Chapter 48 Proliferative Diabetic Retinopathy
The earliest diabetes-induced changes in the retina are biochemical, hemodynamic, and cellular in nature. Often these are initially imperceptible clinically and may have no or minimal effect on vision. In contrast, proliferative diabetic retinopathy (PDR) represents an advanced stage of diabetic eye disease characterized by the growth of newly formed retinal vessels on the retina or optic disc that extend along the retinal surface or into the vitreous cavity, significantly increasing the risk for vision loss.1,2 Among patients with diabetes, nearly 25% with type 1 and 16% with type 2 will develop PDR after 15 years of diabetes.3,4 The rate of progression to PDR is highest among type 1 patients, with a 42% cumulative risk over 25 years.5 Furthermore, there is a strong association between PDR and uncontrolled systemic disease.6,7 The publication of landmark clinical trials establishing the importance of intensive glycemic control in preventing the onset and progression of retinopathy and other diabetic complications in both type 1 and type 2 diabetes has led to marked improvement in the medical care of patients with diabetes over the past two decades. With these improvements there has been a corresponding decline in the incidence of PDR.8–11 Nevertheless, the ocular complications arising from development of PDR remain a leading cause of severe vision loss in developed countries worldwide.10
Pathogenesis of proliferative diabetic retinopathy
Hyperglycemia and metabolic changes from diabetes lead to alterations in the retinal vasculature that result in reduced perfusion of the retinal tissue.12 This state of relative retinal ischemia is thought to be the primary angiogenic stimulus that plays a central role in the pathogenesis of PDR. Various angiogenic factors such as angiopoietin, erythropoietin, basic fibroblast growth factor (bFGF), insulin-like growth factor (IGF), protein kinase C (PKC), tumor growth factor (TGF), and platelet-derived growth factor (PDGF) have stimulatory or modulating activities during the development of PDR. However, based on in vivo and in vitro studies, the protein called vascular endothelial growth factor (VEGF) appears to be primarily responsible for the ischemia-driven angiogenic pathology in PDR.13–15 The role of VEGF in PDR is well supported by studies demonstrating high concentrations of VEGF in the vitreous of patients with PDR which are closely correlated with extent of disease activity.13,16 Following successful laser treatment and in patients with naturally quiescent PDR, VEGF vitreous concentrations were low or undetectable.13 Furthermore, the direct role for VEGF mediation of the neovascular response in PDR was demonstrated by showing that vitreous fluids from patients with active PDR were angiogenic in vitro, and this angiogenic stimulus could be blocked using a VEGF-specific inhibitor. Intraocular vessels from PDR and diabetes-induced iris neovascularization are exquisitely sensitive to VEGF inhibitors, often showing initial regression within one day.17
Although VEGF appears to be the primary direct causative angiogenic factor in PDR, the complex mechanisms regulating in vivo angiogenesis likely involve factors other than VEGF as well. Angiogenic pathways such as the angiopoietin/Tie-2 system modulate the effect of VEGF and directly affect retinal pericytes and endothelial cells, which are the principal cell types thought to be involved in the pathological processes of PDR.18,19 In addition, hyperglycemia reduces PDGF survival-promoting activity, thus leading to pericyte apoptosis and diabetic vasculopathy. This mechanism is driven by hyperglycemia-induced activation of protein kinase C-δ (PKC-δ) which leads to increased expression of a protein tyrosine phosphatase called Src homology-2 domain–containing phosphatase-1 (SHP-1). SHP-1 activation in turn mediates resistance to PDGF, resulting in loss of cellular survival mechanisms and increased pericyte apoptosis.20 Inhibition of SHP-1 is being investigated as a possible protective mechanism against initial retinal changes that underlie subsequent development of PDR.20 VEGF independent pathways such as that mediated by erythropoietin (EPO) have also been implicated in the development of PDR.21 Single nucleotide polymorphisms (SNPs) that increase EPO expression have been associated with development of PDR and severe renal disease in a small genetic study of three independent patient populations.22,23 Antiangiogenic mediators such as pigment epithelium-derived factor (PEDF) are reportedly lower in patients with diabetes and in patients with active PDR compared to other retinopathies.24 An interplay between both angiogenic and antiangiogenic pathways may be important in the eye at various stages of retinopathy.25 A more detailed discussion regarding the pathological angiogenesis of PDR is presented in Chapter 26.
Origin and early recognition of preretinal new vessels
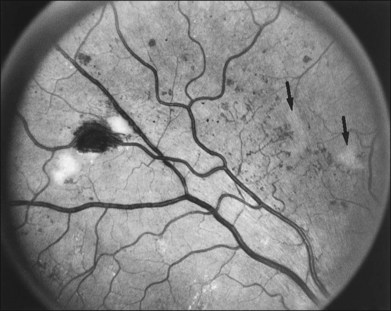
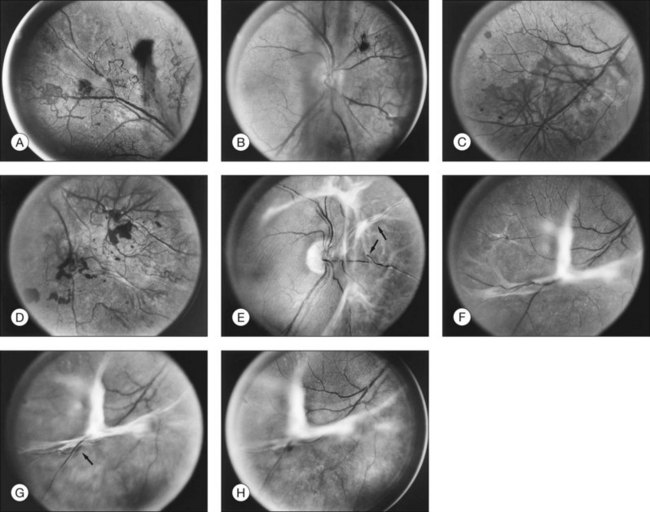
The risk of PDR is greatest in eyes with severe nonproliferative diabetic retinopathy (NPDR), characterized by the presence and severity of soft exudates (cotton-wool spots), intraretinal microvascular abnormalities (IRMA, a term chosen so as to be neutral about whether these abnormal vessels represent intraretinal new vessels or dilated pre-existing vessels), venous beading, and extensive retinal hemorrhages or microaneurysms (H/MA) (Fig. 48.1). In the Diabetic Retinopathy Study (DRS), severe NPDR was defined as the presence of at least three of the above four characteristics, each generally involving at least two quadrants of the fundus. Approximately 50% of such eyes assigned to the untreated control group developed PDR within 15 months.26 Today, a quick assessment of severe or very severe NPDR can be derived from determining the extent and severity of H/MA (moderately severe in 4 quadrants), VB (definitely present in 2 or more quadrants), and IRMA (obvious in 1 or more quadrant) – the 4–2–1 rule (see Box 48.1). Any one of these findings indicates severe NPDR and two or more represent very severe NPDR. As noted above, these levels of NPDR are associated with a high likelihood of developing PDR.
