not well understood but probably lies within a range similar to that of the malleoincudal lever.
It is important to recognize that, in reality, ossicular coupling is a much more complex phenomenon than what is suggested by these simplified traditional models as they do not account for factors such as variation in efficiency with changes in frequency or inefficiencies in sound transmission through the tympanic membrane and ossicular chain attributed to the inherent tension or laxity of the ossicular ligaments. Thus, it is perhaps not surprising that the 25 to 30 dB of gain that is predicted by the acoustic transformer theory does not equate well with experimental
measurements, which suggest an actual more modest increase in the realm of just over 20 dB (6, 7, 8).
measurements, which suggest an actual more modest increase in the realm of just over 20 dB (6, 7, 8).
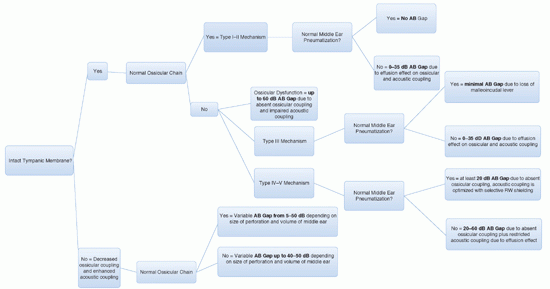
The second pathway of sound stimulation of the inner ear involves direct passage of sound pressure via the oval and round windows without involvement of the tympanic membrane or ossicular chain. This is known as acoustic coupling (4). Given an intact tympanic membrane and functional ossicular chain, this pathway is of only minor importance. However, in the various conditions of a diseased ear, acoustic coupling can be important. This is why, for example, a conductive hearing loss will be greater in the case of ossicular discontinuity and an intact tympanic membrane (60 dB) compared with ossicular discontinuity and an absent tympanic membrane (40 to 50 dB). With the former, the intact tympanic membrane restricts the acoustic coupling pathway by blocking direct access of sound pressure to the oval and round window membranes.
A final relevant consideration in middle ear acoustic mechanics is that of phase. A sound stimulus to the inner ear is detected as the net difference in sound pressures applied to the round and oval windows that results in movement of intracochlear fluids. If these sound pressures are simultaneously applied to the round and oval windows with equal amplitude and phase, they will counteract each other and no resultant intracochlear fluid displacement will occur. In the normal situation, this does not occur due to the unbalanced selective effect of ossicular coupling upon the oval window, the acoustic shielding effect of the tympanic membrane upon the round window, and the uneven anatomical positioning of the round window versus the oval widow relative to incoming sound. However, when the tympano-ossicular mechanism is absent and acoustic coupling is primarily relied upon (as in the case of a type IV or V tympanoplasty), an unshielded round window can yield significant negative acoustic consequences due to phase cancellation (4).
A simplified chart depicting the theoretic ideal acoustic effects of various tympano-ossicular scenarios is shown in Table 153.1.
PREOPERATIVE EVALUATION
When a patient is considered for tympanoplasty or ossiculoplasty, a thorough history, examination, and audiometric evaluation should be performed on both ears. Otoscopy and pneumatic insufflation under the binocular microscope, following careful removal of debris, provide a wealth of information. The results of the audiogram should always be correlated with the physical exam, including Weber and Rinne tuning fork tests, especially when a masking dilemma is present. If the audiogram and tuning fork exam do not agree, surgery should not be performed until this is reconciled.
A preoperative audiogram can be helpful in suggesting underlying pathology. Generally, a perforation will cause a conductive hearing loss between 5 and 40 dB depending on its characteristics (9). Controversy exists as to whether or not the location of a perforation impacts the degree of hearing loss, yet perforation size and underlying middle ear volume do matter (an ear with a smaller volume tends to have worse hearing than one with a larger volume, even given identical perforations).
When the tympanic membrane is intact, a conductive hearing loss greater than 35 to 40 dB strongly suggests the possibility of ossicular chain dysfunction. Furthermore, the pattern of hearing loss may be typical of particular scenarios; for example, ossicular fixation generally causes a low-tone conductive hearing loss, the degree of which is related to the extent and location of the fixation. With malleus head fixation, the low-tone air-bone gap generally closes at the higher frequencies, whereas stapes fixation tends to affect the middle and high frequencies to a relatively greater degree (10).
The status of the eustachian tube will impact surgical outcomes, yet there is no consensus on the optimal way to reliably assess its function (11). Auto-inflation using the Valsalva or Toyenbee maneuver is helpful, albeit a nonphysiologic test of tubal patency. The clinical status of the contralateral ear likewise can provide insight into tubal maturity and function in the diseased ear (12). As part of the eustachian tube evaluation, the nose should be examined so that allergy, adenoiditis, and rhinosinusitis can be treated in an effort to promote optimized tubal function (13). Furthermore, aggressive medical treatment of infection involving the ear itself should be undertaken prior to surgery, including aural toilet and ototopical agent application. When an ear will not dry with medical therapy, culture acquisition may be useful in helping to identify antimicrobial-resistant pathogens.
