Endoscopic sphenoidotomy is a common surgical procedure that often accompanies routine sinus surgery. Safe completion of a sphenoidotomy depends on a thorough understanding of the surrounding anatomy, reviewing preoperative imaging, and maintaining intraoperative orientation. Intraoperative complications include local hemorrhage, catastrophic hemorrhage caused by internal carotid injury, optic nerve injury, and CSF leak. Postoperative complications tend to be less severe and include postoperative stenosis and mucocele formation. Regarding surgery of the sphenoid sinuses, the best management of complications truly is prevention, making pre- and intraoperative vigilance vital to a successful outcome.
Chronic rhinosinusitis is a common disorder accounting for an estimated 20 million visits to physician offices in the United States each year. The aggregated cost of sinusitis is approximately $1.8 billion annually, affecting an estimated 16% of the population in the United States. Despite multiple attempted treatments, including an estimated 500,000 surgeries per year, the disease continues to be a major health problem, both in expenditures and poor quality of life. Functional endoscopic sinus surgery is reserved for patients for whom medical therapy including intranasal steroids, systemic steroids, oral antibiotics, oral and intranasal antihistamines, leukotriene inhibitors, and saline irrigation has failed.
When medical therapy fails to treat patients with chronic rhinosinusitis, surgery is indicated. This article discusses surgery of the sphenoid sinus and its complications. The completion of a safe sphenoidotomy depends on familiarity with its anatomy and its related structures and their variations. A careful review of preoperative CT scans and identification of intraoperative landmarks is paramount to a safe and successful operation. Despite detailed analysis of preoperative CT images and meticulous surgical technique, complications can occur.
Complications of sphenoid sinus surgery can be divided into two categories: intraoperative complications and postoperative complications. Intraoperative complications can be devastating and include vascular and neurologic injury, including those that lead to cerebrospinal fluid (CSF) leaks. Postoperative complications are typically less severe and can be considered functional complications leading to poor long-term surgical outcomes. Examples of these complications include epistaxis, ostial stenosis, and delayed mucocele formation.
Anatomy
The paired sphenoid sinuses result from progressive pneumatization of the body of the sphenoid bone, which is situated centrally at the base of the skull. Aeration begins at approximately 3 months gestational age with the invagination of the cartilaginous cupolar recess and progresses through the teenage years.
The sphenoid sinus itself is bounded anterosuperiorly by the sphenoid crest, which articulates with the ethmoid plate and anteroinferiorly by the rostrum, which articulates with the vomer. Lateral to the sphenoid crest are the sphenoid ostia, which measure approximately 2 mm in dimension, are located 10 to 22 mm from the floor of the sphenoid and approximately 7 cm from the anterior nasal spine. Lateral to the rostrum lie the vaginal processes and the pterygopalatine (vidian) foramina. The lateral limit of the sphenoid sinus is variable depending on the extent of pneumatization into the greater wings of the sphenoid bone and pterygoid processes. Typically, the lateral limit of the sphenoid sinus is flush with the cavernous sinus. Pneumatization may extend laterally between the maxillary and vidian nerves, superior to the infratemporal fossa and inferior to the middle cranial fossa. The floor of the sphenoid sinus forms the roof of the nasopharynx and is contiguous with the anterior aspect of the clivus posteroinferiorly.
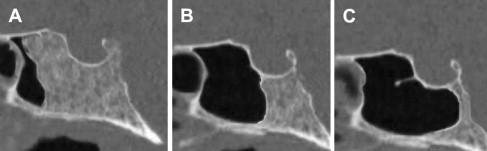
The roof and posterior boundaries of the sphenoid sinus depend largely on a well-described sphenoid bone pneumatization pattern. As originally described by Hamberger, pneumatization of the sphenoid bone is classified as conchal, presellar, or sellar. The conchal pattern is uncommon and defined by absent (or rudimentary) pneumatization of the sphenoid bone. In the presellar pattern, pneumatization extends to the anterior face of the sella turcica, whereas pneumatization extending to the posterior face of the s e lla turcica is defined as sellar pneumatization ( Fig. 1 ). The sellar configuration is the most common pattern and is found in 86% of the population, whereas presellar and conchal pneumatization patterns account for only 11% and 3% of the population, respectively. Other surgeons use a modified version of the Hamberger classification by defining a presellar configuration (anterior to the sella turcica), a sellar configuration (flush with the face of the sella turcica), and a postsellar configuration (pneumatization inferior to the sella turcica). As with Hamberger, pneumatization beyond the limits of the sella turcica is found most frequently. In patients with postsellar pneumatization, the sella forms part of the sphenoid roof, and the remainder is formed by the planum sphenoidale.