The lesions characterizing severe NPDR are related to retinal capillary closure, and their frequent presence in eyes that are about to develop preretinal new vessels is one important observation linking these processes. Further evidence has been provided by the fluorescein angiographic montages of Shimizu and coworkers,27 who found that the extent of capillary closure observed using angiography increased as the severity of new vessels increased on the following four-step scale: (1) none, (2) new vessels involving the retina but sparing the disc, (3) new vessels involving the disc, and (4) neovascularization of the anterior chamber angle with neovascular glaucoma. Muraoka and Shimizu28 have provided serial fluorescein angiographic observations supporting the view that some lesions designated as IRMA or reduplication of small venules are in fact intraretinal new vessels revascularizing areas of capillary loss.
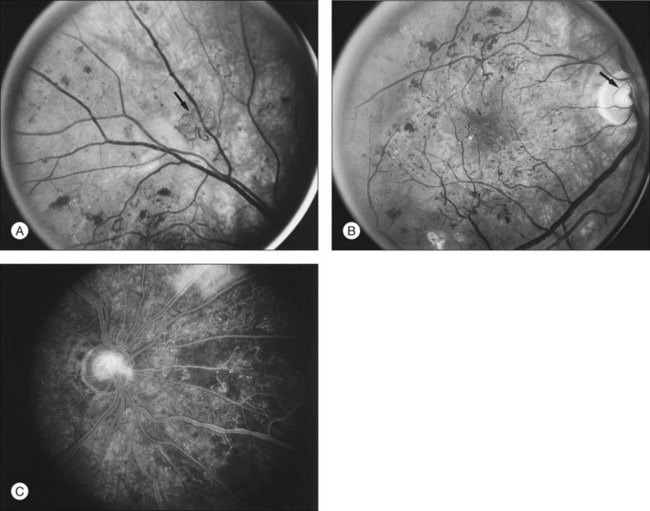
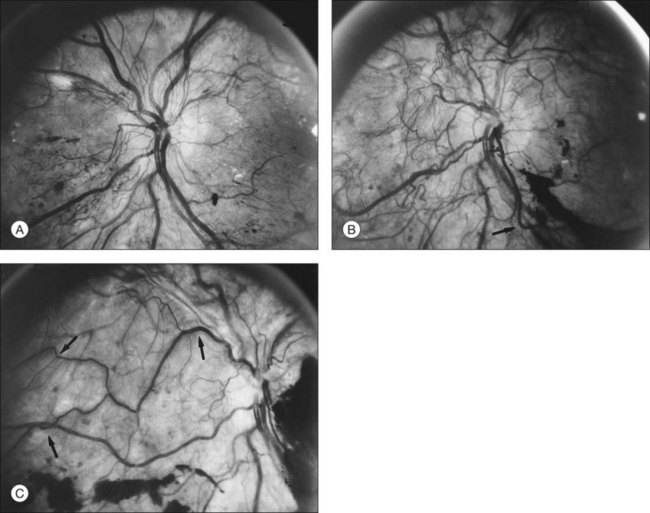
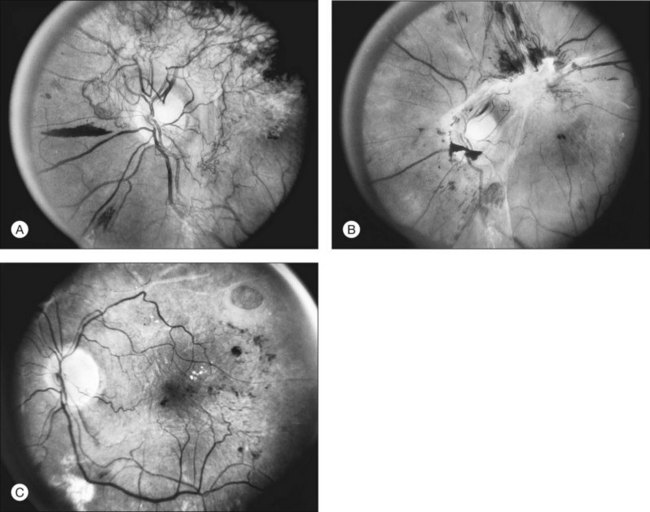
Although there is little doubt that the presence of severe NPDR is predictive of subsequent neovascularization, the characteristic intraretinal lesions are not always present when preretinal new vessels are first recognized. A possible explanation for this absence is the relatively transient nature of some of these lesions. Soft exudates usually disappear within 6–12 months.29 H/MA have a half-life of approximately 3 months.30 Blot hemorrhages and IRMA tend to disappear after extensive capillary closure, when the number of small vascular branches decreases and some small arterioles become sclerosed with a white thread-like appearance. This condition is sometimes described as “featureless retina” (Fig. 48.2B). However, in some eyes intraretinal lesions are mild, and signs of extensive capillary closure are absent when new vessels are first recognized.
