Purpose
To determine the frequency of neovascularization subtypes as determined by fluorescein angiography (FA) alone vs FA and optical coherence tomography (OCT) grading in age-related macular degeneration (AMD).
Design
Retrospective cohort.
Methods
participants : Newly diagnosed neovascular AMD patients who initiated intravitreal anti–vascular endothelial growth factor therapy by 1 physician from October 1, 2005 to December 1, 2012. interventions : Two independent graders classified the baseline lesions using FA alone and FA+OCT. main outcome measures : Analysis of the frequency of lesion subtypes by FA alone or FA+OCT and agreement between both classification systems was performed.
Results
A total of 232 patients (266 eyes) fit the inclusion criteria. Mean age was 86.3 years; 67.7% of eyes (180/266) were from female patients, and 95.5% (254/266) were from white patients. The distribution using FA alone was 49.6% (132/266), 12.0% (32/266), 28.6% (76/266), and 9.8% (26/266) among occult, classic, retinal angiomatous proliferation, and mixed choroidal neovascularization, respectively. With FA+OCT, 39.9% (106/266), 9.0% (24/266), 34.2% (91/266), and 16.9% (45/266) were type 1 (sub–retinal pigment epithelium), type 2 (subretinal), type 3 (intraretinal), and mixed neovascularization (NV), respectively. The κ statistic was 0.65 (standard error ±0.37, P < .001) between the 2 classification systems, representing good agreement.
Conclusion
With both FA-alone and FA+OCT grading, we found a higher incidence of type 3 NV in eyes with newly diagnosed neovascular AMD than that reported in prior studies. The κ statistic between the 2 classification systems showed “good” agreement. The discrepancies are likely attributable to the identification of a higher frequency of type 3 and mixed NV and a lower frequency of type 1 NV with the aid of OCT.
Age-related macular degeneration (AMD) is the most common cause of irreversible central vision blindness among individuals older than 50 years of age in the developed world, and while neovascular AMD represents only 10%–15% of AMD eyes, it is responsible for more than 80% of cases of severe visual loss attributable to retinal exudation, hemorrhage, and disciform scarring. The most commonly used classification of neovascular AMD was first developed for the Macular Photocoagulation Study (MPS) in 1991. It was based on the only available imaging modality at that time, fluorescein angiography (FA). It characterized lesion subtypes as “classic” or well-defined choroidal neovascularization (CNV) and “occult” or poorly defined CNV. Subsequently, this classification scheme was important in determining treatment response in the first pivotal trials with photodynamic therapy and, more recently, in selecting eligible patients and monitoring their response to treatment in the major anti–vascular endothelial growth factor (VEGF) trials. The FA classification system has continued to be used for enrollment into subsequent neovascular AMD treatment trials.
High-definition spectral-domain optical coherence tomography (OCT) has been developed with an axial resolution as high as 7 μm and offers near histologic visualization of the retina. Current treatment paradigms continue to use OCT imaging to monitor response to anti-VEGF therapy. Additional subtypes of neovascular AMD, such as polypoidal choroidal vasculopathy (PCV) and retinal angiomatous proliferation (RAP), have been further detailed with the use of OCT. With the availability of these advancements in imaging, a new classification scheme of neovascularization (NV) based on anatomic localization with multimodal imaging including FA and OCT has been proposed, expanding upon Grossniklaus and Gass’ original observations from histopathologic slides of neovascular AMD.
The first purpose of this study was to evaluate the frequencies of newly diagnosed lesion subtypes in neovascular AMD in treatment-naïve patients presenting to 1 retinal physician (K.B.F.) over a 6-year time period using both the original FA classification system as originally defined by the MPS and the anatomic classification with multimodal imaging combining both FA and OCT. The second purpose of the study was to compare the 2 systems and to assess the agreement between the 2 classification systems.
Methods
This retrospective cohort study design was approved by the Western Institutional Review Board (Olympia, Washington, USA). It complied with the Health Insurance Portability and Accountability Act of 1996 and followed the tenets of the Declaration of Helsinki.
