Purpose
To report a novel method for measuring the degree of inferior oblique muscle overaction and to investigate the correlation with other factors.
Design
Cross-sectional diagnostic study.
Methods
One hundred and forty-two eyes (120 patients) were enrolled in this study. Subjects underwent a full orthoptic examination and photographs were obtained in the cardinal positions of gaze. The images were processed using Photoshop and analyzed using the ImageJ program to measure the degree of inferior oblique muscle overaction. Reproducibility or interobserver variability was assessed by Bland-Altman plots and by calculation of the intraclass correlation coefficient (ICC). The correlation between the degree of inferior oblique muscle overaction and the associated factors was estimated with linear regression analysis.
Results
The mean angle of inferior oblique muscle overaction was 17.8 ± 10.1 degrees (range, 1.8–54.1 degrees). The 95% limit of agreement of interobserver variability for the degree of inferior oblique muscle overaction was ±1.76 degrees, and ICC was 0.98. The angle of inferior oblique muscle overaction showed significant correlation with the clinical grading scale (R = 0.549, P < .001) and with hypertropia in the adducted position (R = 0.300, P = .001). The mean angles of inferior oblique muscle overaction classified into grades 1, 2, 3, and 4 according to the clinical grading scale were 10.5 ± 9.1 degrees, 16.8 ± 7.8 degrees, 24.3 ± 8.8 degrees, and 40.0 ± 12.2 degrees, respectively ( P < .001).
Conclusions
We describe a new method for measuring the degree of inferior oblique muscle overaction using photographs of the cardinal positions. It has the potential to be a diagnostic tool that measures inferior oblique muscle overaction with minimal observer dependency.
Overelevation in adduction can be observed in multiple causes, such as inferior oblique muscle overaction, Duane syndrome, and dissociated vertical divergence. Among them, inferior oblique muscle overaction is a common ocular motility disorder characterized by vertical incomitance of the eye in lateral gaze. Primary inferior oblique muscle overaction often develops during childhood in patients with infantile esotropia, accommodative esotropia, or intermittent exotropia, whereas the secondary type is related to palsy of the superior oblique muscle.
Various surgical procedures have been performed to correct inferior oblique muscle overaction, including myectomy, recession, extirpation, and anteriorization of the inferior oblique muscle. The surgical technique depends on the deviation in central gaze, the amount of elevation in adduction, and the pattern of comitance; however, the decision of the surgical plan appears to be primarily based on individual experience and preference. Moreover, an objective measurement of inferior oblique muscle overaction remains a difficult task in clinical practice.
We previously described a modified limbus test that quantifies the angle of ocular movement using photographs of the 9 cardinal positions of gaze. This technique allows measurement of not only the angle of ocular movement but also the axis of direction in the 9 cardinal positions of gaze.
The purpose of this study was to describe a new clinical technique for measuring the degree of inferior oblique muscle overaction and to evaluate its performance in patients with inferior oblique muscle overaction.
Methods
This was a cross-sectional study in which patients with inferior oblique muscle overaction were enrolled from October 1, 2011 to October 31, 2013. Institutional review board approval was obtained at Hanyang University Guri Hospital, and the study adhered to the Declaration of Helsinki and Health Insurance Portability and Accountability Act regulations. Written informed consent was obtained from all patients or from 1 or both parents for children younger than 18 years of age.
Patients
Patients enrolled in this study had inferior oblique muscle overaction associated with intermittent exotropia, congenital esotropia, and superior oblique muscle palsy. All patients received full ophthalmologic and orthoptic assessments, including history, best-corrected visual acuity, ductions and versions, posterior segment examination, cycloplegic refraction, cover test, and measurement of deviation in the diagnostic positions of gaze near and at distance by loose prism and the alternate cover test. In younger patients, deviation was measured by means of Krimsky test or Hirschberg test. Ductions and versions were graded on a scale of −4 (underaction) to +4 (overaction), with 0 being normal. Inferior oblique muscle overaction was determined by measuring vertical deviation on maximal lateral version. A vertical deviation of approximately 10 degrees was +1, 20 degrees was +2, 30 degrees was +3, and 40 degrees was +4. Two independent ophthalmologists with more than 10 years of clinical experience examined the patient and graded the rating scale of inferior oblique muscle overaction. When there were disagreements between observers for the rating scale of inferior oblique muscle overaction, the observers would discuss their reasons for selecting a particular grade and then, if necessary, reexamine the patient together so that any disparity was clarified. Subjects were excluded from the study if they did not cooperate with all tests. Cases with ocular, neurologic, chromosomal, or congenital disease or a history of previous extraocular muscle surgery were excluded from the study.
