7
Principles of Cochlear Implant Imaging
Andrew J. Fishman and Roy A. Holliday
Radiographic imaging plays a major role in cochlear implantation with regard to preoperative candidacy evaluation, intraoperative monitoring, postoperative evaluation, as well as research and experimental techniques. At a minimum, successful cochlear implantation requires that electrical impulses be delivered to a surviving spiral ganglion cell population, and that these impulses be transmitted to a functioning auditory cortex by an existent neural connection. Accordingly, imaging the auditory pathway of the implant candidate is necessary to screen for morphological conditions that preclude or complicate the implantation process. Increasing resolution of computed tomography (CT) and magnetic resonance imaging (MRI) technology has provided the clinician with more detailed information about the integrity of the auditory pathway. As technologies evolve, a clear understanding of what information can be obtained as well as the limitations of various imaging modalities is essential to proper candidacy evaluation, and selection of the ear to be implanted in complex cases.
Also important is the effect that the presence of a cochlear implant has on future imaging of the head and neck region of an implantee. In the past, the presence of a cochlear implant was considered to be a major contraindication to MRI.1 Because it is now possible to obtain useful images with advances in CT and MRI technology, the issue of device MRI compatibility has opened up a new area of investigation.
♦ Preoperative Imaging
Preoperative imaging is instrumental in determining the feasibility and facility of cochlear implantation. Analysis is performed in a stepwise approach, answering the following three questions: Are there cochleovestibular anomalies that preclude implantation? Is there evidence of luminal obstruction? Are there additional findings that may complicate the surgery or subsequent patient management? This section is not intended to review principles or techniques of image acquisition, but rather to provide a platform for discussion between the implant team and the radiologist.
Are There Cochleovestibular Anomalies that Preclude Implantation?
Approximately 20% of patients with congenital sensorineural hearing loss (SNHL) have radiographically identifiable morphological abnormalities of the inner ear.2 In general, inner ear malformations can be associated with a wide range of hearing sensitivity.3 These patients can manifest progression of hearing loss, though many may retain useful hearing into adult life. As a general rule, however, the more severe the deformity, the worse the hearing.3 Due to the variability and progressive nature of hearing loss in these disorders, most large implant centers are likely to evaluate patients with a variety of malformations. Given the current technology, the minimum requirement for cochlear implantation is the presence of an implantable cavity in proximity to stimulable neural elements whose projections connect to the auditory cortex. Accordingly, the first question that must be answered is the following: Are there any cochleovestibular anomalies that preclude implantation?
Embryology
To fully appreciate the wide variety of possible cochleovestibular malformations, it is helpful to first review the embryogenesis of the inner ear.3,4 We will consider separately the formation of the membranous labyrinth, the bony otic capsule, and the cochleovestibular nerves and ganglia.
The development of the combined cochlear and vestibular membranous labyrinthine system begins with the formation of the otic placode as an ectodermal thickening that forms on the surface of the neural tube in the third gestational week. The otic placode invaginates from the surface and forms the otocyst in the fourth gestational week. The otocyst develops three infolds in the fifth week. The resultant pouches represent the primordial endolymphatic sac and duct, the utricle and semicircular canals, and the saccule and cochlea. Beginning in the sixth week, the cochlear duct grows from its primordial bud beginning from the basal region spiraling apically to reach its full 2.5 to 2.75 turns by the eighth to tenth week. The neuroepithelial end organs continue to develop beyond this period with the organ of Corti completing its formation in the 25th week.
The semicircular canals begin their formation as three small, folded evaginations on the primordial vestibular appendage. They develop as disk-like outpouchings whose centers eventually compress and fuse to ultimately form the semicircular duct structure. By the sixth week of gestational life, this compression and fusion has taken place in first the superior and then the posterior canals. The three canals continue to enlarge and complete their formation to full adult size in sequence beginning with the superior around the 20th week, and followed by the posterior and finally the lateral semicircular canals. Interestingly, the endolymphatic sac and duct are the first to appear and the last to complete their development.
The osseous otic capsule eventually forms from a morphologically fully developed cartilage precursor model via 14 centers of ossification, beginning around the 15th gestational week, and is completed during the 23rd gestational week. The cartilage model and underlying membranous labyrinth continue to grow in the region of the posterior and lateral semicircular canals, while other structures, which have previously attained their final shape and size, have begun ossifying. The cochleovestibular nerves and ganglia develop in concert with the membranous labyrinth and cochleovestibular end organs. They are of neural crest origin and migrate between the epithelial layer and basement membrane of the otic vesicle during the fourth gestational week.
