2 Anatomy of the Pituitary Gland and Parasellar Region
The pituitary gland is a remarkable organ that is located at the base of the brain at the center of the skull base. The gland controls an array of endocrine functions important for human growth and metabolism. The most common pituitary-related pathologies that are surgically treated are pituitary tumors (mostly adenomas) and pituitary apoplexy. The classic indications for surgical treatment include visual loss from progressive mass effect, hormonal control in hyperfunctioning adenomas, failure of medical therapy, and necessity for a tissue diagnosis.1 Transcranial approaches to the sella for treating pituitary pathologies have been in existence since the late 19th century. In the early 1900s, Hirsch described a transnasal approach to the sella turcica that was refined by Cushing, who standardized the translabial, transseptal, transsphenoidal approach to the pituitary gland.2
Recently, given the technologic enhancements in endoscopic visualization and instrumentation, the endonasal endoscopic approach has gained popularity for addressing pathology of the pituitary gland. Regardless of the surgical approach, a commanding knowledge of the anatomy of the pituitary gland and parasellar region is critical for surgeons operating in this area. This chapter addresses the anatomy of the pituitary gland and parasellar region as well as the surrounding anatomy of the cavernous sinus, suprasellar region, and third ventricle. In addition, anatomical principles emphasized by the endoscopic approach are also discussed in greater detail. Although these anatomical relationships are not new, the endoscopic approach places these anatomical concepts in a different light and therefore are important to understand and appreciate.
 Pituitary Gland
Pituitary Gland
The pituitary gland is composed of an anterior and a posterior lobe that are embryologically, anatomically, and functionally distinct. The anterior lobe surrounds the lower part of the pituitary stalk to form the pars tuberalis (Fig. 2.1A). The pituitary stalk generally attaches to the anterosuperior portion of the pituitary gland. If the anterior lobe is separated from the posterior lobe, the pars tuberalis tends to remain with posterior lobe. The anterior lobe is firmer but easily separated from the anterior and lateral sellar walls.
The posterior lobe, on the other hand, is softer and gelatinous. However, it is more firmly attached to the sellar walls and thus sometimes is difficult to remove. The inferior surface of the gland conforms to the sella floor, whereas the shape of the superior and lateral surfaces of the gland is variable because they border soft tissue structures, namely, the cavernous sinus and diaphragma sellae. The superior surface is usually ovoid and may become triangular in shape if the carotid arteries compress the gland laterally and posteriorly (Fig. 2.1B). The width of the pituitary gland is usually equal or slightly larger than the length or depth of the gland. In addition, the superior surface of the posterior gland may be distinguished from the anterior lobe by its lighter color. This is an important anatomical point that can help to distinguish the two lobes when the pituitary is approached transcranially.3
Given its central location, the pituitary gland is surrounded by several critical neurovascular structures. These include the optic nerves, optic chiasm, and anterior circulation superiorly (Fig. 2.2A); the cavernous sinuses, internal carotid arteries, and cranial nerves laterally; and the brainstem and posterior circulation posteriorly (Fig. 2.2B). Anteriorly, the pituitary gland is enclosed by the sphenoid sinus and frontal lobes (Fig. 2.2C). These critical neurovascular structures, often separated by a few millimeters, surround the pituitary gland superiorly, laterally, and posteriorly and therefore make anterior-based approaches the preferred and safest surgical routes to the sellar region.
 Sphenoid Bone
Sphenoid Bone
The complexity of the neurovasculature surrounding or traversing the sphenoid bone necessitates a thorough knowledge of its bony anatomy. More importantly, the sphenoid bone contributes in large measure to the anatomy of the sella and parasellar region, making its anatomy important for any pituitary surgeon. The sphenoid bone is a butterfly-shaped bone divided into the body of the sphenoid centrally, a single greater and lesser wing bilaterally, and pterygoid processes pointing inferiorly from the body of the sphenoid bone. The lesser wings originate from the superomedial part of the central bone, and the greater wings emanate from the lower part of the central bone. The lesser wing of the sphenoid along with the planum sphenoidale contribute to the anterior cranial base, which houses the olfactory tracts, gyrus rectus, and posterior part of the frontal lobe. The lesser wing also contributes to the posterior part of each orbit. In close association to these central bony structures lie the pituitary gland, optic chiasm, as well as several cranial nerves traversing various foramina located in the sphenoid bone. The lateral part of the middle cranial base is formed by contributions from the lesser and greater wings of the sphenoid bone, which house the temporal lobe. The greater wing also forms the lateral wall of the orbit and the roof of the infratemporal fossa3,4 (Fig. 2.3A).