Data Collection
We retrospectively reviewed the charts and imaging data of 374 consecutive patients diagnosed with treatment-naïve neovascular AMD between October 1, 2005 and December 1, 2012. Treatments with ranibizumab (0.5 mg/0.05 mL; Lucentis, Genentech, San Francisco, California, USA), bevacizumab (1.25 mg/0.05 mL, Avastin; Genentech), or aflibercept (2.0 mg/0.05 mL, Eylea; Regeneron, Tarrytown, New York, USA) were administered by a single physician (K.B.F.).
Inclusion criteria were similar to the Minimally Classic/Occult Trial of the Anti-VEGF Antibody Ranibizumab in the Treatment of Neovascular Age-Related Macular Degeneration (MARINA) and Anti-VEGF Antibody for the Treatment of Predominantly Classic Choroidal Neovascularization in Age-Related Macular Degeneration (ANCHOR) study groups. All participants were older than 50 years with newly diagnosed treatment-naïve NV as evidenced by clinical examination and FA. Best-corrected visual acuity was 20/20–20/800 on a Snellen chart (differed from ANCHOR/MARINA, which included 20/40–20/320 on the Early Treatment Diabetic Retinopathy Study charts). Additionally, eyes in the study must have had OCT imaging (time-domain or spectral-domain) performed at the time of diagnosis.
Exclusion criteria were any of the following: previous treatments for CNV in the study eye, including photodynamic therapy (PDT), intravitreal steroids, intravitreal pegaptanib (Macugen; Valeant, Montreal, Quebec, Canada), or thermal laser and eyes with CNV lesions presenting with subfoveal fibrosis, central geographic atrophy (GA) at baseline, or retinal pigment epithelial tears, or composed of more than 50% hemorrhage. Eyes with CNV secondary to other maculopathies, including degenerative myopia, angioid streaks, presumed ocular histoplasmosis syndrome, or inflammatory maculopathies, were excluded.
Demographic information including age; sex; race; family history of AMD, smoking status (current, former, never), history of hypertension and diabetes, history of statin, aspirin, clopidogrel, and/or warfarin use, and history of glaucoma were collected for each patient.
FA images were obtained using a Topcon TRC 501x fundus camera (Topcon Imagenet, Tokyo, Japan). OCT imaging of all patients was performed with time-domain OCT (Stratus; Carl Zeiss Meditec Inc, Dublin, California, USA) or spectral-domain OCT (Spectralis; Heidelberg Engineering, Heidelberg, Germany; or 3-D OCT-2000; Topcon, Tokyo, Japan). OCT instrumentation was necessary for additional accurate identification of lesion subtype utilizing the anatomic classification of lesion subtype. Standard methods of image acquisition were employed for all imaging modalities.
Image Grading
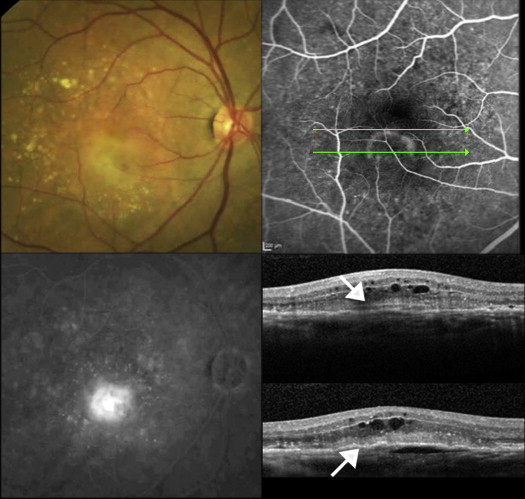
The classification of neovascular lesions was made independently by 2 experienced retina specialists (S.M. and R.G.P.) who evaluated the presenting color photographs, FA, and OCT. First, all the color photographs and FA corresponding to the baseline diagnostic visit were analyzed. Neovascular lesions were subtyped according to the MPS criteria and the Digital Angiographic Reading Center (DARC) Reader’s Manual as occult or classic CNV, and RAP lesions were identified by criteria defined by Yannuzzi and associates and the DARC Reader’s Manual. Secondly, OCT images corresponding to the same diagnostic visit were reviewed, and each case was classified according to the guidelines provided by Freund and associates. The anatomic classification, which uses OCT in combination with FA, categorizes lesions as type 1 (sub–retinal pigment epithelium [RPE]), type 2 (subretinal), type 3 (intraretinal), or mixed NV. Eyes with PCV were considered to be a form of type 1 CNV. Type 1, 2, and 3 NVs corresponded to occult, classic, and RAP angiographic lesions, respectively. Cases with multiple lesion types were identified as mixed NV and each component was also recorded. Table 1 provides further details of the criteria of CNV subtype classification based on each imaging modality. Finally, in cases with disagreement between FA and OCT findings ( Figure 1 ), FA images were reanalyzed focusing on early frames to better recognize subtle angiographic findings, in particular those of RAP lesions. A third supervising grader (K.B.F.) evaluated the lesion type in the presence of significant discrepancies.