Cochlear Malformations
There is much confusion in the literature regarding the nomenclature of cochlear morphologic anomalies especially regarding the term Mondini malformation. In 1791, Carlo Mondini presented his findings on an anatomical dissection of a young deaf boy.5 According to his writings, prior reports of human deafness were attributed to abnormalities of the external auditory canal and eustachian tube, tympanic membrane, middle ear and ossicles, or compression of the auditory nerve. During his dissection on the posterior face of the petrous bone, he discovered significant vestibular aqueduct enlargement and commented that the usual bony lip that “protects the vestibular aqueduct” was missing and was substituted by a membranous plate of dura. He noted that the vestibule was not deformed but was of greater than usual size. He also noted an increase in the size of the elliptical recess though it was normal in shape. He commented that the semicircular canals appeared normal and that the positions of their openings into the vestibule were unremarkable. In observing the medial opening of the vestibular aqueduct, he commented that it was quite enlarged and was larger than the size of the common crus. The cochlea was described as possessing only 1.5 turns and ending in a cavity corresponding to the last spiral turn. He also described an incompletely formed interscalar septum. The more contemporary term incomplete partition is commonly used to describe this classic anomaly and denotes this specific aspect of the deformity.3,6 In this historic subject, the deformity was bilateral.
Because of its relative frequency as well as its historic significance, the term Mondini malformation is commonly used to describe all forms of cochlear morphological abnormalities and not just the incomplete partition. The term Mondini dysplasia was used by Schuknecht7 in an in-depth analysis of the histopathology and clinical features of cochlear anomalies. Schuknecht’s treatise described a variety of malformations including one patient with “the normal 2.5 turns but measur[ing] only 23 mm in length (normal: 32 mm)” and another with “Mondini dysplasia limited to the vestibular system,” as well as several patients with cochleae possessing 1.5 turns, and other variant morphologies of both the cochlear duct and vestibular system. Schuknecht histologically described these malformations as isolated findings or in association with the Klippel-Feil, Pendred, and DiGeorge syndromes. His work detailed the clinical nature of these disorders as being unilateral or bilateral, and associated with acoustic and vestibular dysfunction that is variable in severity, static, or progressive.
Phelps8 reserves the term Mondini deformity for cochleae whose basal turns are normal and possess a deficiency of the interscalar septum of the distal 1.5 coils. He differentiates these cochleae from those termed dysplastic owing to their widened basal turn being in wide communication with a dilated vestibule. According to Phelps the significance is in the clinical absence of a spontaneous cerebrospinal fluid (CSF) leak and meningitis in patients with his strict definition of Mondini deformity as opposed to those patients with dysplasia who did manifest these complications in a series of 20 patients studied.
Since the writings of Mondini, several investigators have documented a variety of inner ear malformations. Though not the first to describe or name these malformations, Jackler et al3 in 1987 proposed a classification system for the congenitally malformed inner ear based on the theory that a variety of deformities result from arrested development at different stages of embryogenesis. The authors clearly stated that their classification could not describe all observable abnormalities but was meant to serve as a framework upon which other describable anomalies could be added, which by their supposition would have resulted from aberrant, rather than arrested, development.
This body of work warrants mention as it is often cited and serves well as an initial systematic basis for the interpretation of images. Jackler et al formulated their classification system upon review of polytomes and CT scans of 63 patients with 98 congenitally malformed ears, and provided the following categorization (Table 7–1). The disorders identified as having normal cochleae were subdivided out solely for the purposes of Jackler’s classification scheme. It is important to recognize that disorders of the vestibule, semicircular canals, and vestibular aqueduct are also often found in conjunction with cochlear malformations. Inner ear deformities tend to occur bilaterally in 65%.3 When bilateral, there is a 93% chance that they will be similar, though various combinations of morphological classes have been documented.3
| Absent or malformed cochleae |
| 1. Complete labyrinthine aplasia |
| 2. Cochlear aplasia |
| 3. Cochlear hypoplasia |
| 4. Incomplete partition |
| 5. Common cavity |
| Normal cochleae |
| 1. Vestibule: lateral semicircular canal dysplasia |
| 2. Enlarged vestibular aqueduct |
Complete labyrinthine aplasia, also called Michel deformity, could result from arrest prior to formation of the otocyst, resulting in complete absence of inner ear development.3 This is the rarest among the above classified malformations (Fig. 7–1).
Cochlear aplasia is defined as an absent cochlea with an intact but often variably deformed vestibular labyrinth. This is the second rarest cochlear malformation noted by Jackler et al, representing ˜3% of identified cochlear malformations.
The term cochlear hypoplasia has been used to describe a range of abnormalities from a rudimentary cochlear diverticulum to an incompletely formed cochlear bud of several millimeters (Fig. 7–2). This group comprised 15% of cases from Jackler et al; it was thought to represent arrested development during the sixth gestational week, and may be associated with either a normal or malformed vestibule and semicircular canals.