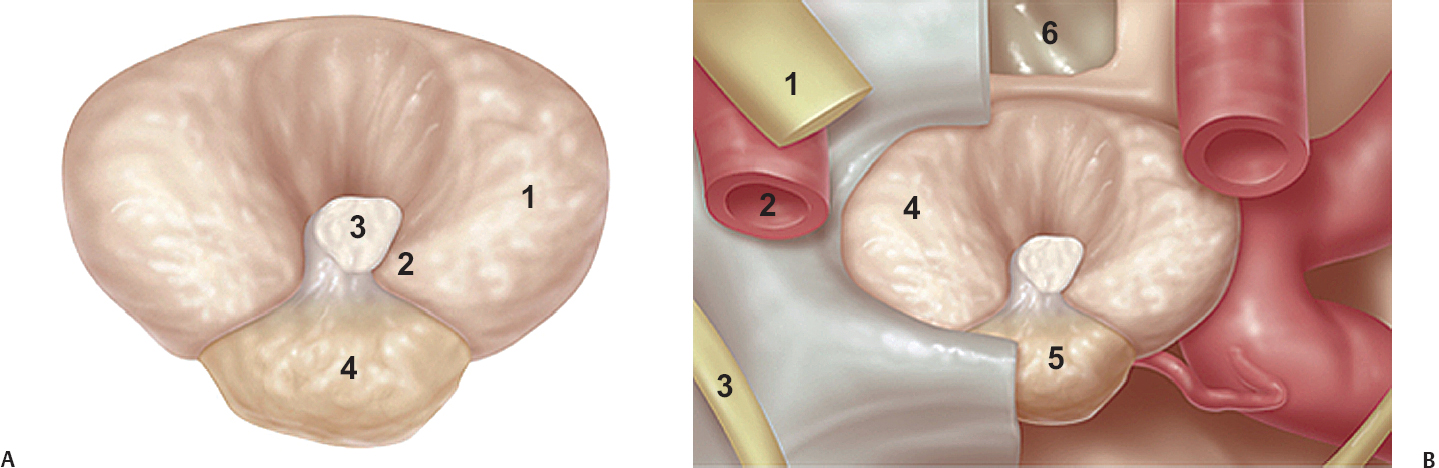
Fig. 2.1 (A) The pituitary gland may be divided into a firmer anterior lobe and a softer, gelatinous posterior lobe. The anterior lobe surrounds the pituitary stalk to form the pars tuberalis. 1, anterior lobe; 2, pars tuberalis; 3, pituitary stalk; 4, posterior lobe. (B) The superior surface of the pituitary gland is usually ovoid and may become triangular if the carotid arteries compress the gland posteriorly and laterally. The posterior gland may also be distinguished from anterior lobe by its lighter color. 1, optic lobe; 2, internal carotid; 3, oculomotor nerve; 4, anterior pituitary; 5, posterior pituitary; 6, sphenoid sinus.