New vessels may arise anywhere in the retina; however, they are most frequently seen posteriorly, within about 45 degrees of the optic disc. They are particularly common on the disc itself (Davis reported 69% of 155 eyes with PDR31; Taylor and Dobree, 73% of 86 eyes32). In the DRS, among 1377 control-group eyes with new vessels present in baseline photographs 15% had new vessels only on or within 1 disc diameter (DD) of the disc or in the vitreous cavity anterior to this area (new vessels on disc, or NVD), 40% had new vessels only outside this zone (new vessels elsewhere, or NVEs), and 45% had new vessels in both zones.33 Also from the DRS, NVE had been shown to occur most frequently in the superotemporal quadrant (field 4, 27%), followed in frequency by the inferonasal (field 7, 21%) quadrant.34 Although rare, the appearance of neovascularization arising from the perifoveal capillaries has been reported,35 and possibly may provide insight on the association of DR and perifoveal telangiectasia.36
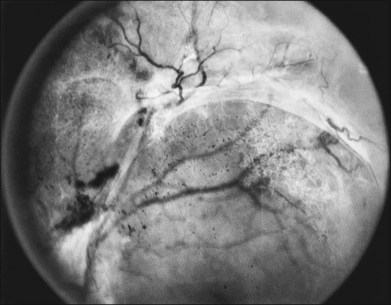
NVD (defined as NV at or within 1 disc diameter of the diskc37) begins as fine loops or networks of vessels lying on the surface of the disc or bridging across the physiologic cup. They are usually easily identified once established, but in their earliest stages they may be overlooked, especially with the low magnification of binocular indirect ophthalmoscopy. They also may be difficult to distinguish from normal vessels in nonstereoscopic photographs or with monocular direct ophthalmoscopy. The most satisfactory examination methods are those that provide a magnified stereoscopic view, either biomicroscopy with contact or precorneal lens or stereoscopic 30-degree photography. If necessary, new vessels can be identified using fluorescein angiography where they will leak profusely, unlike normal physiologic vasculature (Fig. 48.2).
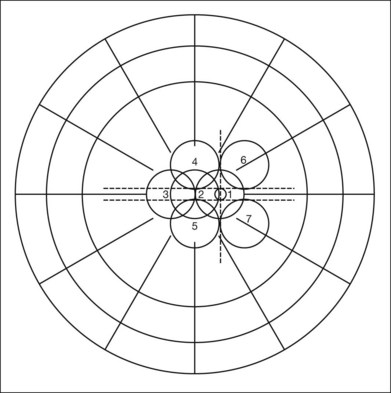
Evaluation of early NVE requires identification of the lesion and differentiation from IRMA. Binocular indirect ophthalmoscopy of the retina combined with a biomicroscopic or direct ophthalmoscopic examination of any suspicious lesions and careful review within 5 or 6 DD of the disc is a useful approach. Indirect ophthalmoscopy alone is not adequate. When new vessels or fibrous proliferation are extensive, wide-angle (45-degree or, preferably, 60-degree) photographs have the advantage of providing in one or two fields an integrated view of all or most of these lesions. For detection of early NVE, stereophotographs with a 30-degree camera are superior, and in most patients an adequate stereoscopic effect can be obtained in all the seven standard fields of the modified Airlie House classification33,37 (Fig. 48.3), even with a maximum pupillary dilation of only 4 or 5 mm. The fundus should be scanned for definite or questionable NVE outside the standard fields, particularly between and above fields 4 and 6, between and below fields 5 and 7, and temporal to fields 4 and 5. Subsequent follow-up visits are greatly facilitated by a set of 30-degree stereophotographs from the baseline examination.
Ultrawide field imaging is a newer modality allowing visualization of retinal areas previously difficult or impossible to image. A single 200-degree field taken with ultrawide field scanning laser ophthalmoscopes resulted in detection of lesions that were beyond the field of routine standard 30- and 45-degree photography.38 This capability of ultrawide field retinal imaging may enhance the detection of areas of peripheral vessel leakage and non-perfusion by flourescein angiography.39 Potentially, when validated in a broader patient population, imaging of the retinal periphery may provide prognostic and early risk stratification for visual loss in patients with diabetic retinopathy.