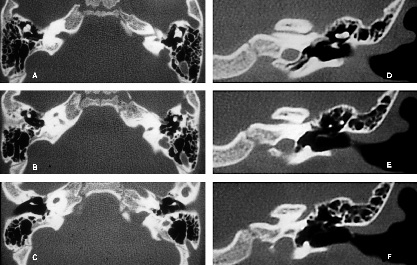
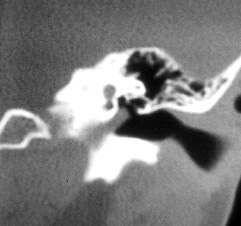
Figure 7–1 Computed tomography (CT) scan of a patient with a common cavity deformity on the right and complete cochleovestibular aplasia on the left. Axial sections (A,B,C) are depicted from superior to inferior. (A) A narrow internal auditory canal (IAC) on the left containing only a facial nerve. (B) The IAC on the right communicating with the common cavity. Coronal sections through the left temporal bone (D,E,F) demonstrate the absence of the otic capsule with only the carotid and facial nerve canals visible in the region. (D) The tensor tympani muscle. This patient was successfully implanted in the right ear.
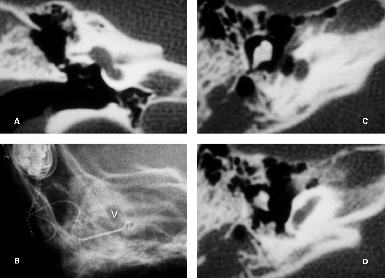
Figure 7–2 CTscan of a patient with bilateral cochlear hypoplasia. Images are shown from the right temporal bone that was successfully implanted. (A) A coronal section through the vestibule demonstrates the relatively normal formation of the vestibular apparatus as well as the presence of an oval window. (B) An intraoperative transorbital plain radiograph of the multichannel electrode array implanted in this patient. This is the expected appearance of the array placed into this small cavity. Note that the morphology is quite similar to the coronal section (A). V, vestibule; marked for reference. (C) The oval window and ossicles are also seen in axial image. These are useful surgical landmarks because they allow for the formation of a topographic roadmap when implanting abnormal cochleae. (D) Only the proximal basal turn of the cochlea is present. The middle or apical turns are absent.
Incomplete partition is a term used by Jackler et al in their study, and it is pointed out that this is the closest to the malformation originally described by Mondini. This is the most commonly described cochlear abnormality, making up 55% of the study described. It is thought to represent arrest in development during the seventh gestational week, a time at which the cochlea would have completed 1 to 1.5 turns.3 Radiographically, these cochleae possess only 1.5 turns comprised of a basal turn leading to the appearance of a confluent middle and apical turn, which may also be viewed and described as incomplete partitioning by a deficient interscalar septum.3,6 These cochleae may also manifest varying degrees of abnormalities of the vestibular system and endolymphatic duct and sac (Fig. 7–3).
The term common cavity is used to denote confluence of the cochlea and vestibule into a common rudimentary cavity that usually lacks an internal architecture and is often associated with abnormally formed semicircular canals. This is the second most common abnormality described, and made up 26% of the Jackler et al study (Fig. 7–4).
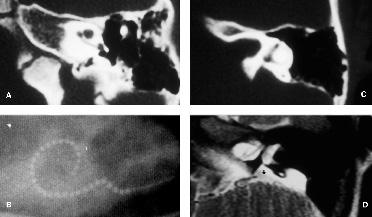
Figure 7–3 Images from a patient with bilateral incomplete partition. (A) Axial CT scan clearly depicts an intact basal turn and confluent middle and apical turns. (B) Note that a multichannel electrode array was implanted nearly a full turn with a few stiffening rings remaining outside the cochleostomy. This patient also has a wide vestibular aqueduct as seen in the axial CT image (C) as well as in the T2-weighted magnetic resonance imaging (MRI) (D) marked by (*). Intraoperatively, egress of cerebrospinal fluid (CSF) was easily controlled with packing of fascia around the array at the cochleostomy.
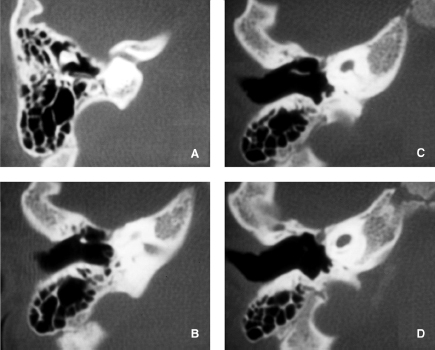
Figure 7–4 Axial CT scan of the right temporal bone from the patient in Fig. 7–1. Sections are depicted from superior to inferior (A–D). Note the labyrinthine facial nerve passing anteriorly and superiorly to the common cochleovestibular chamber. (A) In this patient the semicircular canals are absent. The bony cochlear aqueduct is visible (C,D).
