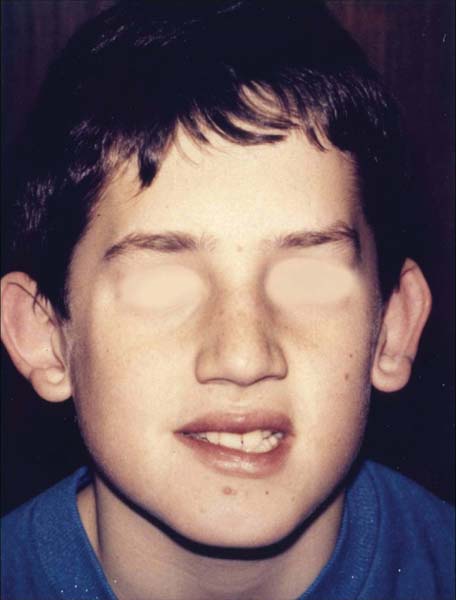
83 A 5-year-old boy has a strong family history of large, protruding ears. Like his family members, he was noted to have prominent ears shortly after birth. His parents had been informed that his ears would ultimately normalize with time. However, increasing projection of his ears has become a center of attention. His parents are now anxious about further teasing, as suffered by other family members at school and the impact on his self-esteem as he grows. Otherwise, he has been a healthy and happy child. His physical examination is unremarkable except for obvious underdevelopment of the antihelical folds of his ears, which contributes the lateral projection of each helix (Fig. 83.1). The auriculocephalic angle measures about 45 degrees bilaterally. Prominent deep conchal bowls are also present. The external ear growth continues into early childhood as the auricle reaches 85% of adult size by 3 years of age. Near-complete development is achieved by 5 or 6 years of age and is considered the appropriate age for repair, especially because this age marks the onset of self-recognition and school matriculation. Specific anatomic landmarks and criteria have been established to help define the normal-appearing external ear (Fig. 83.2). Normal measurements are based on accepted averages for the size and shape of the ear as well as the location and projection of the ear on the head (Table 83.1). Even though prominauris is often obvious, several key features determine the presence or absence of correctable prominent ears. The physical examination is the key diagnostic element in assessment of prominent ears. Fig. 83.1 The patient. Fig. 83.2 Normal auricle and landmarks in an adult. Although most individuals have slight asymmetry from one auricle to the other, cosmetically detectable auricular deformities occur in 3 to 5% of the population. Prominauris, or ear protrusion, is defined by the abnormal projection of the ear from the mastoid cortex. This is the most common ear deformity and is frequently the result of unfurling or incomplete development of the antihelical and superior crural folds. A broad, deep conchal bowl can also contribute to the abnormal appearance of the ear. This is another common auricular deformity that may occur alone or in combination with other abnormalities. Thus surgical correction requires proper recognition of each abnormality of the pinna and concha in persons with atypical ears. Each ear must be examined separately because the deformity may differ from one ear to the other. Specific terms help to describe frequently encountered external ear deformities.
Prominauris and Otoplasty
History
Differential Diagnosis—Key Points

Vertical length | 55–60 mm |
Width | 5% of height (30–35 mm) |
Vertical axis | Angled 20% posteriorly |
Auriculomastoid angle | 20–35 degrees |
Location | |
Superior pinna | Level with lateral brow |
External auditory canal | Level with inferior orbital rim |
Helical-mastoid distances | |
Superior rim | 18–20 mm |
Middle (external canal) | 14–16 mm |
Inferior (cauda helix) | 10–12 mm |
 The protruding ear has a normal shape and size but with unfurling of the superior crus and antihelix giving lateral protrusion. Present at birth, these abnormalities become more conspicuous with increasing age.
The protruding ear has a normal shape and size but with unfurling of the superior crus and antihelix giving lateral protrusion. Present at birth, these abnormalities become more conspicuous with increasing age.
 The lop ear is an abnormal ear with helical cartilage that is soft and lacks strength to maintain its structure. The ear subsequently hangs limp, causing it to fold at the upper pole and resemble the appearance of a rabbit’s floppy ear. Faulty development of the helix, scapha, and antihelix are attributed to this deformity. Sometimes the ear will appear smaller than normal.
The lop ear is an abnormal ear with helical cartilage that is soft and lacks strength to maintain its structure. The ear subsequently hangs limp, causing it to fold at the upper pole and resemble the appearance of a rabbit’s floppy ear. Faulty development of the helix, scapha, and antihelix are attributed to this deformity. Sometimes the ear will appear smaller than normal.
 The cup ear consists of both the lop and the protruding
The cup ear consists of both the lop and the protruding
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