Photographs of the 9 Cardinal Positions of Gaze
Photographs were obtained at a distance of 1 m from the subject using a 36.8 megapixel digital single-lens reflex camera (D800; Nikon Inc, Tokyo, Japan) with a ring flash attached to the lens. The resolution of all selected images was 5520 × 3680 pixels. The subject’s head was firmly fixed on a chin rest with a band wound around the head to prevent head movements, and the subject looked at a fixation target located 6 m away. The subject was then instructed to immobilize his or her head with the eyes in the primary position. Head position was examined to confirm the absence of obvious tilt or chin-up or chin-down position. To obtain photographs of the primary position of each eye, we took a photograph of each eye fixated on a 6 m target with occlusion of the contralateral eye. Next, a Lancaster screen was installed at a distance of 1 m from the subject, and the subject visually tracked the fixation target along the axis of the Lancaster screen into maximum dextro-supraversion, supraversion, levo-supraversion, levoversion, dextroversion, dextro-infraversion, infraversion, and levo-infraversion for photographs of the secondary and tertiary positions ( Figure 1 ). Verbal encouragement was used to ensure stability of the head and maximum effort into the extremes of gaze.
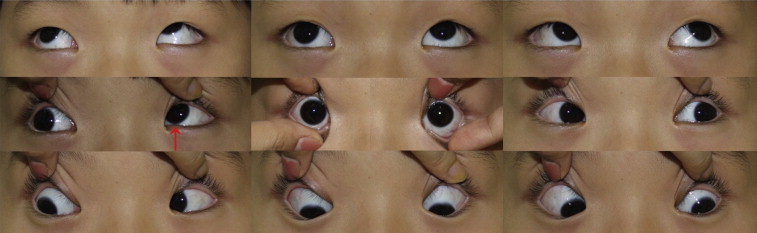
Image Processing Procedures
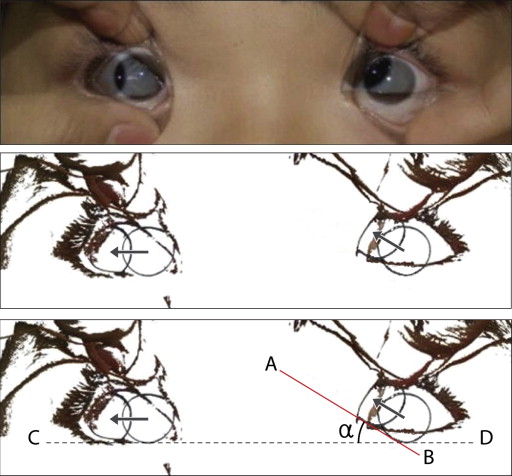
After photographs of the 9 cardinal positions were collected, the images were processed using Photoshop 6.0 (Adobe, San Jose, California, USA). The digital image of the primary position was first opened in Photoshop. The secondary or tertiary position image was then selected and copied to the clipboard, and the contents of the clipboard were pasted onto the image of the primary position to create a separate layer. The pasted layer was converted to a semitransparent image to help achieve better overlap with the image of the primary position ( Figure 2 , Top). Using the blending tool, the respective layer’s light or dark portions were converted to a transparent portion; this was done to identify the margin of the corneal limbus ( Figure 2 , Middle). The resulting image was then saved as a TIFF file with no layers.