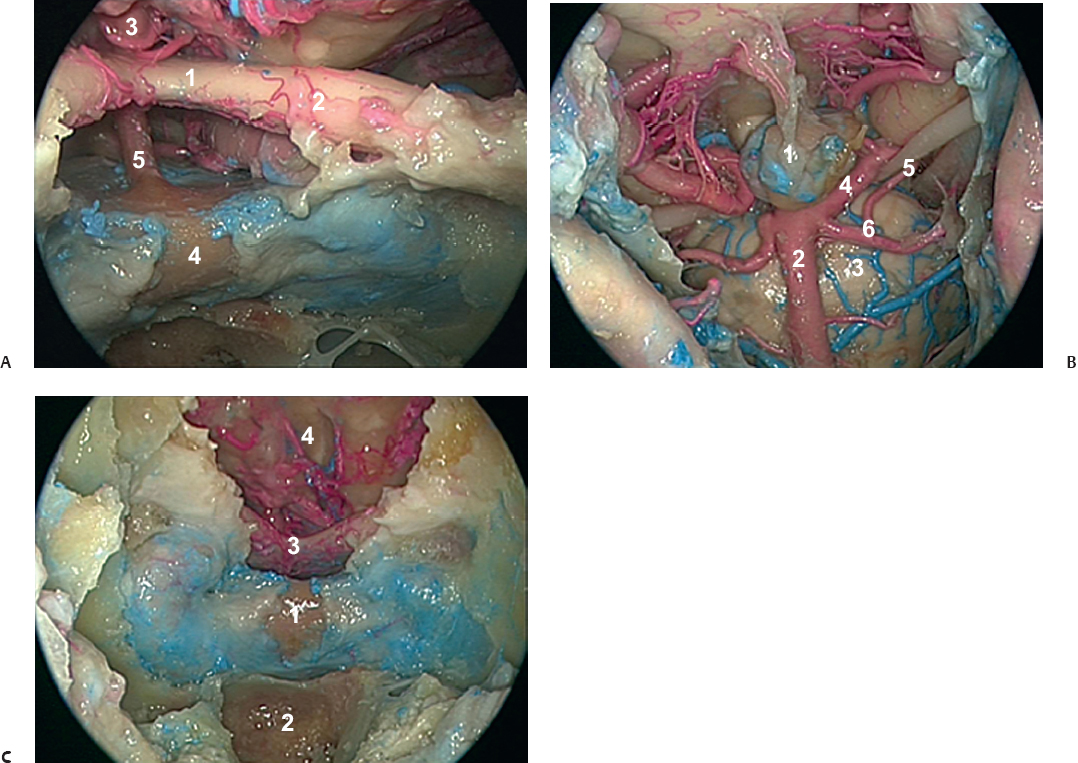
Fig. 2.2 (A) The pituitary gland is flanked by the optic chiasm and anterior cerebral circulation superiorly and the optic nerves supero-medially. 1, optic chiasm; 2, optic nerve; 3, anterior cerebral circulation; 4, pituitary gland; 5, pituitary stalk. (B) The pituitary gland is surrounded by the brainstem and posterior circulation posteriorly. 1, pituitary gland; 2, basilar artery; 3, brainstem; 4, posterior cerebral artery; 5, oculomotor nerve; 6, superior cerebral artery. (C) The pituitary gland is enclosed by the sphenoid sinus anteriorly and the frontal lobes anterosuperiorly. 1, pituitary gland; 2, sphenoid sinus; 3, optic chiasm; 4, frontal lobes.
Several cranial nerves traverse multiple foramina formed within the sphenoid bone. The superior orbital fissure, located between the inferior margin of the lesser wing and the superior margin of the greater wing of the sphenoid bone, is negotiated by the oculomotor, trochlear, abducens, and ophthalmic branch of the trigeminal nerve. The optic canals, which transmit the optic nerves, are located above and medial to the superior orbital fissure, separated by a ridge of bone called the optic strut. Extracranially, the optic strut corresponds to the lateral opticocarotid recess, an important anatomical landmark on the lateral sphenoid wall during transsphenoidal surgery. Other important foramina embedded in the sphenoid bone, located at the junction of the body and greater wing, are the foramen rotundum, pterygoid canal, foramen ovale, and foramen spinosum. The major structures passing through these foramina are the maxillary nerve, vidian nerve, mandibular nerve, and middle meningeal artery, respectively5 (Fig. 2.3B).