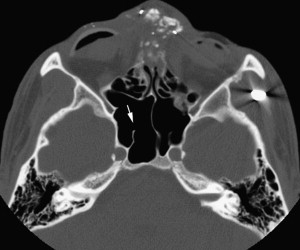
Sphenoid sinus dimensions vary but typically measure approximately 2 cm × 2 cm × 3 cm, with a volume ranging from 5.8 to 7.5 mL. Although paired in nature, the bilateral sphenoid sinuses are infrequently symmetric. The degree of septation within the sphenoid sinus creates this lack of symmetry. A single septum is identified in 20% to 95% of specimens, with accessory septations in 11% to 41%. More importantly, when a single septum is identified, this septation commonly is located off of the midline, indicating that the septum inserts off the midline in most cases (and may mislead the surgeon when identifying the midline). When more septations are present, these septations frequently insert on one or both carotid prominences ( Fig. 2 ) and are oriented in the sagittal plane. Septations that are transverse or horizontal may indicate the presence of a sphenoethmoidal cell (discussed later).
Several neurovascular structures are intimately related to the sphenoid sinus. The largest most important vascular structure is the carotid artery, located medially within the cavernous sinus. The carotid artery indents the lateral wall of the sphenoid sinus in 71% to 98% of cases and may be dehiscent in 4% to 22%. In the superolateral wall of the sphenoid sinus, the optic nerve is identified, typically by a bulge in 8% to 100% of patients, and is dehiscent in 4% to 8%. Together, the optic nerve and the carotid artery form the opticocarotid recess ( Fig. 3 ). Autonomic fibers contained within the pterygopalatine (ie, vidian) nerve run along the lateral floor of the sphenoid sinus within the pterygopalatine canal, inferior and medial to the maxillary nerve (V 2 ), which can be exposed when significant lateral pneumatization of the sphenoid bone is present.
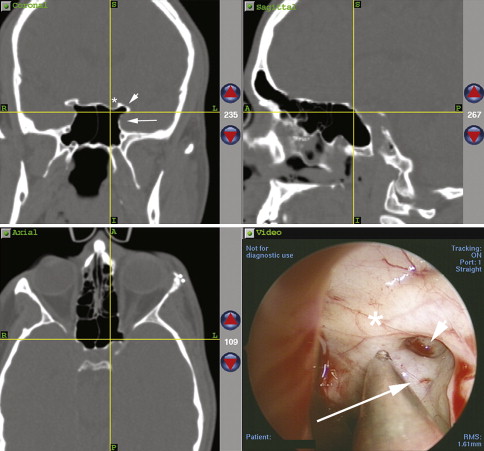
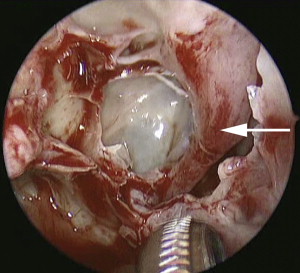
The sphenoid sinus may be related to a sphenoethmoidal (ie, Onodi ) cell, which may be present in 3% to 42% of patients. A sphenoethmoid cell pneumatizes superolaterally to the sphenoid sinus, and can be recognized radiographically by the presence of a horizontal septation within the sphenoid sinus on coronal imaging ( Fig. 4 ). When a sphenoethmoidal cell is present, the optic nerve travels immediately lateral to this ethmoid sinus rather than the sphenoid sinus itself. This anatomic variation places the optic nerve at risk if a sphenoidotomy is performed in a haphazard fashion.

Given the complex anatomy and vital structures surrounding the sphenoid sinuses, great care must be taken when operating within or around the sphenoid sinuses. An in-depth understanding of the regional anatomy lessens the risk for operative complications during sphenoidotomy.
Operative technique
The sphenoid sinus can be safely entered through the posterior ethmoid or the nasal cavity, medial to the superior turbinate. When the sphenoidotomy is performed through the ethmoid route, the superior turbinate is identified after perforating the basal lamella ( Fig. 5 ). Once the superior turbinate is identified, the surgeon is directed toward the sphenoid os, which lies medial to the superior turbinate. A parallelogram is then envisioned, with its boundaries being the skull base superiorly, the lamina papyracea laterally, the septum and superior turbinate medially, and the horizontal portion of the basal lamella inferiorly. The parallelogram is divided superomedially to inferolaterally ( Fig. 6 ).