The classification scheme proposed by Jackler et al is not all-inclusive. There are varieties of disorders that may be encountered that defy classification, as the authors well noted. A very narrow internal auditory canal of a diameter 2 to 2.5 mm or less on either conventional or CT has been reported in association with a normal inner ear as well as a variety of inner ear malformations.9–12 It has been reported unilaterally and bilaterally, in association with a variety of other congenital anomalies and as an isolated disorder. The clinical significance of this finding on a preimplant evaluation is that there is a high likelihood that it indicates the presence of only a facial nerve and the absence of the cochleovestibular nerve. A CT scan demonstrating an internal auditory canal of less than 2 to 2.5 mm is considered by many authors to be an absolute contraindication to cochlear implantation.9,10,13 Evaluation of the contents of the internal auditory canal using MRI scanning may be warranted in selected patients, as increased experience is being gained with high-resolution scanning techniques.
There is also a particular form of X-linked deafness that has been both radiographically described and genetically identified.10,14,15 It is seen in some severely deaf males who have a deficiency of bone between the lateral end of bulbous internal auditory canal and the basal turn of the cochlea.10 It has been detailed by both CT and MRI and it entails the clinical implication that there is an obvious large communication between the CSF-containing internal auditory canal and the cochlea. This situation also causes concern because a multichannel electrode array may inadvertently be introduced into the internal canal at the time of implantation.
In summary, the specific terminology used is less important than the detail in which reported cases are described with regard to radiographic and histologic features of each element of the inner ear: specific cochlear morphology, size and relation to the vestibule, patency of the bony modiolus, and the nature of inner ear aqueducts. With adequate patient evaluation and knowledge, clinicians can avoid jumping to conclusions regarding the association of these various clinical features with hearing, implantation outcome, and complications.
Patient Evaluation
Initial radiologic evaluation of the cochlear implant candidate is typically performed with high-resolution CT scanning. Patients with a malformed inner ear or narrow internal auditory canal may undergo supplemental MRI. An MRI of inner ear malformations requires different parameters than those commonly employed in the evaluation of adult hearing loss. The acquisition of appropriate images requires higher resolution and greater-strength magnets.16,17 Intravenous contrast is rarely used. An MRI is obtained in a patient with an inner ear anomaly to identify both the nonosseus partitioning of the malformed cochlea and the neural structures contained within the internal auditory canal (Fig. 7–5). CT and MRI studies are only macroscopic evaluations of the cochleovestibular apparatus; form does not necessarily imply function. Evidence of the existence of a stimulable auditory neural pathway, either by documentation of prior or residual hearing or by utilization of promontory stimulation testing, predicts a more favorable outcome (Figs. 7–6 and 7–7).
A few cochleovestibular anomalies preclude implantation. Complete labyrinthine aplasia would be an absolute contraindication for implantation on the affected side. The determination of cochlear aplasia should involve the careful differentiation from a common cavity deformity by a combination of MRI and promontory stimulation in selected patients to evaluate the possible presence of an adjacent stimulable cochlear nerve ganglion cell population. The failure to identify a cochlear nerve by high-resolution MRI would also contraindicate implantation regardless of the presence of an implantable cavity.
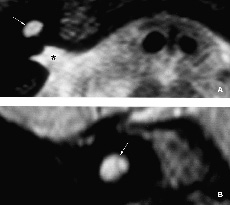
Figure 7–5 T2-weighted MRI demonstrating nonosseous partitioning of a common cavity. These images are from the inner ear shown in Fig. 7–4. (A) Note the bright signal from fluid seen in the internal auditory canal (*) and the cochleovestibular chamber in the axial section. There are low signal intensity septations visible within the common cavity on both the axial (A) and coronal (B) images that are not seen on CT scanning (white arrows).
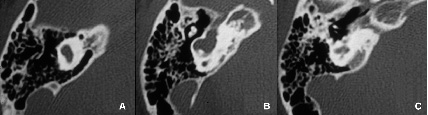
Figure 7–6 Axial CT scan images in another patient with a common cavity deformity. Michel’s aplasia was present on the contralateral side. The sections (A–C) are depicted from superior to inferior. (B) Note the formation of rudimentary semicircular canals. (C) The internal auditory canal becomes apparent. This patient demonstrated some preoperative subjective auditory sensations and language development. Promontory stimulation, as well, indicated the presence of auditory perception. She was successfully implanted with a multichannel device, and currently derives significant benefit from implant use.