Natural course of proliferative diabetic retinopathy
Development and proliferation of new vessels
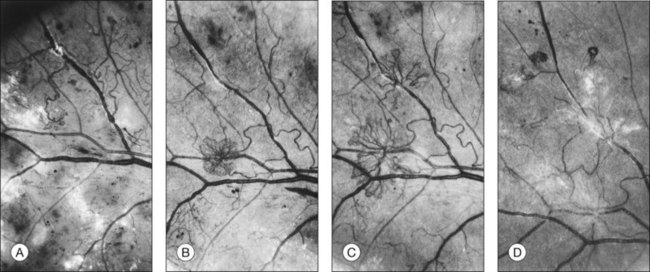
Initially, new vessels may be barely visible. Later, their caliber is commonly one-eighth to one-quarter that of a major retinal vein at the disc margin, and occasionally they are as large as such veins (Fig. 48.4). New vessels frequently form networks that often resemble part or all of a carriage wheel. The vessels radiate like spokes from the center of the complex to a circumferential vessel bounding its periphery (see Figs 48.2A and 48.4). New vessel networks may also be irregular in shape, without a distinct radial pattern. New vessel patches often lie over retinal veins and appear to drain into them. The superotemporal vein is involved somewhat more frequently than others.31,32 In the 1158 DRS control-group eyes that had NVE in at least one of the five photographic fields in which they were graded (fields 3 to 7 in Fig. 48.3), the number of times each field was involved was assessed. In each eye a count of one was divided equally among all fields containing NVE, and the counts for each field were totaled for all eyes. Field 4, which usually includes a major portion of the superotemporal vein, had a score of 308 (27% of 1158), whereas other scores ranged from 194 (17%) for field 5 to 242 (21%) for field 7.2
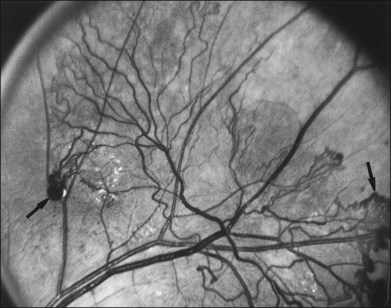
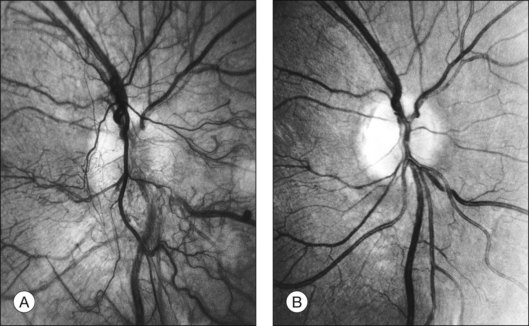
At times new vessels grow for several DD across the retina without forming prominent networks. The new vessels appear much like normal retinal vessels but are easily recognized as new vessels because of their unique capability of crossing both arterioles and veins in the underlying retina (Figs 48.5. 48.6). New vessels of this type commonly arise on the disc and are often accompanied during their actively growing phase by mild-to-moderate thickening (presumably edema) of the disc and surrounding retina (Fig. 48.7). This appearance is similar to typical cases of diabetic papillopathy,40 in which all or most of the dilated small vessels on and adjacent to the disc are intraretinal and characteristically do not leak on fluorescein angiography.
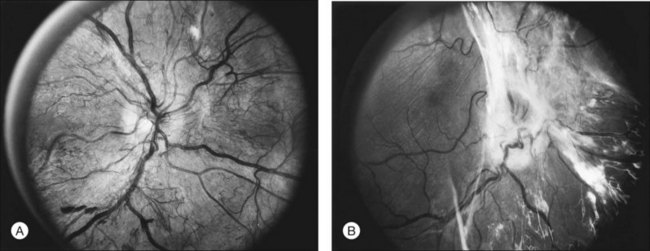
The growth rate of new vessels is extremely variable. In some patients a patch of vessels may show little change over many months, whereas in others a definite increase may be seen in 1–2 weeks. Early in their evolution new vessels appear bare, but later, delicate white fibrous tissue usually becomes visible adjacent to them. The common clinical convention of referring to such tissue as “fibrous” is adhered to in this chapter, even though it has been shown to contain both fibrocytes and glial cells.41,42 New vessels characteristically follow a cycle of proliferation followed by partial or complete regression.31,43 Regression of a wheel-shaped net of new vessels typically begins with a decrease in the number and caliber of the vessels at the center of the patch, followed by their partial replacement with fibrous tissue. Simultaneously, the peripheral vessels tend to become more narrow, although they may still be growing in length and the patch may still be enlarging (Fig. 48.4). At times, regressing new vessels appear to become sheathed. The width of the sheath, which presumably represents opacification and thickening of the vessel wall, increases until only a network of white lines without visible blood columns remains (Fig. 48.8). At times certain new vessels seem to become preferential channels, enlarging while adjacent vessels regress and disappear. Fresh, active new vessels are commonly seen emerging from the edges of partially regressed patches, and new vessels are frequently seen at different stages of development in different areas of the same eye. Early in their evolution, the fibrous components of fibrovascular proliferations tend to be translucent and are easily underestimated. Subsequently, with increasing growth, contraction, or separation from the retina, they become more prominent. If contraction of the vitreous and fibrovascular proliferations does not occur, new vessels may pass through all the stages described here without causing any visual symptoms. Concurrently, a decrease in intraretinal lesions and in the caliber of major retinal vessels may occur as retinopathy enters the quiescent stage. Occasionally, new vessels appear to regress completely, leaving no trace of their previous presence.44
Based on the findings of the DRS, the development of PDR with high-risk characteristics places the patient at an increased risk for visual loss and generally requires prompt laser treatment. PDR with high-risk characteristics is defined by one or more of the following lesions: (1) NVD that is approximately one-quarter to one-third disc area or more in size (i.e., greater than or equal to NVD in standard photograph 10A); (2) any amount of NVD if fresh vitreous or preretinal hemorrhage is present; or (3) NVE greater than or equal to one-half disc area in size if fresh vitreous or preretinal hemorrhage is present Therefore, attention must be paid to the presence, location, and severity of new vessels, as well as the presence or absence of preretinal or vitreous hemorrhages.2
Contraction of the vitreous and fibrovascular proliferation
Before the beginning of posterior vitreous detachment, new vessels are usually asymptomatic.31,43 Small hemorrhages in the posterior vitreous are occasionally seen near the growing ends of the new vessels, but they usually remain subhyaloid or hang suspended in the most posterior portion of the vitreous without becoming apparent to the patient. When symptomatic vitreous hemorrhages occur, some evidence of localized posterior vitreous detachment can usually be found. When only a small area of the posterior vitreous surface is detached, it appears flat and very close to the retina, but as detachment becomes more extensive, this surface moves forward and assumes a curved contour more or less parallel to the retina and about 0.5–2 DD anterior to it. This otherwise smoothly curved surface is held posteriorly by vitreoretinal adhesions at the sites of new vessels. The new vessels in turn tend to be pulled forward in these same areas. Vitreous strands and opacities can usually be seen anterior to the posterior vitreous surface, whereas posteriorly the vitreous cavity is optically empty or contains red blood cells.31,45 The principal force pulling the posterior vitreous surface forward usually appears to be the forward vector resulting from contraction of this surface and the fibrovascular proliferation growing along it. In explaining this process to students and patients, it helps to use the analogy of a bowl lined with a piece of cloth attached to the rim of the bowl: if the cloth shrinks, it eventually becomes tightly stretched across the top of the bowl.