| CNV | Color & Red-free Photographs | FA Early | FA Late | OCT |
|---|---|---|---|---|
| Type 1 | RPE elevation with irregular height and shape; pigment mottling | Stippled hyperfluorescence within 1 or 2 minutes (fibrovascular PED), or lack of early hyperfluorescent signal (late leakage of undetermined source) | Mild to moderate staining and/or leakage corresponding to the RPE abnormalities | The area of staining corresponds to an elevation of the RPE line with sub-RPE material of mixed reflectivity, often with overlying subretinal fluid. Intraretinal fluid is less common. |
| Type 2 | Grayish subretinal lesion occasionally with a surrounding ring of hyperpigmentation | Early intense, well-demarcated hyperfluorescence with a characteristic lacy pattern | Intense leakage originating from the area of early hyperfluorescence | The early lacy hyperfluorescence corresponds to a linear collection of subretinal hyperreflective material directly above the RPE line. The leakage corresponds to intraretinal edema and/or subretinal fluid. |
| Type 3 | Focal intraretinal hemorrhages. Dilated right angle corkscrew-like vessels. May occur over a PED. Dilated compensatory retinal vessels. May have visible retinal-retinal anastomoses. | Early, but focal, leakage often seen in close proximity to retinal vessels. May have retinal-retinal anastomoses. | Focal intense leakage, often with cystoid macular edema | There is an intraretinal focal hyperreflective lesion in an area of localized outer retinal disruption. Often, there is a focal defect and variable degree of elevation of the underlying RPE. This intraretinal lesion corresponds to the early focal FA leakage and manifests surrounding intraretinal cystic changes. |
| Mixed variants | ||||
| Type 1 and 2 | Various combinations of findings from types 1 and 2 | Well-demarcated hyperfluorescent lacy ± surrounding area of stippled hyperfluorescence | Leakage and staining | Type 1 and Type 2 findings The area of stippled hyperfluorescence corresponds to the type 1 findings extending beyond the type 2 findings |
| Type 1 and 3 | Various combinations of findings from types 1 and 3 | Stippled hyperfluorescence ± hot spot | Staining or leakage, often with cystoid macular edema | Type 1 and type 3 findings. The area of angiographic staining corresponds to the type 1 lesion extending beyond the type 3 findings. |
| Type 2 and 3 | Various combination of findings from types 2 and 3 | Well-demarcated hyperfluorescence. No contrast of the hot spot. | Intense leakage, often with cystoid macular edema | Type 3 and type 2 findings |
Readers also graded the lesion location and overall size. FA was used to measure the greatest linear diameter (mm) and the total area of CNV lesion (mm²). Measurements were performed only on fundus camera images. The total area of CNV lesion was defined as the area of CNV leakage plus any contiguous areas of hemorrhage, blocked fluorescence, or serous PED that could be obscuring the boundaries of the CNV. The lesion location was defined as foveal (subfoveal or juxtafoveal) or extrafoveal, as determined according to the MPS terminology.
Statistical Analysis
Statistical analysis was performed using SPSS software Version 21 (SPSS, Inc, Chicago, Illinois, USA). The numbers of neovascular AMD lesions as identified by the FA classification system and by the anatomic (FA and OCT) classification system were recorded, including the breakdown of neovascular lesion components in the mixed NVs. A subgroup analysis was also performed to identify neovascular AMD lesions based on these same classification systems in the newly diagnosed neovascular AMD eyes that had baseline spectral-domain OCT (3-D OCT 2000; Topcon, Tokyo, Japan; and Spectralis; Heidelberg Engineering, Heidelberg, Germany). The κ statistic was performed to compare the agreement between both classification systems with the entire cohort and subgroup with initial spectral-domain OCT. This analysis expresses the extent to which the observed agreement exceeds that which would be expected by chance alone and is defined as follows: greater than 0.75 represents “excellent” agreement; 0.40–0.75 represents “fair” to “good” agreement; and less than 0.40 represents “poor” agreement.