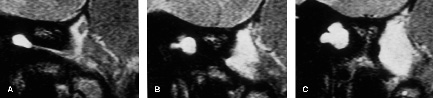
Figure 7–7 T2-weighted coronal MRI of the inner ear depicted in Fig. 7–6, depicted from anterior to posterior. (A) Note the narrow internal auditory canal leading to the fluid containing common cochleovestibular cavity. (B,C) The formation of rudimentary semicircular canals that also contain fluid.
With careful patient selection and preoperative planning, utilization of the various imaging and electrophysiologic testing modalities available, and consultation with experienced device programmers, implantation has been successfully done on many patients with a variety of cochlear malformations.18–25
Is There Evidence of Luminal Obstruction?
In the absence of morphological contraindications to implantation, the next question that must be answered is the following: Is there any evidence of luminal obstruction? Inner ear inflammation, abnormalities of bone metabolism, or trauma may ultimately result in luminal obstruction either by ingrowth of fibrous scar tissue or pathologic neoossification. The etiology that is most commonly encountered, especially in pediatric cochlear implant candidates, is postmeningitic labyrinthitis ossificans. Other postinflammatory causes include suppurative labyrinthitis secondary to otitis media or cholesteatoma, and hematogenous infections (septicemia, mumps, Rubella, or other viral infections). Metabolic bone disorders include otosclerosis and Paget’s disease. Common posttraumatic causes include labyrinthectomy and temporal bone fractures. Wegener’s granulomatosis and autoimmune inner diseases such as Cogan’s syndrome have also been reported to result in labyrinthine ossification.26–29
Bacterial meningitis is the most common cause of acquired severe SNHL in children.30 Some degree of hearing loss has been reported in retrospective analyses to develop in 7 to 29% of survivors of meningitis.31,32 Deafness may follow bacterial meningitis in children in 2 to 7% of cases, with 1.5% being severe and bilateral.30,33 The organisms commonly responsible for postmeningitic deafness are Haemophilus influenzae and Streptococcus pneumoniae. Neisseria meningitidis is also a causative organism, though it is thought to result in a lower incidence of postinfectious deafness.33,34 Though most series report H. influenzae as the leading causative organism in most meningitic deafness, it is of note that a greater proportion of children surviving pneumococcal meningitis (33%) develop hearing loss, as opposed to H. influenzae type b (9%) or meningococcal meningitis (5%).30,32,35 Pneumococcal meningitis that presents a gram-positive exotoxin is additionally associated with severe ossification, whereas the ossification associated with Haemophilus is generally less severe owing to the effects of endotoxins, which may be diminished by corticosteroids.30,33 Some degree of cochlear neo-ossification may be encountered intraoperatively in as high as 70% of patients deafened by meningitis.36 In series including all deafness etiologies, some degree of basal turn cochlear neoossification has been reported in ˜15% of adult patients, and as high as 28 to 35% of pediatric patients.37–39
Pathophysiology of Labyrinthine Ossification
The cochlear aqueduct is a bony channel that connects the subarachnoid space of the posterior cranial fossa to the scala tympani. It opens adjacent to the round window and is lined with a loose network of fibrous tissue termed the “periotic duct,” which is an extension of the arachnoid.40 This is thought to be the site of origin of the inflammatory process into the inner ear in cases of meningitis. Other possible routes include the internal auditory canal and modiolus, the middle ear windows secondary to otitis media, lateral canal fistulization secondary to chronic inflammatory processes, trauma, and hematogenous spread.41,42 When encountered, ossification is nearly always most severe in the region of the round window and proximal scala tympani in the basal turn, adjacent to the opening of the cochlear aqueduct.29 The middle and apical turns are less commonly affected, and the scala vestibuli is often spared.18 Because most cases of labyrinthitis ossificans are partial and the extent of obstruction commonly manifests asymmetrically within an individual patient, preoperative imaging plays an essential role in selecting the side to implant.43 Total cochlear ossification may occur, and is more commonly seen in children than adults.18,44
Cochlear ossification following meningitis is associated with a severe loss of cochlear hair cells as well as a decreased spiral ganglion cell population.45 There is no clearly predictable relationship between the extent of ossification and the number of injured spiral ganglion cells.46 Hinojosa et al47 studied the temporal bones of deaf patients with labyrinthitis ossificans and found that the remaining neuronal cell population ranged from 6310 to 28,196 with a mean of 17,152. This is in comparison to the total cochlear neuronal population of ˜35,500 in the human infant.48 Linthicum et al49 studied the postmortem effects of implants on neuronal population and found that benefit may occur with as few as 3300 neurons. Cochlear ossification does not contraindicate cochlear implantation per se; it does, however, complicate electrode insertion.50
There are several theories regarding the pathogenesis of labyrinthine neo-ossification. Druss51 described in 1936 two types of new bone: metaplastic bone, which originates from ingrown fibrous scar or connective tissue, and osteoplastic bone, which originates from the adjacent otic capsule after disruption of the endosteum. Postlabyrinthitis ossification is thought to occur via the metaplastic process. During the initial acute stage of infection, bacteria within the perilymphatic spaces induce an acute inflammatory reaction characterized by leukocyte infiltration as well as fibroblast proliferation.52 Labyrinthine fibrosis is considered to be the early stage of ossification and may occur within weeks of initial infection.29,52,53 Ossification eventually ensues and this is termed the osseous or late stage of labyrinthitis ossificans. According to Sugiura and Paparella,52,54 undifferentiated mesenchymal cells originating in the endosteum, modiolar spaces, and basilar membrane likely differentiate into fibroblasts and either subsequently or directly into osteoblasts, and form local or diffuse osseous deposits.