The thickness of the posterior vitreous surface varies, as indicated by three different appearances. Immediately adjacent to the site of new vessels, the surface is often thick enough to be seen easily with the ophthalmoscope. Presumably this increased opacity is due to proliferation of fibrous tissue along the posterior vitreous surface. In other areas some distance from any visible new vessels, the surface is also sometimes thick enough to be detected ophthalmoscopically or in stereoscopic fundus photographs. In these areas the surface is usually somewhat shiny, with thinner and thicker areas alternating to give a “Swiss cheese” effect but without actual holes; presumably a thin layer of fibrous tissue is also present here. In still other areas the posterior vitreous surface is so thin that it can be appreciated only by mentally integrating many separate slit-lamp sections. Only the portion directly illuminated by the slit beam is visible, and the impression of a continuous surface is gained by watching the slit beam glide along smoothly over the surface as the slit lamp is moved. Frequently in the same eye all these various appearances can be seen in different areas of the same surface, the general course of the surface continuing without change as its thickness varies (Fig. 48.9).
Posterior vitreous detachment usually begins near the posterior pole, the most common locations being the region of the superotemporal vessels, temporal to the macula, and above or below the disc.31 Detachment often spreads fairly rapidly (within hours, days, or weeks) to the periphery of the quadrant in which it begins, unless such spread is impeded by vitreoretinal adhesions associated with patches of new vessels. Extension circumferentially into other quadrants of the fundus tends to be slower, sometimes requiring months or years to reach completion. Detachment of the vitreous from the disc is usually prevented by adhesions between the vitreous and fibrovascular proliferations arising there. Vitreous detachment is not a smoothly progressive process. It occurs in abrupt steps, usually halting whenever its advancing edge meets a patch of active or regressed new vessels. If contraction continues, the patch is pulled forward, with or without the underlying retina, and vitreous detachment spreads beyond it. At times the peripheral spread of posterior vitreous detachment is halted temporarily by invisible adhesions to the retina in areas where no new vessels are present. These adhesions are indicated by a subtle linear elevation of the inner surface of the retina at the junction of posteriorly detached and anteriorly attached vitreous. After several weeks or months, vitreous detachment usually spreads farther peripherally, and the subtle retinal fold flattens.
Traction exerted on the new vessels appears to be a factor contributing to the recurrent vitreous hemorrhages that often coincide with extension of vitreous detachment. Hemorrhages also occur independently, sometimes apparently in relation to bouts of severe coughing or vomiting and occasionally at the time of insulin reactions. More often they occur during sleep and are unrelated to any obvious factor.46,47 Blood in the fluid vitreous posterior to the detached vitreous framework usually absorbs within weeks or several months, retaining its red color until absorbed. Hemorrhage in the formed vitreous tends to lose its red color and become white before absorption is complete. Absorption of a large hemorrhage from the formed vitreous is usually slow, requiring many months.
The arrangement and movement of blood in the posterior fluid vitreous often make it possible to define the limits of posterior vitreous detachment ophthalmoscopically.31,48 In areas of vitreous detachment, the presence of fresh blood in the posterior fluid vitreous obscures fundus details, distinguishing these areas from adjacent areas in which the vitreous remains attached and details of the retina are clear. In the upper quadrants of the fundus, blood tends to become deposited in thin meridional streaks on the detached posterior vitreous surface, identifying its position. Inferiorly, blood pools between the detached vitreous and attached retina, outlining the inferior extent of vitreous detachment and often forming a fluid-level or “boat-shaped” hemorrhage. At times, even when posterior vitreous detachment cannot definitely be identified with slit lamp and contact lens, a thin, curving line of subhyaloid hemorrhage parallel to and behind the inferior equator can be seen, presumably marking the lower edge of an area of vitreous detachment. Occasionally the posterior vitreous surface can be traced across the macula on slit-lamp examination, but usually its continuity is lost in this region. In some of these cases a round or oval hole with sharp edges can be detected in the posterior vitreous surface, occupying an area 2–4 DD wide in the posterior pole. The posterior vitreous surface in this area appears broken, with solid vitreous protruding back through the hole and coming into contact with the retina. At times the surface of a bulging mushroom of vitreous can be seen extending posteriorly through such a hole, occasionally with hemorrhage suspended within its lower part (Fig. 48.10).
Retinal distortion and tractional detachment
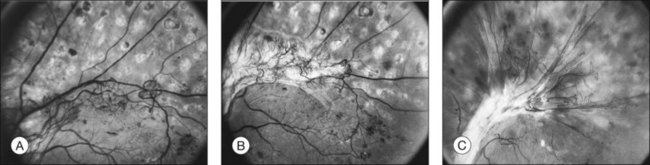
With contraction of an extensive sheet of fibrovascular proliferations, distortion or displacement (“dragging”) of the macula may occur.49 In some cases the central, more intensely pigmented area of the retinal pigment epithelium (RPE) appears to be dragged with the neurosensory macula toward the major focus of contracted tissue, whereas in other cases only the neurosensory macula appears displaced. Since the most common site of extensive fibrovascular proliferations is on and near the disc, the macula is usually dragged nasally and often also somewhat vertically (Figs 48.11, 48.12).
