Pediatric Ophthalmology
Edited by P. F. Gallin
Thieme Medical Publishers, Inc.
New York ©2000

5

Preventions
Trauma remains among the three leading causes of unilateral blindness and vision loss in children.1–3 In particular, for children over 7 years of age, trauma is by far the leading cause of monocular vision loss. If even half of these injuries were prevented, the savings in human suffering, medical costs, and shattered lives would be enormous. They would eclipse any gains that would be made from the eradication of retinoblastoma, congenital glaucoma, and rhabdomyosarcoma. No ophthalmologist will be able to claim the credit from such stupendous scientific advances, yet any ophthalmologist can assist in reducing the incidence of eye injury. Eye safety is the careful application of a few principles to the care of every child. It consists of a message for children, parents, teachers, and civic leaders. The message is simple, the execution complex, but the results are rewarding for patient and practitioner.
 Epidemiology of Pediatric Eye Injury
Epidemiology of Pediatric Eye Injury
There are 2.4 million eye injuries in the United States each year.4 Ten percent of these—240,000— occur in children under 18. Annually, this means that one in every 250 children will sustain an eye injury. Several studies have described the nature and causes of these injuries. The setting is typically in the home for children under 5. A small number of eye injuries in this younger age group occurs as a result of automobile accidents. Children between6 and 18 suffer about half the injuries at home, one quarter at school, one fifth in sports and recreation, and the remainder in miscellaneous settings.
Fortunately, most of the injuries are not vision threatening. They are superficial and heal rapidly, without sequelae. However,it is estimated that 5%— or 14,000 injuries— are potentially blinding injuries.5 The goal of eye safety is to prevent these injuries. It has been proven that up to 90% of such injuries can be prevented with an effective safety program, meaning that 12,000 eyes can be saved each year.
 Eye Safety
Eye Safety
The basic principle of eye safety is the use of appropriate, well-fitted, protective eyewear. The ophthalmologist can have little control over risk-taking behavior, but the use of protective eyewear can succeed in guarding the child from injury. This requires the ophthalmologist to have an understanding of the special needs that arise in prescribing such protective equipment for pediatric patients.
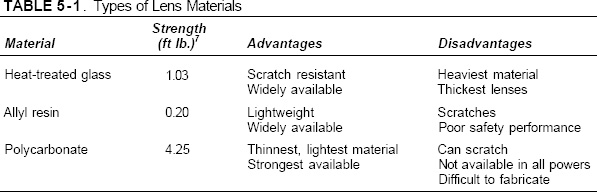
Fashion or dress eyewear comes in one of three materials: heat-treated glass, allyl resin (one brand called CR-39, a trademark of PPG industries), and polycarbonate. Each has advantages and disadvantages described in Table 5-1. In relation to trauma, the ability of the lens to withstand a blow without fracturing is crucial. This strength is measured by dropping a metal ball of fixed weight from varying heights until the lens fails. This is called the drop ball test, and the U.S. Food and Drug Administration (FDA) mandates that dress eyewear withstand up to 0.15 foot pounds of energy before fracturing. To give some sense of the magnitude of force involved, a tennis ball would strike the eye with at least 30 foot pounds of force. The lenses that are ground for street wear usually have a thickness at the center of 2 mm. By comparison, industrial safety lenses usually have a center thickness of 3 mm.
There is no question that polycarbonate lenses can withstand most blows and missiles, even a .22 caliber bullet. However, the use of polycarbonate in street eyewear for children on a routine basis is problematic, given its ease of scratching. Both heat-treated glass and allyl resin exceed the FDA standards for dress eyewear. When used appropriately, they will protect the eye from very low-velocity objects but are totally inappropriate in settings where the eye will be exposed to forces in excess of their fracture strength.Any time there is need to protect the eye in specific high-risk circumstances, it is mandatory that polycarbonate be prescribed. The practitioner who fails to indicate this on a lens prescription for those children who will be exposed to these risks can be successfully sued by the patient. In particular this is the case for one-eyed children, whose situation will be described subsequently. In general, the community standard in most areas is to prescribe one of the three lens materials, unless extenuating circumstances are noted.
 Sport Safety Eyewear
Sport Safety Eyewear
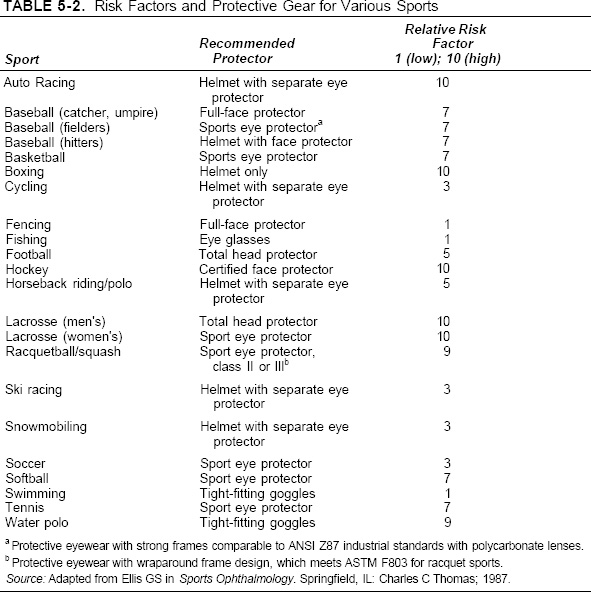
Children enjoy playing a range of sports in both organized and unsupervised leagues. Their frequent risk-taking behavior and athletic immaturity can expose them to even higher risks of injury than those seen in adults. Each sport is unique as to the risk of eye injury, and the necessary protective measures that should be taken. Table 5-2 lists the major sports by risk of injury and appropriate safety eyewear.
The use of eye protection can have a dramatic impact on the reduction of injuries. In Canada, a program to mandate face protection led to the complete elimination of blinding eye injuries.6 This program was the creation of a group of dedicated ophthalmologists who worked with junior hockey leagues to require such equipment. The Hockey Eye Certification Council was formed to assure that equipment would continue to adhere to the standard. This program serves as a model of what can be accomplished in reduction of eye injuries.
 School
School
Children and adolescents spend many hours in school. Risk of injury is particularly great during physical activity and laboratory work. Every lab is required to provide safety eyewear and instruction in its proper use. Goggles are the usual protection used because they can be worn over glasses as well as by children who do not wear glasses. The lenses are made of polycarbonate, and side shields guard against particulate and liquid matter. In sports, the appropriate safety eyewear should be required for all athletes.
 Some Special Circumstances
Some Special Circumstances
Remember that contact lenses do not offer any protection for the eye. Children who wear them should wear safety glasses or goggles over them when exposed to increased risk. The same holds true for any children who may have had refractive surgery. Sunglasses are usually made of heat-treated glass or allyl resin and so have very limited fracture strength. There is a sunglass standard issued by the American National Standards Institute (ANSI Z80). This mandates the degree of transmittance that is acceptable. However, there is no standard for sunglasses to be used in sports. It is recommended that the frame used meets the standard set for industrial use (ANSI Z87) with lenses that transmit less than 1% of UVB and UVA less than 400 nm. Cost of sunglasses will not guarantee that they will meet these standards.
 The One-Eyed Patient
The One-Eyed Patient
Although all children must be protected from eye trauma, those with one functioning eye need particular protection. The definition of a poorly functioning eye is vision corrected to less than 20/40. This was chosen because many states deny driving licenses to those with worse vision.
The American Academies of Ophthalmology and Pediatrics have issued a joint statement for these children, which appears in Appendix 5-1.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