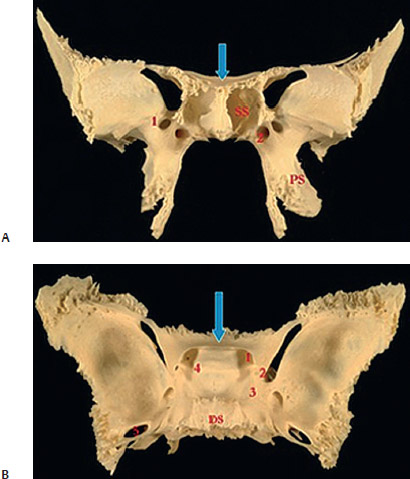
Fig. 2.3 (A) The lesser wing, greater wing, and pterygoid process emanating from the butterfly-shaped central sphenoid bone seen from an anterior-posterior view. 1, forcemen rotundum; 2, vidian canal; arrow, planum sphenoidale. (B) Anatomical landmarks and em-bedded foramina of the sphenoid bone as seen from a superior view. 1, optic canal; 2, anterior clinoid; 3, groove of internal carotid artery; 4, middle clinoid; 5, foramen ovale; 6, posterior clinoid; DS, dorsum sellae; arrow, planum sphenoidale.
Important vascular structures have an intimate relationship with the sphenoid bone. The internal carotid arteries project into the sphenoid bone and form prominences in the lateral wall of the sphenoid sinus. The cavernous sinuses, discussed later in greater detail, lie on the lateral aspect of the pituitary gland and serve as a conduit for lateral extension of some pituitary adenomas. Intercavernous sinuses pass through the sellar cavity and dorsum sellae. Finally, the basilar artery lies on the posterior surface of the sphenoid bone, which contributes to the superior clivus (Fig. 2.2B)
 Sellar Bone
Sellar Bone
The sella turcica is a bony region of the sphenoid bone that houses the pituitary gland. The gland is limited anteriorly by the tuberculum sellae and posteriorly by the dorsum sellae. The tuberculum is a thick ridge of bone connecting the sellar fossa to the planum sphenoidale. Between the tuberculum sellae and planum sphenoidale lies a depression bounded laterally by the optic foramina called the chiasmatic sulcus. The optic chiasm usually lies posterior to this bony landmark. The sella turcica has three bony spicules or prominences; namely, the middle, anterior, and posterior clinoid processes, the latter two of which provide attachment to the tentorium cerebelli. The anterior clinoid processes are located at the medial edge of the lesser wings, the middle clinoid processes lateral to the tuberculum sellae, and the posterior clinoid processes on the superolateral margin of the dorsum sellae (Fig. 2.3B). The depth or height of the sella is usually determined by the sellar floor and a perpendicular line connecting the tuberculum and dorsum. The length of the sella is the largest anterior-posterior dimension of the pituitary fossa, typically located at the level of the tuberculum. The greatest distance between the two carotid sulci is considered the sellar width.
 Sphenoid Sinus
Sphenoid Sinus
The sphenoid sinus, contained within the central part of sphenoid bone, is widely considered the gateway to the pituitary gland, parasellar region, and anterior skull base. It is a large paranasal sinus located posterior to the ethmoid sinuses, typically divided into two unequal halves by a single vertical septation. However, it is not uncommon to find multiple complete and incomplete septations dividing the sinus into several cells, complicating the descriptive anatomy of this region.3,6 The major vertical septation often continues posteriorly to the face of the sella. However, it may localize to either of the carotid siphons, emphasizing the need for atraumatic dissection while removing these septations to avoid damage to the underlying vascular structures (Fig. 2.4). Single septations are found 68% of the time, and these septations may be found as much as 8 mm off the midline.7
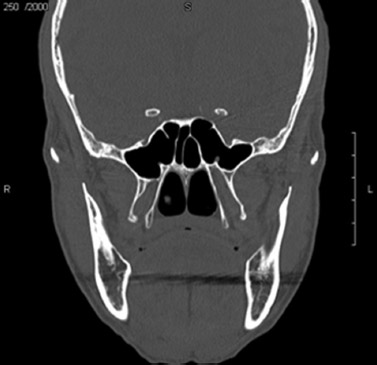
Fig. 2.4 Computed tomography image of a well-pneumatized sphenoid sinus with multiple vertical, horizontal, and oblique septations.