Several authors have postulated that the pathogenesis of metaplastic bone formation may be related to disruptions of cochlear blood supply, which has been demonstrated both experimentally and observed histologically in the temporal bones of patients having undergone a variety of surgical procedures.26,55–59 This theory has been claimed to be supported by cell cultures experiments performed by Gorham and Test60 in which low oxygen tension favors bone formation, whereas high oxygen tension favors osteoclastic resorption. Additional investigators have commented on the similar findings between the ossification of vascular occlusion and that of suppurative labyrinthitis.52,54
The two types of neo-ossification were further characterized in histologic studies performed by Kotzias and Linthicum26 on human temporal bones with a variety of pathologic processes including patients who had undergone a variety of neurotologic procedures. The metaplastic form is characterized by high cellularity and the relative absence of eosinophilia. There are no osteoblasts on the surface. Though its margins are indistinct, it is confined to the lumen of the cochlea. The osteoplastic form occurs only when there has been disruption of the endosteum such as occurs during trauma or a surgical defect. It is characterized by less cellularity and increased eosinophilia, and is characteristically lamellar in form, with clear margins and osteoblasts on the surface and not clearly distinct from the endosteal layer.
The postmeningitic neo-ossification is thought to occur via the metaplastic process with the ectopic bone being typically chalky white whereas the native otic capsule bone is generally ivory in hue.36 The difference in color and the neo-ossified bone’s being confined to the lumen of the cochlea aid in differentiating it from the native otic capsule during drilling of the ossified cochlea in the implantation procedure.
Advanced otosclerosis may, in rare cases, cause luminal obstruction that is usually limited to the round window or first few millimeters of the scala tympani.13,26,29 It has been suggested by Kotzias and Linthicum26 that the otosclerotic process may damage the endosteal layer, resulting in the osteoplastic form of neo-ossification. Green et al29 histologically identified foci of otosclerosis within the areas of neo-ossification. All their specimens, as well, demonstrated the pathology to be limited to the first 6 mm of the basal turn in the scala tympani. The pattern of ossification induced by trauma is less predictable.13
Evaluation of Cochlear Patency by Computed Tomography Scanning
Multiple authors have reported discrepancies between the CT scan interpretation of cochlear patency and the findings at implant surgery. This is likely due in part to the thicker image slices available at the time these studies were performed, as well as the early stage of experience of the image interpreters. Early fibro-ossific changes that were not identified on CT scanning are frequently encountered during surgery in postmeningitic patients. This would be especially likely when there is little ossification within the fibrous matrix.31,43,61 The time course for metaplastic ossification is quite variable but is thought to begin with fibrosis as early as 8 days to a few weeks after the initial insult.26,29,52,53,55 The ultimate time frame and extent of eventual osseous deposition is quite variable. It has been reported to be detected as early as 2 months postmeningitis in humans by CT scanning.53 Evidence of ongoing ossification has also been detected to be present histologically in human temporal bones as late as 30 years past the initial insult.29
The reported accuracy of high-resolution CT scan identification of cochlear ossification has ranged from 53% to greater than 90%.13,36,62–64 A review of these studies is useful because they detail the pattern and likelihood of ossification found among various deafness etiologies as well as the potential pitfalls of CT scan interpretation with regard to particular regions of the cochlea. In 1987, Jackler et al63 compared CT scan interpretations with intraoperative findings on 35 cochlear implant patients (17 adults and 18 children) with a variety of deafness etiologies. The group included one adult and seven children deafened by meningitis, making up 23% of the study population. CT scans were performed on a General Electric (GE) 8800 (Fairfield, CT) system with 1.5-mm contiguous axial sections processed using a bone algorithm. Axial scans were taken parallel to the infraorbital-meatal line, and coronal scans were tilted 105 degrees from this plane. The authors reported their CT scan data as either patent or ossified (partial or complete) and detailed the location (round window, basal turn, middle turn, apical turn).