Contraction of vitreous or areas of fibrovascular proliferation may also lead to retinal detachment. This retinal detachment may be limited to avulsion of a retinal vessel, usually a vein, sometimes accompanied by vitreous hemorrhage. Alternatively, a relatively thin fold of retina may become elevated, with only a narrow zone of retinal detachment adjacent to its base, sometimes outlined by a pigmented demarcation line. In other cases retinal detachment may be more extensive, but the concave shape that is typical of traction detachment is generally maintained. At times, small, apparently full-thickness retinal holes may be seen near the proliferation; these sometimes, but not always, lead to rhegmatogenous detachment. When such detachment does occur, it tends to have a flat or convex anterior surface and be more extensive, often reaching the ora serrata. The occurrence and severity of retinal detachment are influenced by the timing and degree of shrinkage of the vitreous and fibrovascular proliferations and by the type, extent, and location of the new vessels responsible for vitreoretinal adhesions. Extensive nets of large-caliber new vessels accompanied by heavy fibrous tissue produce broad, tight vitreoretinal adhesions. Contraction of such proliferations is often followed by extensive retinal detachment (Fig. 48.12). New vessels with little accompanying fibrous tissue tend to produce less extensive vitreoretinal adhesions and less risk of retinal detachment, particularly when posterior vitreous detachment begins soon after the onset of neovascularization (Fig. 48.13). At times, new vessels that extend for a considerable distance along the surface of the retina appear to be adherent to the retina only at their sites of origin and to the vitreous only near their distal ends. In this case, the posterior vitreous surface can pull away from the retina by a distance equal to the length of the vessels before exerting traction on the retina. When new vessels are confined to the surface of the disc, vitreous detachment can reach completion without producing traction on the retina, since there are no vitreoretinal adhesions. Retinal detachment does not occur in such eyes, but recurrent vitreous hemorrhage from the new vessels is common.
Involutional or “Quiescent” Proliferative Diabetic Retinopathy
DR ultimately reaches an involutional stage wherein the retinopathy has “burned-out” and is termed “quiescent.” At this stage vitreous contraction has reached completion and the vitreous is detached from all areas of the retina except where vitreoretinal adhesions associated with new vessels prevent such detachment.31,43,50,51 Vitreous hemorrhages decrease in frequency and severity and may stop entirely, although many months may elapse before substantial vitreous clearing occurs. Some degree of retinal detachment may be present at this stage. If the detachment is localized and the macula remains intact, visual acuity may be good. However, dragging or distortion of the macula or long-standing macular edema can lead to substantial reduction in vision. In some cases, retinal detachment involves the entire posterior pole, with resultant severe loss of vision. Although spontaneous partial reattachment occasionally occurs, if the macula has been detached for months or years, usually little significant return of vision occurs.
Relationship of proliferative diabetic retinopathy to type and duration of diabetes
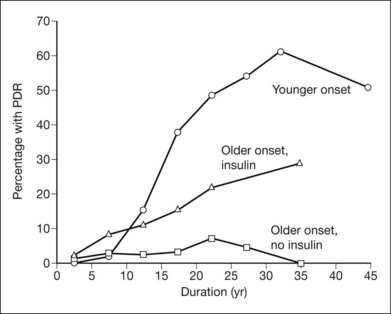
In a population-based stereophotographic study carried out by Klein and coworkers,52 the prevalence of PDR in insulin-taking patients younger than 30 at diagnosis (exclusively or mainly type 1) was near zero when duration of diabetes was less than 10 years and then rose rapidly to about 50% in persons with 20 years or more of diabetes. In an older-onset (30 years or more) insulin-taking group, which included both diabetes types, prevalence of PDR rose fairly steadily, from 2% in persons with less than 5 years of diabetes to about 25% in those with 20 years or more. In the older-onset, noninsulin-taking (type 2) group, prevalence of PDR increased only slightly with duration, from less than 5% before 20 years to about 5% thereafter (Fig. 48.14).53 Among patients with PDR, its severity did not appear to differ between the younger-onset and the combined older-onset groups. In each case, in the worse eye about 25% of patients had DRS high-risk characteristics and 15% had retinopathy severity ungradable because of extensive vitreous hemorrhage, phthisis bulbi, or enucleation secondary to complications of DR.7 In patients with PDR, macular edema was more common in the combined older-onset group with retinal thickening or scars of previous focal photocoagulation present in at least one eye in about 45% (versus 30% in the younger-onset group).54
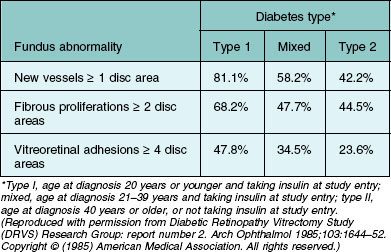
The Diabetic Retinopathy Vitrectomy Study (DRVS) found a substantial variation in severity of PDR by diabetes type among persons with vitreous hemorrhage severe enough to reduce visual acuity to 5/200 or less for a period of at least 1 month.55–58 In this study the severity of new vessels, fibrous proliferation, and vitreoretinal adhesions decreased significantly as diabetes type shifted from type 1 to type 2 (Table 48.1).
Table 48.1 Percentage of Diabetic Retinopathy Vitrectomy Study (DRVS) group H eyes assigned to early vitrectomy with specified severity level of new vessels, fibrous proliferations, and vitreoretinal adhesions, by diabetes type
Diabetes with onset after age 30 is more common than the younger-onset type, and in clinical practice PDR is seen with about equal frequency in the younger- and older-onset groups. Klein et al.52,53 estimated that in the population they surveyed, 43% of patients with PDR were in the younger-onset group, 42% were in the older-onset insulin-taking group, and 15% were in the noninsulin-taking group. In the DRS, in which more than 90% of the 1742 patients examined had PDR in at least one eye, 44% were classified as juvenile-onset (younger than 20 years at diagnosis and taking insulin at entry into the study); 28% as adult-onset, possibly insulin-dependent (age 20 years or older at diagnosis, not overweight, and taking insulin); and 26% as classic adult-onset (mild symptomatic or asymptomatic onset at age 20 years or older and either overweight or not taking insulin at study entry). The remaining 2% were not classifiable.33 Aiello and coworkers59 described the distribution of age at diabetes diagnosis among 244 patients with PDR at the Joslin Clinic during a 5-month period: diagnosis age less than 20 years, 53%; 20–39 years, 25%; and 40 years or older, 22%.