The natural sphenoid sinus ostium is elliptical and usually located in the anterosuperior aspect of the anterior sphenoid sinus wall approximately 1.5 cm superior to the posterior choanae in the sphenoethmoidal recess adjacent to the posterior tip of the middle turbinate and inferior edge of the superior turbinate (Fig. 2.5). The Onodi cell, when present, represents pneumatization of a posterior ethmoid cell into the sphenoid sinus and may distort identification of the true sphenoid sinus. It is present in 7 to 25% of patients and must be recognized radiographically and endoscopically prior to embarking on a skull base approach or endoscopic sinus surgery. This is important because of the passage of the optic nerve in the lateral wall of the cell8 (Fig. 2.6).
The sphenoid sinus is variably pneumatized and is characterized by the position of the sinus in relationship to the sella turcica. Pneumatization is classified into sellar (80%), presellar (17%), and conchal (3%) types. A sellar sphenoid sinus has extensive pneumatization anteriorly and inferiorly to the sellar protuberance, making identification of intrasphenoidal anatomical landmarks easier during endoscopic transsphenoidal surgery. A presellar pneumatization pattern has pneumatization anteriorly, making the sellar protuberance and other landmarks slightly more difficult to identify. Finally, no pneumatization exists for the conchal type of sphenoid sinus, common in children younger than 12 years of age, which poses a challenging anatomical dissection for the management of any pituitary or anterior skull base lesion8 (Fig. 2.7). In this pattern, the bone separating the sella from the sphenoid sinus is usually greater than 10 mm.3
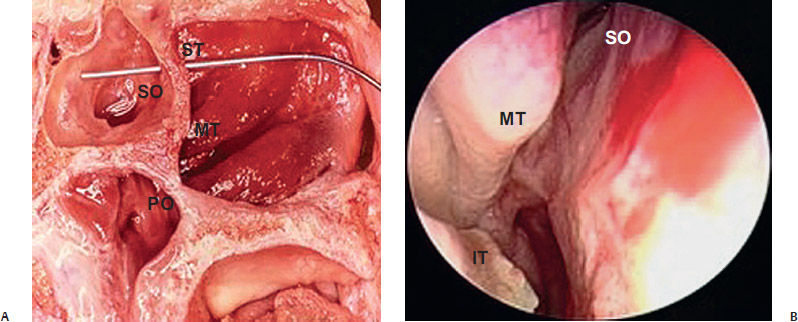
Fig. 2.5 (A) Sagittal cadaveric dissection demonstrating the location of the natural sphenoid sinus ostium. (B) Endoscopic image demonstrating the location of the sphenoid sinus ostium in relationship to the superior turbinate. IT, inferior turbinate; MT, middle turbinate; PC, posterior choanae; SO, sphenoid ostium.
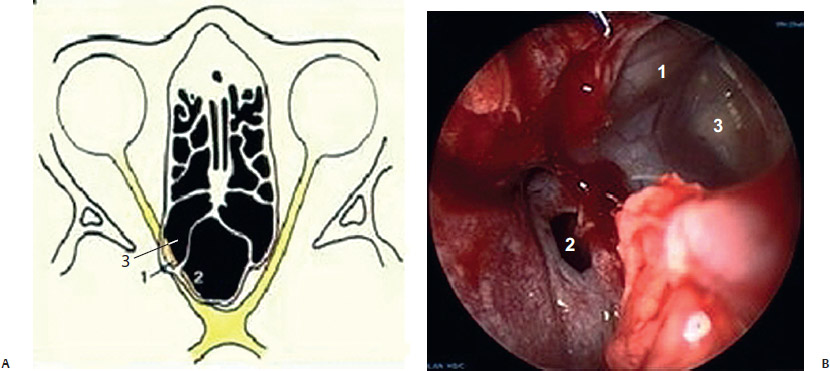
Fig. 2.6 (A) Axial image of the posterolateral pneumatization of a posterior ethmoid cell termed an Onodi cell. (B) Endoscopic image of a left Onodi cell, demonstrating the optic nerve running in its superior lateral corner. 1, optic nerve; 2; sphenoid sinus; 3, onodi cell.
Image guidance is critical for a transsphenoidal approach through a conchal sphenoid sinus to avoid straying laterally while drilling.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