All patients deafened by meningitis had some degree of ossification found at the time of surgery; however, only five of eight had a preoperative CT interpretation suggesting ossification, with the remaining three interpreted as normal. This yielded a 38% false-negative rate among patients deafened by meningitis. However, looking at the specific case data presented, it is apparent that among the three instances of postmeningitic false-negative CT interpretation, two had partial ossification limited to the round window and the third had soft tissue in the round window region, and that all the cases of basal turn involvement were correctly identified by CT.
When all etiologies were considered, there were an additional three false-negative CT interpretations making a total of six of 13, or a 46% false-negative rate. This included one patient with Cogan’s syndrome who had ossification found in the round window and basal turn, and one patient with trauma and basal turn ossification, as well as one patient with prior malignant otitis externa who had undetected complete cochlear soft tissue obliteration. All the children with congenital deafness (10) or ototoxicity (one) and all the adults with progressive familial, viral, syphilis, Meniere’s disease, and unknown etiologies had patent readings on CT scan and no ossification noted at the time of surgery. The effects that these findings had on insertion and outcome is difficult to ascertain as the 18 children in the study were implanted with a House/3M (St. Paul, MN) single-channel device, and no performance data are provided. This is especially true in light of the fact that the great majority of patients today are implanted with long multichannel arrays.
Seicshnaydre et al64 in 1992 compared preoperative CT interpretation with intraoperative findings on 31 children who received a Nucleus multichannel cochlear implant (Cochlear Corporation; Englewood, CO). They reported that scanning was done utilizing a high-resolution bone algorithm with slice thicknesses of 1 to 1.5 mm in the axial and coronal plane. They analyzed their data differently from the previous study. They considered four categories with regard to ossification: normal, narrowed basal turn, bony lip at round window, and ossified cochlea. They also subdivided their cases into postmeningitic and nonmeningitic etiologies. A look at their specific data reveals the difficulty in interpreting the more subtle findings of narrowed basal turn and abnormalities of the round window. Among patient whose CT scans were interpreted as positive for narrowing or the basal turn, 71% were true positives and 29% were false-positive interpretations after confirmation at surgery. Of note is that all the false-positive cases were in nonmeningitic cases. As for abnormalities of the round window, there was an 80% false-positive rate of interpretation in nonmeningitic cases, whereas all the meningitic cases were correctly interpreted.
Seidman et al36 in 1994 performed a retrospective comparison of preoperative CT scan radiologic reports and findings during cochlear implant surgery. CT scans were performed on a GE 9800 system with a slice thickness of 1.5 mm nonoverlapping and utilizing a high-resolution bone algorithm. The authors’ analysis included 32 patients deafened by meningitis. Although 22 (69%) patients were found to have intraoperative evidence of ossification, only seven were properly identified preoperatively. Ten patients were correctly identified as patent, while 15 were falsely identified as patent yielding a 60% (15 of 25) false-negative rate for preoperative CT scan interpretation of cochlear ossification among postmeningitic patients in this study. Interestingly, the authors also reported one false-positive CT interpretation in a patient with osteogenesis imperfecta with a high-resolution CT scan suggesting cochlear otospongiotic changes and luminal occlusion.
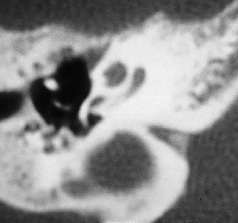
Figure 7–8 CT scan of a patient bilaterally deafened by meningitis demonstrates osseous obstruction limited to the proximal basal turn. Though the middle and apical turns appear patent on CT, further evaluation with MRI is warranted to further assess the possibility of luminal fibrosis. Note that the relationship between the round window and cochlear aqueduct are nicely demonstrated in this section.
Langman and Quigley65 in 1996 reported a sensitivity of 100% and specificity of 86% for the identification of cochlear obstruction using CT scans taken at 1.5-mm contiguous slices on a GE 9800 scanner; however, as the authors pointed out, only 14% of the patients in their study were deafened by meningitis. They did not report data specific to etiology.