In a comprehensive meta-analysis including 28 prospective interventional or observational studies comprising 27 120 diabetic patients with at least 10 years of follow-up, lower rates of progression to PDR and severe visual loss were observed in those more recently diagnosed with diabetes.10 The 4-year risk of progression to PDR and severe visual loss was substantially lower among participants in 1986–2008 (2.6% and 3.2%) than in 1975–1985 (19.5% and 9.7%). At 10 years, similar patterns were observed with participants in 1986–2008 studies having lower proportions of PDR and NPDR at all time points than participants in 1975–1985 studies. National population-based estimates have reflected this trend of a reduction in the prevalence of PDR, presumably reflecting improved glycemic and systemic control as well as earlier detection of retinal complications.60 These trends in the reduction of PDR and visual loss are discussed in greater detail in Chapter 45 (The epidemiology of diabetic retinopathy).
Proliferative diabetic retinopathy and blood glucose control
The results from the Diabetes Control and Complications Trial (DCCT)/Epidemiology of Diabetes Interventions and Complications (EDIC) and the United Kingdom Prospective Diabetes Study (UKPDS) have established the benefit of intensive blood glucose control in reducing the risk for DR in both type 1 and type 2 patients.61–70 These large multicenter trials demonstrated conclusively that the long-term risks for the development and progression of DR can be reduced dramatically by improving blood glucose control with intensive treatment.61–70
Additional evidence that better glycemic control in patients with severe NPDR or early PDR reduces their risk of further progression is provided by Early Treatment Diabetic Retinopathy Study (ETDRS) multivariable analyses of risk factors for progression to high-risk PDR. HbA1c at baseline was a strong risk factor. Patients with HbA1c >12% had the highest risk of progression and patients with HbA1c <8.3% had the lowest risk of progression (OR 1.59 vs 1.00, P <0.0001).71 Even in the lowest A1c category, the 5-year rate of developing high-risk PDR from severe NPDR was high (50%). These data suggest that the benefits of better control continue to be manifest even once severe NPDR or PDR has developed; however, they do address the effects, beneficial or harmful (see below), of improving control at this stage.
Early worsening of retinopathy with improved glycemic control
Soon after HbA1c assays, home blood glucose monitoring and continuous subcutaneous insulin infusion became widely available, several small clinical trials and case series reported the frequent occurrence of unexpected worsening of DR72–75 in the first 3–12 months following the initiation of intensive insulin therapy (termed “early worsening”).73,76–78 In most of these early trials the patients enrolled had no more than mild-to-moderate NPDR at baseline and the early worsening, when it occurred, was usually mild (development of cotton-wool spots and/or IRMA) and transient. In some reports, however, when glycemic control was very poor and/or retinopathy more severe at baseline, some eyes developed severe PDR and/or macular edema and substantial visual loss.63,72–75
In the DCCT, cotton-wool spots or IRMA, or both, developed in only 1% of 348 patients entering the trial with no retinopathy. This proportion increased to 48% in the 60 patients with mild nonproliferative retinopathy, defined as the presence of microaneurysms plus mild retinal hemorrhages and/or hard exudates. Recovery was frequent and at the 4-year follow-up visit progression from baseline on the ETDRS scale was about the same in intensive treatment group eyes that had experienced early worsening as in conventional treatment group eyes that had not (1.3 vs 1.0 steps). Clinically important early worsening (defined as development of PDR, severe NPDR, or clinically significant macular edema) was not observed in patients with no retinopathy or with microaneurysms involving only one eye, but it occurred in 6 of the 32 patients with moderate NPDR. DCCT patients were followed closely, and early worsening did not lead to serious visual loss, but DCCT findings support the conclusion that early worsening may be more common and more sight-threatening in patients with more severe retinopathy and/or very poor glycemic control. For this reason, patients with advanced nonproliferative or active proliferative DR should be monitored closely before and for several months after initiation of intensive insulin treatment.70,72,75,79 Panretinal photocoagulation prior to initiation of such treatment may be considered when factors suggest a particular need to protect against advancing severe retinopathy. Such considerations include very severe NPDR or active PDR, long-standing very poor glycemic control and high likelihood of suboptimal follow-up.72 The most important risk factors for early worsening were higher baseline HbA1c and greater reduction of HbA1c after enrollment. Possible mechanisms include72,75 alterations in retinal blood flow, decreased autoregulation of the retinal circulation, transient ischemia owing to a decrease in nutrient substrate, and insulin-induced changes in retinal homeostasis that lead to an increase in growth factors such as VEGF.80–82 Because the short- and long-term benefits of improved glycemic control in reducing the risk of retinopathy progression are remarkable67 and because treatments for sight-threatening retinopathy are highly effective in preventing visual loss, intensive glycemic control should not be discouraged for fear of retinopathy progression.69
Absence of proliferative diabetic retinopathy in individuals with diabetes of extreme duration
Despite the nearly universal development of some degree of retinopathy in people with diabetes given sufficient time, the development of PDR plateaus at approximately 60%. This observation has generated significant research interest, as it suggests that there may be protective mechanisms that may delay or prevent the progression to PDR. There are published reports on two unique cohorts of type 1 patients with more than 50 years of type 1 diabetes. The Golden Years cohort from the United Kingdom was noted to have characteristic normal body mass, low insulin dose, a favorable lipid profile, and a positive family history of longevity consistent with possibly genetically determined favorable outcomes.83 The Joslin 50-year Medalist cohort has been characterized for all four major diabetic vascular complications of retinopathy, nephropathy, neuropathy, and cardiovascular disease. The 50-Year Medalist Study84,85 has demonstrated that substantial proportions of individuals may survive diabetes duration of 50 years or more and remain free of advanced diabetic vasculopathy including PDR (49.4%). Longitudinal data from a subgroup of 97 Medalists followed for an average of 20.6 years and 39.4 visits suggests that retinopathy worsening occurs almost entirely within the first two decades of follow-up and eyes that do not develop PDR have a slower rate of retinopathy progression. These findings strongly suggest the existence of a subgroup of individuals who develop early protection against the long-term adverse effects of hyperglycemia. Furthermore, despite multiple studies that have strongly associated worse glycemic control, hypertension, and hyperlipidemia with more severe diabetic retinopathy or diabetic macular edema in patients with shorter duration diabetes, no relationship has been found between these factors and PDR status in the Medalists. Instead, initial findings suggest that specific combinations of advanced glycation endproducts may be associated with increased risk for (carboxyethyl-lysine and pentosidine) or protection from (carboxymethyl-lysine and fructose-lysine) PDR in this unique cohort. Ongoing studies in the Medalists and other populations with extremely long duration of diabetes may yield additional insights into protective mechanisms against PDR development, including novel genetic, biochemical, and physiologic factors.
