9 Prolactinomas and Apoplexy
Prolactin-secreting adenomas (prolactinomas) are the most common form of secreting pituitary tumors. Among pituitary tumors, they are second in frequency only to non-functioning adenomas. They account for 30% of all pituitary adenomas and 50 to 60% of functional pituitary tumors. Although it has been estimated that there are 100 cases per 1 million people, the authors of more recent studies describe that number as an underestimate of the true prevalence.1 Autopsy and radiologic studies indicate an overall prevalence of pituitary microadenomas from 10 to 25%, although most of these are thought to be insignificant.2
Prolactinomas present most commonly as microadenomas (<10 mm) causing a prolonged state of hyperprolactinemia. Macroadenomas (≥10 mm) also cause local mass effect on the rest of the gland as well as the adjacent structures. Prolactinomas can also be a manifestation of multiple endocrine neoplasia (MEN) type 1 syndrome or be familial.1
The need for surgical treatment of prolactinomas sharply declined after the U.S. Food and Drug Administration approval of bromocriptine in 1978. Medical treatment with dopamine agonists (D2 agonists) has become the mainstay for treatment of most prolactinomas, with a goal of normalizing prolactin levels as well as tumor shrinkage. Thus, the indications for treating prolactinomas surgically are evolving; these indications as well as the different surgical options available are discussed in this chapter.
 Clinical Manifestations of Prolactinomas
Clinical Manifestations of Prolactinomas
Patients with prolactinomas can present with the clinical sequelae of hyperprolactinemia, endocrine dysfunction, local mass effect, or pituitary apoplexy (Table 9.1). Despite an equal distribution of prolactinomas among men and women, women are four times more likely than men to be symptomatic. Women usually present earlier in the course of the disease, with smaller tumors at the time of diagnosis. Men’s loss of libido and impotence in cases of hyperprolactinemia are more commonly missed.
Patients with prolonged hyperprolactinemic states usually seek medical attention because of the effect of the hyperprolactinemia on the gonadal function and breast tissue, with a classic presentation of amenorrhea and galactorrhea in women and loss of libido in men. Prolactin inhibits the production of gonadotropin-releasing hormone at the level of the hypothalamus, resulting in hypogonadism and infertility. Children and postmenopausal women do not develop clinical symptoms of hypogonadism. Adolescents can present with delay or failure of sexual and reproductive development. Premenopausal women usually present with galactorrhea, amenorrhea, and infertility when their use of oral contraceptive regimen has been discontinued. Approximately 5% of women with primary amenorrhea and 25% of women with secondary amenorrhea (excluding pregnancy) have a prolactinoma.3 When galactorrhea accompanies amenorrhea, the incidence of a prolactinoma is as high as 80%.
Table 9.1 Clinical Manifestations of Prolactinomas
| Hyperprolactinemia |
| Amenorrhea (female patients) |
| Galactorrhea |
| Infertility |
| Decreased libido |
| Impotence (male patients) |
| Osteoporosis |
| Delayed puberty (adolescents) |
| Mass effect |
| Headaches |
| Visual acuity and field impairment |
| Cranial nerve palsies |
| Hypothalamic dysfunction |
| Hydrocephalus |
| Hypopituitarism |
| Pituitary apoplexy |
Untreated hyperprolactinemia also leads to premature osteoporosis in both sexes secondary to the estrogen and testosterone deficiency. The osteopenia is progressive and correlates with the duration of hypogonadism. Normalization of prolactin levels halts further bone loss, and some increase of bone density is seen, but normalization to baseline values is not the norm.
Prolactinomas can also present with symptoms due to local mass effect on local structures, such as headaches, visual compromise, cranial nerve palsies, hypopituitarism, and hydrocephalus. Suprasellar extension of the tumor to the visual apparatus most commonly results in a homonymous bitemporal hemianopsia, and cranial nerve palsies occur from lateral extension into the cavernous sinus.
Pituitary apoplexy (acute hemorrhage into or infarction of the pituitary adenoma) can present with acute signs of hypopituitarism and compression of the sellar and suprasellar structures. Patients present with a sudden onset of headache, nausea, vomiting, diplopia, visual loss, or a decreased level of consciousness.4 Signs of meningeal irritation can also be observed in cases in which the hemorrhage extends into the subarachnoid space. Pituitary apoplexy can occur in patients with a known prolactinoma or can be the cause of initial presentation of the patient.