The associations between FA CNV and anatomic NV classifications and each possible demographic variable were assessed individually by Fisher exact test, χ 2 test, or independent Student t test. Similarly, the associations between lesion characteristics such as size, greatest linear diameter, and location and each possible demographic variable were also analyzed. The demographic factors that were shown to have a significant association were incorporated into regression analyses as covariates when examining the associations between lesion characteristics and neovascular lesion subtypes. Adjusting for demographic confounders ensured that the observed associations between clinical characteristics and NV types were real and not attributable to demographic confounders.
Results
A total of 374 patients with treatment-naïve neovascular AMD in at least 1 eye treated with anti-VEGF therapy were identified. Among these 374 patients, 232 patients (266 eyes) met the eligibility criteria. The mean age was 86.3 ± 8.1 years; 67.7% of eyes (180/266) were from female patients and 95.5% (254/266) from white patients, followed by 2.6% (7/266) Hispanic, 1.5% (4/266) Asian, and 0.4% (1/266) African-American.
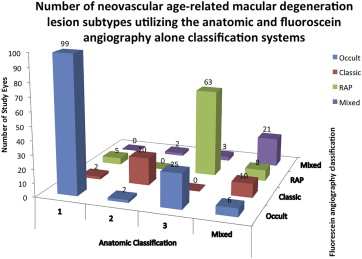
Using the FA classification system, the distribution of neovascular subtypes was 49.6% (132/266) occult CNV, 12.0% (32/266) classic CNV, 28.6% (76/266) RAP lesions, and 9.8% (26/266) mixed CNV. Of mixed lesions, 50.0% (13/26) were minimally classic, 30.8% (8/26) predominantly classic, 11.5% (3/26) occult and RAP, and 7.6% (2/26) classic and RAP. Based on anatomic classification using both FA and OCT, 39.9% (106/266) had type 1 (sub-RPE), 9.0% (24/266) type 2 (subretinal), 34.2% (91/266) type 3 (intraretinal), and 16.9% (45/266) mixed NVs. Of mixed lesions, 80.0% (36/45) were mixed 1 and 2, 15.5% (7/45) mixed 1 and 3, and 4.4% (2/45) mixed 2 and 3. Overall, there was good agreement between FA and anatomic classification with a κ statistic of 0.65 (standard error ±0.37, P < .001). When looking at each subtype individually, there was a significant increase in type 3 and mixed lesions and a decrease in type 1 subtype frequencies with the anatomic classification as compared to the FA classification ( Figure 2 ). The overall incidence of pure classic or type 2 lesions was low in both the FA and anatomic classifications.
In the subgroup that had baseline spectral-domain OCT, using the FA classification system, the distribution of neovascular subtypes was 52.9% (82/155) occult CNV, 9.0% (14/155) classic CNV, 32.3% (50/155) RAP lesions, and 5.8% (9/155) mixed CNV. Of mixed lesions, 66.7% (6/9) were minimally classic, 11.1% (1/9) predominantly classic, 11.1% (1/9) occult and RAP, and 11.1% (1/9) classic and RAP. Based on anatomic classification using both FA and spectral-domain OCT, 40.6% (63/155) had type 1, 7.1% (11/155) type 2, 40.0% (62/155) type 3, and 12.2% (19/155) mixed NVs. Of mixed lesions, 57.9% (11/19) were mixed 1 and 2, 36.8% (7/19) mixed 1 and 3, and 5.2% (1/19) mixed 2 and 3. Overall, again there was good agreement between FA and anatomic classification, with a κ statistic of 0.67 (standard error ±0.05, P < .001).