Once patient assessment is complete, a few general rules should be applied to surgical candidacy. First, one should avoid elective surgery on an only-hearing ear as much as is reasonably possible. Exceptions to this would be situations where surgery is primarily confined to the tympanic membrane, and drilling or significant ossicular manipulation is unlikely, or when a perforation is contributing to difficulty with hearing aid usage. Also, cases that involve disease processes that impart risk of hearing loss, such as cholesteatoma, will generally warrant intervention. Second, when bilateral disease is present, surgery should be undertaken on the worse-hearing ear in the absence of any other compelling reason to do otherwise on account of underlying disease. Finally, special consideration should be given to the timing of surgery in the pediatric patient.
Age as a prognostic factor in tympanoplasty is controversial, with contradicting reports present in the literature (14, 15). The authors’ approach to pediatric patients is to avoid repairing the tympanic membrane during the otitis-prone years (≤3 years). If the contralateral ear is normal, routine tympanoplasty is considered at age 4 for an ear that is dry or only occasionally drains with water
contamination (16). However, if the contralateral ear is abnormal at this time, adenoidectomy is considered and tympanoplasty is deferred until the contralateral ear reaches stable quiescence or the patient reaches age 7. If contralateral disease is still present at this time, a more aggressive technique, such as cartilage tympanoplasty, is performed on the worse-hearing ear. The second ear is repaired several months later, but only after the first ear is documented to have a stable satisfactory outcome and is not expected to require further surgery.
contamination (16). However, if the contralateral ear is abnormal at this time, adenoidectomy is considered and tympanoplasty is deferred until the contralateral ear reaches stable quiescence or the patient reaches age 7. If contralateral disease is still present at this time, a more aggressive technique, such as cartilage tympanoplasty, is performed on the worse-hearing ear. The second ear is repaired several months later, but only after the first ear is documented to have a stable satisfactory outcome and is not expected to require further surgery.
TABLE 153.1 THEORETIC IDEAL ACOUSTIC EFFECTS OF VARIOUS TYMPANO-OSSICULAR SCENARIOS | |
|---|---|
|
TYMPANOPLASTY
General Principles
Modern tympanoplasty techniques all have common ground in that they endeavor to reconstruct the deficient middle fibrous layer of a tympanic membrane perforation with graft materials that then act as a scaffold for lateral epithelial growth. Although simplified myringoplasty techniques that utilize non-grafted temporary scaffold materials, such as a thin paper patch, can be used for small perforations, they are relatively limited in application and simple to learn. Thus, patch myringoplasty techniques are not a focus of this discussion.
The common goals of tympanic membrane repair are to
Create a barrier between the dry lateral epithelialized compartment (drumhead, external auditory canal, open mastoid cavity) and the moist medial mucosalized compartment (middle ear, eustachian tube)
Provide reinforcement to correct tympanic membrane weaknesses in order to resist future disease processes (atelectasis, perforation)
Create an optimized sound-conducting platform for ossicular coupling or a round window shield for acoustic coupling depending on tympanoplasty type
Create a contour favorable for outward keratin debris migration
Applied Tympanic Membrane Mechanics
The tympanic membrane is the major element of the middle ear transformer mechanism and acts as a barrier between the sound pressure of the ear canal and middle ear. Its motion, which has been studied with laser vibrometry and stroboscopic holography, is both complex and variable depending on the frequency of stimulation (17, 18). At frequencies up to 1,000 Hz, the tympanic membrane tends to vibrate in one consolidated phase, but as frequency rises further, its vibration splits into a state of phase subdivision, with overall diminished efficiency.
While it is intellectually satisfying to assert that reconstruction of the tympanic membrane must endeavor to exactly recreate these native vibratory patterns, in truth it is unknown if this is possible or even necessary. Numerous tympanic membrane graft materials have been used that are quite dissimilar to the native drumhead in rigidity and thickness, yet excellent acoustic outcomes have been attained. For example, reconstruction with large cartilage grafts has been reported to result in hearing outcomes equal to those with more pliable temporalis fascia (15, 19, 20, 21), including occurrences of complete air-bone gap closure in the speech frequencies. Further complicating the situation is uncertainty regarding the interplay between an aphysiologic reconstructed tympanic membrane and the underlying aphysiologic reconstructed ossicular chain in collectively providing acoustic gain (22). Gaps between observed clinical outcomes and predicted tympanoplasty outcomes based on tympanic membrane acoustic models highlight the fact that there is still much to be learned.