 Differential Diagnosis of the Hyperprolactinemic State
Differential Diagnosis of the Hyperprolactinemic State
Before offering treatment to patients with hypogonadic dysfunction due to a hyperprolactinemic state, it is imperative to correctly differentiate patients who harbor a prolactinoma. The cause of hyperprolactinemia can be physiologic, pharmacologic, or pathologic (Table 9.2). A thyroid-stimulating hormone (TSH) level should always be measured simultaneously with a prolactin level because of the stimulatory effect of TSH on prolactin release by the pituitary gland. Lactotroph cells that secrete prolactin are stimulated by estrogen and inhibited by dopamine. Prolactin levels below 25 ng/mL in women and 20 ng/mL in men are within the normal range.
Physiologic hyperprolactinemia occurs in a variety of physical and psychological stress states, but the prolactin level rarely exceeds 40 ng/mL. It is imperative to rule out pregnancy as a cause because the prolactin level increases during the first and second trimester and peaks in the third trimester above several hundred nanograms per milliliter. Prolactin levels rapidly decrease in the postpartum period in women who do not breast-feed. In women who breast-feed, prolactin levels decrease after a few weeks despite surges after suckling. Within a few months, prolactin levels return to normal even if breast-feeding is continued.
Macroprolactin can be responsible for hyperprolactinemia in up to 20% of cases.5 Macroprolactin, a complex of prolactin and immunoglobulins, has a longer half-life than free prolactin and may cause an increase of the total level of prolactin in the blood.5 It is generally thought that macroprolactin does not have any biologic effect, and several laboratory tests can be used to differentiate macroprolactin from free prolactin levels.
Medications are a common cause of hyperprolactinemia, which can be seen with any agent that antagonizes dopamine receptors on lactotroph cells in the pituitary gland. Antidepressant therapies, antihypertensive drugs, and estrogen can induce hyperprolactinemia, resulting in prolactin levels in the range of 25 to 100 ng/mL. The hyperprolactinemia usually resolves in a few days to weeks after cessation of the offending medication.6
Table 9.2 Causes of Hyperprolactinemia
| Physiologic Pregnancy |
| Breast-feeding (suckling reflex) |
| Stress |
| Exercise |
| Pharmacologic |
| Neuroleptic medication (phenothiazines, haloperidol) |
| Atypical antipsychotic medications (clozapine, risperidone) |
| Antidepressant medication (tricyclics, monoamine oxidase inhibitors, selective serotonin reuptake inhibitors) |
| Antihypertensive medication (α-methyldopa, reserpine, verapamil) |
| Metoclopramide |
| H-2 blockers |
| Sellar/parasellar lesions |
| Prolactinomas |
| Pituitary adenomas with stalk effect |
| Germinomas |
| Craniopharyngiomas |
| Meningiomas |
| Primary empty sella syndrome |
| Lymphocytic hypophysitis |
| Histiocytosis X |
| Sarcoidosis |
| Metastasis |
| Other |
| Primary hypothyroidism |
| Hypothalamic dysfunction |
| Chronic renal failure |
| Liver failure |
| Ectopic secretion of prolactin |
| Seizures |
| Macroprolactin |
Primary hypothyroidism causes hyperprolactinemia in 20 to 30% of patients because of the effects of an increased thyrotropin-releasing hormone. Thyrotroph hypertrophy as well as pituitary hyperplasia may ensue and in rare cases may cause visual field defects. Correction of primary hypothyroidism leads to normalization of prolactin levels within a few months. Chronic renal failure also results in hyperprolactinemia because of a decreased renal clearance of serum prolactin.
Any mass in the sellar and suprasellar region can interrupt the dopaminergic inhibition of the lactotrophs and result in a state of hyperprolactinemia from “stalk effect.” The stalk effect rarely induces prolactin levels above 150 ng/mL, although rare cases of significant elevation have been reported.3 In some cases of acromegaly, prolactin can be co-secreted with growth hormone, and some rare cases of Cushing’s disease have also been described with co-secretion of prolactin.
Most cases of hyperprolactinemia that are not related to the presence of a prolactinoma can be ruled out based on the patient’s history and physical examination. In case of doubt, magnetic resonance imaging (MRI) of the pituitary with and without gadolinium enhancement is used to correlate the level of the hyperprolactinemia with the radiologic findings of an adenoma. Patients with visual loss based on physical and radiologic findings should be evaluated by formal visual field testing. All patients with radiologic signs of a pituitary adenoma should also be evaluated with a pregnancy test (in women of child-bearing age), thyroid and renal function tests, and a full evaluation of other pituitary hormones (growth hormones, insulin-like growth factor-1, fasting morning cortisol, thyroid function tests, adrenocorticotrophic hormone, luteinizing hormone, follicle-stimulating hormone, sex hormones).