Of the demographic factors examined, age and use of warfarin were found to be significantly associated with the anatomic classification system ( Table 2 ). Age at first injection was significantly older for patients with type 3 NV (88.4 years) compared with type 1 (84.9 years), 2 (84.9 years), and mixed (86.4 years) NV, respectively. Use of warfarin was more common in study eyes with type 2 (14.3%, 3/21) and 3 (12%, 11/80) NV compared to type 1 (3.8%, 4/102) and mixed (2.2%, 1/44) NV. The FA classification was not found to be associated with any of the demographic factors examined.
| Anatomic Classification | FA Classification | |
|---|---|---|
| P (Fisher Exact, χ 2 , or Independent Student t Test) a | ||
| Age | .018 b | .301 |
| Sex | .383 | .467 |
| Race | .608 | .922 |
| Family history of AMD | .575 | .628 |
| History of smoking | .077 | .428 |
| History of HTN | .596 | .770 |
| History of DM | .561 | .939 |
| Statin | .618 | .792 |
| Aspirin | .684 | .092 |
| Clopidogrel | .811 | .585 |
| Warfarin | .041 b | .198 |
| Glaucoma | .149 | .786 |
a Fisher exact and χ 2 test were used when comparing categorical variables. Fisher exact test was used if a cell value was less than 5. Independent Student t test was used when comparing categorical variable against continuous variable.
History of smoking was significantly associated with both lesion area and lesion diameter ( Table 3 ). Lesion area was significantly larger for current smokers (13.05 ± 7.38 mm 2 ) than for nonsmokers (6.40 ± 5.81 mm 2 ) or former smokers (5.77 ± 5.16 mm 2 ). Lesion diameter was significantly larger for current smokers (4.40 ± 1.78 mm) than for nonsmokers (3.13 ± 1.44 mm) or former smokers (3.00 ± 1.58 mm).
| Lesion Area | Lesion Diameter | |
|---|---|---|
| P (Univariate) | ||
| Age | .274 | .070 |
| Sex | .679 | .923 |
| Race | .670 | .064 |
| Family history of AMD | .465 | .634 |
| History of smoking | .001 a | .024 a |
| History of HTN | .672 | .583 |
| History of DM | .566 | .905 |
| Statin | .093 | .151 |
| Aspirin | .105 | .113 |
| Clopidogrel | .103 | .094 |
| Warfarin | .176 | .582 |
| Glaucoma | .171 | .090 |
Associations between lesion characteristics (lesion location, lesion area, and lesion diameter) and neovascular lesion subtypes were analyzed with age, history of smoking, and use of warfarin as covariates ( Table 4 ). Compared to type 1 NV, type 2, 3, and mixed NVs were less likely to be foveal in location. This finding was not observed with the FA classification ( Table 4 ). Lesion area and lesion diameter were significantly associated with both anatomic and FA classification. Mixed NV had greater lesion areas and diameters compared to type 1 NV, which in turn had greater lesion areas and diameters than type 2 and 3 NV ( Table 4 ). Similar findings were observed with the FA classification.
| Lesion Location | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Anatomic NV Types | Foveal Location a | Adjusted OR | 95% CI | P | FA CNV Types | Foveal Location a | Adjusted OR | 95% CI | P |
| 1 | 79.2% (84/106) | Reference | Occult | 80.3% (106/132) | Reference | ||||
| 2 | 70.8% (17/24) | 0.180 | 0.039–0.823 | .027 b | Classic | 81.2% (26/32) | 0.173 | 0.021–1.395 | .099 |
| 3 | 79.1% (72/91) | 0.103 | 0.018–0.537 | .007 b | RAP | 77.6% (59/76) | 0.172 | 0.018–1.618 | .124 |
| Mixed | 95.5% (43/45) | 0.184 | 0.039–0.834 | .028 b | Mixed | 96.1% (25/26) | 0.129 | 0.015–1.087 | .129 |
| Lesion Area | |||||
|---|---|---|---|---|---|
| Anatomic NV Types | Mean (mm 2 ) | SE | FA CNV Types | Mean (mm 2 ) | SE |
| P = .022 b | P = .016 b | ||||
| 1 | 7.354 | 1.094 | Occult | 7.525 | 1.011 |
| 2 | 3.805 | 1.454 | Classic | 4.616 | 1.403 |
| 3 | 4.196 | 1.058 | RAP | 4.601 | 1.150 |
| Mixed | 10.106 | 1.337 | Mixed | 9.491 | 1.485 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