Surgical Exposure
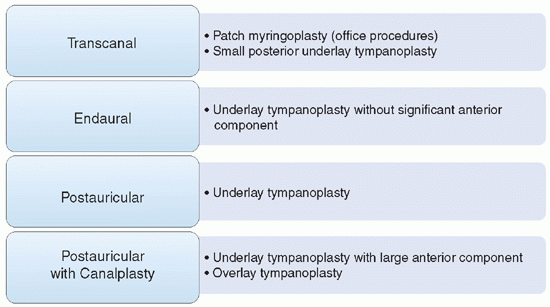
The importance of assuring proper visualization and exposure in order to surgically manipulate the tympanic membrane and middle ear may seem obvious, but if taken for granted, surgical results can be compromised. Line-of-sight visualization in itself does not always signify adequate exposure. The surgeon must assure that instruments are allowed to enter the microscopic field at a sufficiently open lateral angle so as not to impede binocular vision or require awkward manipulation. Although minimally invasive approaches can be desirable, these should only be utilized if they provide equally sufficient access and exposure to the surgical target. The morbidity associated with even the widest tympanoplasty access route (postauricular with canalplasty) is generally not high. Table 153.2 provides a suggested guide for choosing appropriate access for tympanic membrane repair. One noteworthy consideration is that when a perforation involves the anterior drumhead, wide exposure via a postauricular incision and, when needed, a canalplasty may be helpful.
Canal Incisions
Numerous sites for canal incisions have been described to raise a tympanomeatal flap, and generally these are chosen according to the anticipated surgical plan. Many surgeons have traditionally insisted upon preservation of the posterior -superior “vascular strip” of canal skin or avoidance of transecting the tympanic annulus. However, many of these dictums seem to be routinely ignored by accomplished otologists with little if any apparent negative consequence. In reality, quality surgical execution and careful atraumatic handling of canal skin are probably the key factors to a successful outcome regardless of how this is done (see Fig. 153.1).
Preparing the Drumhead
Prior to graft placement, the tympanic membrane should be prepared to maximize the chances of graft take and rapid epithelialization. This typically involves
freshening the margins of the perforation with cold knife rim resection or laser application in order to encourage sprouting of new microvasculature. As a general rule, it is better to be aggressive in completely removing unhealthy portions of the tympanic membrane than to attempt incorporation of them into the reconstruction process. This includes myringitis (particularly important), tympanosclerotic plaque, scar, and old graft material. Pathologic adhesions between the drumhead and middle ear should also be released.
freshening the margins of the perforation with cold knife rim resection or laser application in order to encourage sprouting of new microvasculature. As a general rule, it is better to be aggressive in completely removing unhealthy portions of the tympanic membrane than to attempt incorporation of them into the reconstruction process. This includes myringitis (particularly important), tympanosclerotic plaque, scar, and old graft material. Pathologic adhesions between the drumhead and middle ear should also be released.
TABLE 153.2 SUGGESTED ROUTES OF ACCESS FOR TYMPANIC MEMBRANE REPAIR | |
|---|---|
|
Choosing, Preparing, and Shaping the Graft
The most commonly used tympanic membrane grafting material is temporalis fascia, which is desired for its pliability. This is harvested, via either an endaural or postauricular incision, as the glistening whitish layer of fascia immediately overlying the temporalis muscle fibers. After harvest, this is generally pressed thin and set aside for drying, which may promote ease of trimming and placement. Readily available alternatives to temporalis fascia that are also thin and pliable include pressed perichondrium, periosteum, and muscle. Cadaveric acellular dermal matrix (AlloDerm, LifeCell Corp, Branchburg, NJ) (23) has also been used with success and may be particularly useful for simple in-office tympanoplasty procedures where harvest of a tissue graft is not desired.
Auricular cartilage grafts are very useful in tympanoplasty (24, 25) and may be harvested from various sites, but are typically harvested from the tragus and the cymba with the overlying perichondrium intact. These can be applied with or without perichondrium or the concurrent use of fascia; however, the authors’ bias is to apply cartilage grafts that have been stripped of perichondrium on the medial surface but have adherent perichondrium or overlying fascia on the lateral surface (26). In the authors’ experience, such grafts tend to be much more resistant to involvement with postoperative middle ear adhesions than either fascia or perichondrium.