Systemic medications and proliferative diabetic retinopathy
Systemic medications are often used in the setting of diabetes mellitus to attain optimal glycemic control and treat coexisting conditions. These drugs can have beneficial or deleterious effects on the onset or progression of diabetic eye disease. There is mounting evidence that oral systemic medications can reduce microvascular complications possibly though mechanisms other than their effect on glycemic control, blood pressure and lipid lowering. The results of clinical trials on glycemic control (DCCT,61,65 EDIC,69,70 UKPDS,62,67,68 ACCORD,86 ADVANCE87), lipid-lowering medications (ACCORD-EYE,88 FIELD89) and angiotensin-converting enzyme inhibitors (EURODIAB,90 EUCLID,90 ADVANCE86) angiotensin II type 1-receptor blockers (DIRECT91,92, RASS93) on retinopathy progression are discussed in detail in Chapter 45 (The epidemiology of diabetic retinopathy) and Chapter 47 (Nonproliferative diabetic retinopathy and diabetic macular edema).
Evidence to support the rationale of using systemically active therapeutic agents to prevent or limit local microvascular complications such as PDR is also growing. Thiazolidinediones are a class of oral hypoglycemic agents used in the treatment of type 2 diabetes that activate the peroxisome proliferator-activated receptor (PPAR) γ – a transcription factor known to regulate the expression of genes primarily located in adipose tissue, but also present in other tissues such as the retina.94 The thiazolidinedione rosiglitazone has been reported to delay the onset of PDR, possibly because of antiangiogenic effects mediated by PPARγ agonist activity.95,96 Shen and colleagues95 performed a longitudinal medical record review of 124 patients treated with rosiglitazone and 158 patients not receiving rosiglitazone as controls, who were matched by baseline characteristics including level of HbA1c. Among patients with severe NPDR receiving rosiglitazone, the relative risk of progression to PDR at 3 years was reduced by 59% (P = 0.045), and this effect continued over 5 years of follow-up. Furthermore, at 5 years of follow-up, a significantly smaller proportion of patients in the rosiglitazone group experienced a decline of 3 or more lines in visual acuity (0.5% vs 38.0%; P = 0.03). No difference was found in the incidence of DME or CSME between the groups (P = 0.28). Initial case series and a prospective cohort-based electronic medical record-based review have reported the association of thiazolidinedione use and diabetic macular edema (OR 2.6; 95% CI 2.4–3.0). However, data from the largest clinical trial study to date to evaluate an association between thiazolidinedione exposure and DME in patients with type 2 diabetes demonstrated no such association. Thus, it appears that DME can occur at least sporadically with thiazolidinedione use, although this is relatively rare.
Other risk factors for proliferative diabetic retinopathy
Most studies seeking to identify risk factors for the development of PDR begin with patients who have various levels of NPDR or no visible retinopathy at all, and make comparisons of baseline factors between those who do and do not develop PDR. As expected, the significant risk factors for the development of PDR include increasing NPDR severity, decreased visual acuity, and elevated HbAlc. Additional risk factors included the presence of diabetic neuropathy, decreased hematocrit, increased serum triglyceride, and decreased plasma albumin.71 However, it should be noted that if the risk factors for progression from severe NPDR to PDR differ substantially from those mediating onset or progression of earlier NPDR previous studies may not have readily identified these differences.
The association of elevated serum lipids with increased risk of progression to high-risk PDR, as well as their association with increased hard exudates and decreased visual acuity,97 provide additional motivation for lowering the frequently elevated lipid levels observed in diabetic patients. Data from the ACCORD-EYE study show that DR progression rates were reduced from 10.2% with placebo to 6.5% with fenofibrate therapy for dyslipidemia (adjusted OR 0.60; 95% CI 0.42–0.87; P = 0.006).88 Severe anemia is a less frequently encountered problem in diabetic patients, but its association with increased risk of severe retinopathy has been suggested by ETDRS analyses and three other reports.71 Hypertension was not identified as a risk factor for development of high-risk PDR in the ETDRS, while findings in previous studies have been variable.7,71 In the UKPDS, patients with hypertension were randomized between more- and less-intensive regimens of blood pressure control, and retinopathy progression was significantly less common in the former, as was the incidence of photocoagulation and of a 3 or more line decrease in visual acuity. Risk reductions after 7.5 years ranged from 35% to 45% for these outcomes. Progression to PDR was too infrequent for meaningful analysis. A more detailed discussion of the epidemiology and risk factors for DR is presented in Chapter 45.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