Measurement of the Degree of Inferior Oblique Muscle Overaction
The degree of inferior oblique muscle overaction was defined as the angle between the directions of the visual axis of 2 eyes in the lateral gaze. It was measured using the angle between a horizontal line and the tangent line, which corresponded to the direction of ocular movement in the adducted position ( Figure 2 , Bottom). To quantify these angles, the processed image was loaded into the ImageJ program (software version 1.46; National Institutes of Health, Bethesda, Maryland, USA). The angle made by the line joining A and B with the horizontal in Figure 2 , Bottom was measured by the measuring tools in ImageJ. For simplicity, we assumed that the line joining C and D was on a horizontal line. Thus, the angle of inferior oblique muscle overaction is the angular amount in the 2 lines that is α. To determine interobserver reliability, 2 independent observers (H.W.L. and J.W.L.) measured the degree of inferior oblique muscle overaction using the above method.
Statistical Analysis
Statistical analyses were performed using SPSS for Windows version 17.0 (SPSS, Inc, Chicago, Illinois, USA) and the MedCalc statistical packages (V.12.7; MedCalc Statistical Software, Ostend, Belgium). The intraclass correlation coefficient (ICC) was calculated to analyze interobserver variation. Agreement between measurements is represented in Bland-Altman plots. Linear regression analysis was performed to assess the relationship between the angle of inferior oblique muscle overaction and the clinical grading scale, hypertropia in the primary position, and hypertropia in the adducted position. Subgroup analyses based on the type of inferior oblique muscle overaction were conducted using an independent sample t -test. One-way analysis of variance (ANOVA) was used to compare the mean angle of inferior oblique muscle overaction between 4 subgroups of the clinical grading scale. P values less than .05 were considered statistically significant.
Results
A total of 127 patients were investigated during the study period. Seven of these 127 patients were excluded, 5 because of incomplete data sets and 2 because of an inability to comply with the modified limbus test owing to small lid fissures. Thus, 142 eyes of 120 patients (60 men) with a mean age of 11.2 ± 10.8 years (range, 3–62) were included. Of these, 102 had secondary inferior oblique muscle overaction attributable to superior oblique muscle palsy with a positive Bielschowsky head-tilt test, while 40 had primary inferior oblique muscle overaction associated with intermittent exotropia (n = 25), accommodative esotropia (n = 13), and congenital esotropia (n = 2).
Demographics and characteristics of the patients are shown in Table 1 , together with a comparison between patients with primary inferior oblique muscle overaction and secondary inferior oblique muscle overaction. Compared with primary inferior oblique muscle overaction, patients with secondary inferior oblique muscle overaction were older ( P = .008), were myopic ( P = .024), and had greater hypertropia in the primary position ( P < .001) and adducted position ( P = .024). There were no significant differences in the degree of inferior oblique muscle overaction measured by the clinical grading scale ( P = .073).
| Total | Primary IOOA (n = 23) | Secondary IOOA (n = 97) | P Value | |
|---|---|---|---|---|
| Age (y) | 11.2 ± 10.8 (3∼62) | 5.9 ± 2.8 | 12.4 ± 11.5 | .008 a |
| Gender (male/female) | 60 (72 eyes)/60 (70 eyes) | 12/11 | 48/49 | .818 b |
| Spherical equivalent (D) | −0.18 ± 1.71 (−11.0∼4.0) | 0.45 ± 1.06 | −0.48 ± 1.89 | .024 a |
| HT in the primary position (PD) | 6.7 ± 6.5 (0∼30) | 1.8 ± 5.3 | 8.1 ± 5.9 | <.001 a |
| HT in the adducted position (PD) | 9.6 ± 8.1 (0∼40) | 5.7 ± 6.3 | 10.9 ± 8.4 | .024 a |
| Grading scale of IOOA | 2.1 ± 0.7 (1∼4) | 2.3 ± 0.8 | 2.0 ± 0.7 | .073 a |
| Angle of IOOA (degrees) | 17.8 ± 10.1 (1.8∼54.1) | 19.1 ± 11.0 | 17.8 ± 9.9 | .590 a |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