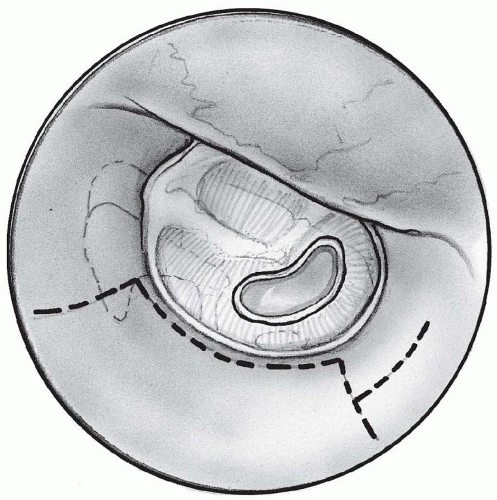 Figure 153.1 Canal incisions. A: The classic vascular strip incision involves preservation of the posterior canal skin to within a few millimeters of the annulus. |
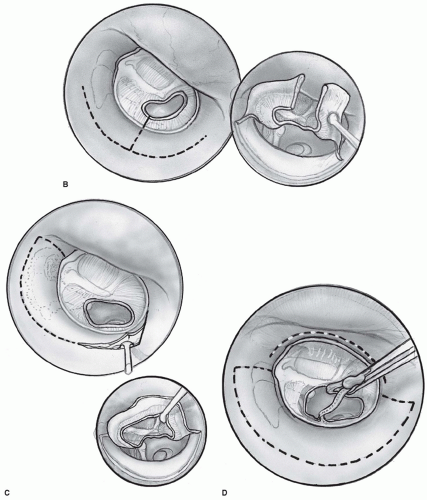 Figure 153.1 (Continued) B: A “book page” flap provides particularly good access for graft placement by dividing the annulus with an incision through the canal skin and tympanic membrane into the perforation. C: A “ship sail” flap is larger at the superior aspect and is particularly useful when wide curettage of scutum bone results in the need for extra tympanomeatal flap length for coverage. D: Modified canal incisions for underlay tympanoplasty can incorporate both a standard tympanomeatal flap as well as a separate anterior canal incision to elevate the annulus and anchor the graft. (Continued on next page) |
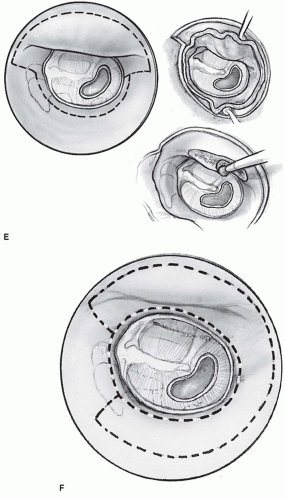 Figure 153.1 (Continued) E: Overlay tympanoplasty requires incisions that afford removal of the anterior canal wall skin to allow access for canalplasty. F: Overlay tympanoplasty incisions can be modified to allow wider removal of canal skin if desired. |
When the use of a composite perichondrium-cartilage island graft is desired, perichondrium is usually stripped off of one side, and the remaining cartilage is cut to the desired shape as an “island” upon the preserved opposite side (see Fig. 153.2). If used for repair of a large perforation, a composite island graft is shaped into a thin circular disk 8 to 9 mm in diameter, with a notch cut to cradle the malleus manubrium and tails of perichondrium on the periphery that can be anchored on the external auditory canal wall under the annulus. For optimized acoustics, a cartilage graft thickness of 0.7 mm or less is preferable; however, if shaved too thin, undesirable curling of the graft may occur.
The choice of graft material is made based on the complexity of the reconstruction and the activity of any underlying chronic ear disease. In higher risk situations, cartilage tympanoplasty techniques may provide more durable results (27, 28). A high-risk perforation might be considered one that is larger than 50%, an anterior perforation, a perforation draining at the time of surgery, a recurrent
perforation (29, 30), or a perforation in the setting of permanent absent eustachian tube function. Other situations where cartilage is useful are the atelectatic ear, retraction pockets, and cholesteatoma as re-atrophy and perforation are common over the long term when fascia is used solely in the reconstruction (31).
perforation (29, 30), or a perforation in the setting of permanent absent eustachian tube function. Other situations where cartilage is useful are the atelectatic ear, retraction pockets, and cholesteatoma as re-atrophy and perforation are common over the long term when fascia is used solely in the reconstruction (31).
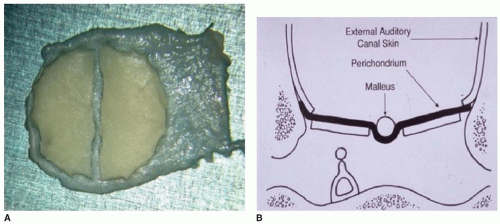 Figure 153.2 Composite perichondrium-cartilage island graft. A: A composite perichondrium-cartilage island graft is formed by stripping perichondrium off a single side of the graft. The cartilage is then cut to the desired shape and size without violating the remaining perichondrium. For total tympanic membrane reconstruction, the preferred diameter of the graft is 8 to 9 mm. A 1-mm central strip of cartilage is removed to accommodate the malleus handle and to allow posterior graft elevation for ossiculoplasty. The remaining peripheral perichondrial “apron” is set over the canal wall bone. B: Cross section of a perichondrium-cartilage island used as an underlay graft. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