In summary, it has been our observation as well as reported in the literature that advances in CT scan technology and radiologist experience have improved the ability to predict luminal obstruction on the basis of CT scan, as current technology allows for the routine acquisition of 1-mm slice thicknesses.13,62 A subset of these patients, particularly those deafened by meningitis, may benefit from MRI to help distinguish the early fibrous phases of labyrinthitis ossificans from a patent fluid-filled lumen, as both may appear gray on CT scans.33,66–68 The evaluation of cochlear patency is initially performed by high-resolution CT scanning. Ossified obstruction can reliably be identified involving the basal segment in isolation or extending distally into the middle and apical turns. Involvement limited to the basal segment on CT may be further evaluated by MRI so that a patent fluid-filled distal lumen may be differentiated from soft tissue obliteration as this may influence surgical planning (Figs. 7–8 to 7–11).
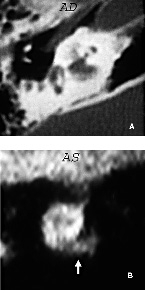
Figure 7–9 (A) This patient bilaterally deafened by meningitis demonstrated osseus obliteration of the cochlea extending into the middle and apical turns on the right side (AD). The left cochlea appeared patent by CT scan; however, the left (AS) coronal MRI (B) demonstrates the presence of intermediate signal within the basal turn (white arrow), which is suggestive of luminal fibrosis.
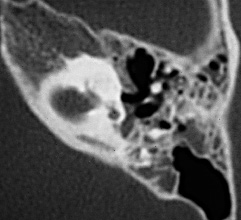
Figure 7–10 CT scan of a patient bilaterally deafened by meningitis demonstrates extensive osseous obliteration involving all turns of the cochlea. The opposite side appeared patent. Note the unusual bulbous appearance of the internal auditory canal, which is demonstrated on the T2-weighted MRI in Fig. 7–11.
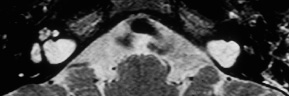
Figure 7–11 MRI of the patient depicted in Fig. 7–10. Note the bilaterally abnormal bulbous morphology of the internal auditory canals as demonstrated by the bright signal from CSF fluid on this T2-weighted image. A bright fluid signal is also present in the lumen of the right cochlea but absent on the left side, which demonstrated extensive osseous obliteration on CT scan.
Are There Additional Findings that May Complicate the Surgery or Subsequent Patient Management?
The initial objectives of preoperative sectional imaging are the determination of cochlear morphology and luminal patency. Additional useful information may be derived that can optimize safety and facility of surgery, as well as influence subsequent patient management. Proper surgical planning must involve careful review of sectional images so that potential complications may be anticipated and properly managed. Preoperative imaging often provides valuable information that would not preclude implantation, but rather helps assess which would be the technically easier ear to implant.
Vascular Anatomy
Aberrant middle ear vascular anatomy that might complicate mastoidectomy and facial recess approach to the cochleostomy may be anticipated by the routine acquisition of preoperative CT scanning. An extreme anterior displacement of the sigmoid sinus with approximation against the posterior canal wall has been reported in 1.6% and a high-riding jugular bulb may be present in 6% of the general population.69 It is rare (though possible) that a jugular bulb or diverticulum may overlie the round window niche or promontory (Fig. 7–12). The distance between the round window and carotid artery may be determined in cases where a drill-out procedure is planned. Abnormal course or dehiscence of the carotid canal may also be detected.
Facial Nerve
Preoperative CT scanning is especially useful in identifying the position of the aberrant facial nerve that may be associated with cochlear malformations. It has been well documented in such cases that the course of the facial nerve may be quite unusual and at increased risk of injury during implantation surgery.18,70,71 By careful preoperative mapping of the course of the facial nerve canal, such patients may be safely and successfully implanted (Fig. 7–13). Careful review of the position of the facial nerve is also warranted as well in patients without cochlear malformations, as there may be dehiscences of the intratympanic portion that may be encountered during the approach to the cochleostomy site.
In some patients with otosclerosis, the presence of spongiotic bone between the apical turn of the cochlea and the pregeniculate facial nerve canal permits unwanted stimulation of the facial nerve during implant use.72 Careful analysis of the CT study helps to anticipate that certain electrodes will require deprogramming (Fig. 7–14).
Mastoid and Tympanic Cavity
The mastoid air cell system and tympanic cavity should also be included in the analysis of preoperative CT studies. The degree of mastoid pneumatization is especially useful information when operating on very young children. Though considered fully developed at birth, the depth of the facial recess as well as its degree of pneumatization may be anticipated.
Radiographic findings in conjunction with clinical severity may be considered in side selection as well as determination of the most appropriate course of therapy for patients with associated chronic ear disease. Chronic ear disease need not be an absolute contraindication for cochlear implantation if carefully selected patients are managed with staged procedures. Traditional canal-wall-up surgery or a more extensive exenteration with a blind sac and oversew type operation can be performed in more severe cases. Subsequent implantation can be performed in a stable, well-protected, well-healed fat-obliterated mastoid cavity.