 Laboratory and Radiologic Correlation of Prolactin Levels
Laboratory and Radiologic Correlation of Prolactin Levels
Correlating the degree of hyperprolactinemia with the radiologic findings is important to make a correct diagnosis of a pituitary prolactin-secreting adenoma. Patients with a microprolactinoma typically have prolactin levels in the range of 100 to 250 ng/mL. Patients with a macroprolactinoma typically have levels above 250 ng/mL. In cases in which a lateral extension of the tumor is seen toward the cavernous sinus, the serum prolactin level may attain a level of several thousand nanograms per milliliter. A falsely low prolactin level (25 to 150 ng/mL) is observed in some cases of large prolactin-secreting macroadenomas with very high levels of prolactin that induce a high-dose “hook effect.”7 The hook effect is observed when using radioimmunoassays with a monoclonal sandwich technique where both the capture and signal antibody become saturated. The hook effect can be overcome by performing serial dilutions of the serum samples.
 Radiologic Characteristics of Prolactinomas
Radiologic Characteristics of Prolactinomas
All patients with a suspected prolactinoma should undergo MRI scanning with and without the use of gadolinium. MRI has replaced the need for any other imaging. Coronal and sagittal views centered on the pituitary gland should be obtained. On T1 sequences obtained immediately after injection of gadolinium, pituitary adenomas including prolactinomas present as hypointense lesions compared with the rest of the normal pituitary tissue. On delayed T1 sequences after gadolinium administration, prolactinomas are hyperintense to the rest of the pituitary gland because of a washout phenomenon (Fig. 9.1). Small microprolactinomas may easily be missed if a dynamic study is not performed. Coronal views enable the surgeon to evaluate the anatomy of the sphenoid septa as well as the carotid arteries to ensure a transsphenoidal approach can safely be performed if surgery is contemplated.
 Medical Treatment of Prolactinomas
Medical Treatment of Prolactinomas
Prolactinomas can be controlled medically with the use of dopamine agonists. These agents bind the lactotrophs on their D2 receptors and inhibit prolactin synthesis and release. Bromocriptine accomplishes tumor shrinkage and control of microprolactinomas in approximately 85% of cases.8 Bromocriptine dosing is usually started at 1.25 to 2.5 mg per day and is slowly increased to a total dose of 5 to 10 mg per day. The initial treatment is usually started with oral intake of the medication at bedtime to limit side effects of orthostatic hypotension. Side effects are a limiting factor in 5 to 10% of cases and consist of dizziness, nausea, arrhythmias, and gastrointestinal discomfort. Cabergoline can be used as an alternative to bromocriptine because it has fewer side effects and superior efficacy (Fig. 9.2).9 Overall tumor shrinkage and normalization of prolactin levels are superior to those of bromocriptine, but the cost of treatment is higher.10 Treatment is usually started at 0.5 to 1.5 mg once or twice per week. Similar dose escalation may be necessary when treating large tumors, with subsequent decrease of the dose after tumor shrinkage has been accomplished. Cabergoline is most useful in patients who are resistant to bromocriptine or who cannot tolerate its side effects.9 After several years of normoprolactinemia under medical treatment, an attempt at weaning the patient from dopamine agonist therapy can be accomplished, with a sustained biochemical cure in up to 38% of cases of microprolactinomas.11 Normoprolactinemia seems to be more common after cabergoline withdrawal and has been reported in 22 to 59% of cases of microprolactinomas and in 11 to 23% of cases of macroprolactinomas.10 Prolonged normoprolactinemia is more probable in cases in which the tumor disappeared on imagery during dopamine agonist treatment, in cases of microprolactinomas, and in cases of prolonged normoprolactinemia on medical treatment for at least 1 year before drug withdrawal.10 Long-term data are not available to determine the durability of normoprolactinemia after dopamine agonist withdrawal. Recurrences of hyperprolactinemia are associated with a radiologically observable rate of tumor growth in 10% of cases of microprolactinomas.12 Alternatives to bromocriptine and cabergoline have been developed with the use of pergolide, lisuride, and quinagolide, but the experience with these options is very limited in North America.
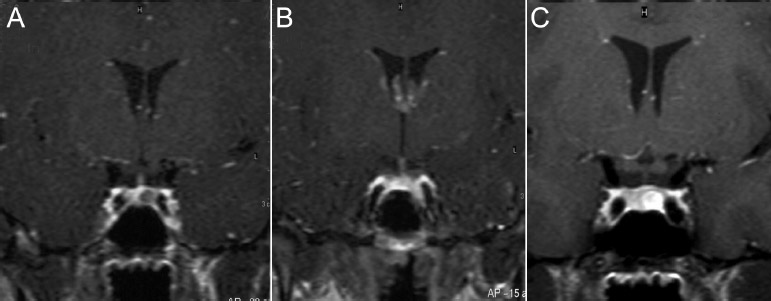
Fig. 9.1 Coronal T1-weighted MRI views of a microprolactinoma during a dynamic study. (A)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