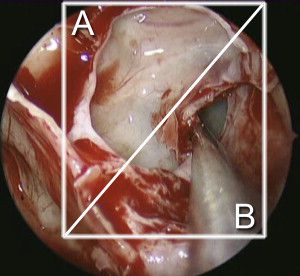
Surgeons generally may safely enter the sphenoid sinus in the inferomedial portion of this “box” without significant risk to the carotid artery or the optic nerve. Entry into a sphenoethmoidal cell may be avoided when using this technique. If difficulty identifying the superior turbinate is encountered, lateralizing the middle turbinate with an elevator and introducing a 0° camera medial to the middle turbinate to locate the sphenoid ostium medial to the superior turbinate is often helpful.
When entering the sphenoid sinus through the transnasal route, the os is usually located 7 cm from the limen nasi and approximately 30° from the nasal floor. A measured beaded probe or stereotactic probes may be used to confirm these distances. If entering the sphenoid from this route, the superior turbinate need not be manipulated further; however, when entering the sphenoid through the ethmoid route, removing the lower third or half using a through-cutting punch typically helps visualize the sphenoid ostium.
Using a curette or suction, the os can usually be cannulated without much difficulty. Bleeding in the region of the os can obstruct visualization. If not performed already, a transoral pterygopalatine fossa injection with 1% lidocaine and 1:100,000 epinephrine may help constrict the sphenopalatine artery and its branches, and additional injection around the septal branch of the sphenopalatine artery may further induce vasoconstriction. Pledgets moistened with 0.05% oxymetazoline or a mixture of 1:1000 epinephrine and 10,000 units of thrombin are also useful to help control bleeding. If bleeding near or on the skull base cannot be controlled with pledgets, cautery may be necessary. Electrocautery should be used with discretion around the sphenoid sinus and, when necessary, bipolar electrocautery should be used, because monopolar cautery can cause inadvertent CSF leak when used close to the skull base.
After the sphenoid sinus is entered through the ostium, it is enlarged superiorly and laterally using a circular sphenoid punch. When opened maximally, the superior limit of the sphenoidotomy is the roof of the sinus, which is an invaluable landmark and particularly useful when clearing posterior ethmoid cells from the skull base. Laterally, the sphenoidotomy can be widened to the lateral wall of the sinus, taking care to note the position of the optic nerve, the presence or absence of a sphenoethmoidal (Onodi ) cell, and the position of the pterygopalatine neurovascular bundle. Aggressive enlargement inferiorly is discouraged to avoid the septal branch of the sphenopalatine artery. Furthermore, the vidian nerve runs along the inferolateral floor of the sinus and could be damaged if the sphenoidotomy is extended too far inferiorly and laterally.
When performing surgery for mild to moderate chronic sinusitis, opening and widening the natural os is typically all that is required. When polyps are present or if inspissated secretions or fungal material may need to be extracted, a larger sphenoidotomy is performed. Instrumentation within the sphenoid sinus, however, is fraught with potential complications and should be avoided.
Operative technique
The sphenoid sinus can be safely entered through the posterior ethmoid or the nasal cavity, medial to the superior turbinate. When the sphenoidotomy is performed through the ethmoid route, the superior turbinate is identified after perforating the basal lamella ( Fig. 5 ). Once the superior turbinate is identified, the surgeon is directed toward the sphenoid os, which lies medial to the superior turbinate. A parallelogram is then envisioned, with its boundaries being the skull base superiorly, the lamina papyracea laterally, the septum and superior turbinate medially, and the horizontal portion of the basal lamella inferiorly. The parallelogram is divided superomedially to inferolaterally ( Fig. 6 ).
Surgeons generally may safely enter the sphenoid sinus in the inferomedial portion of this “box” without significant risk to the carotid artery or the optic nerve. Entry into a sphenoethmoidal cell may be avoided when using this technique. If difficulty identifying the superior turbinate is encountered, lateralizing the middle turbinate with an elevator and introducing a 0° camera medial to the middle turbinate to locate the sphenoid ostium medial to the superior turbinate is often helpful.
When entering the sphenoid sinus through the transnasal route, the os is usually located 7 cm from the limen nasi and approximately 30° from the nasal floor. A measured beaded probe or stereotactic probes may be used to confirm these distances. If entering the sphenoid from this route, the superior turbinate need not be manipulated further; however, when entering the sphenoid through the ethmoid route, removing the lower third or half using a through-cutting punch typically helps visualize the sphenoid ostium.
Using a curette or suction, the os can usually be cannulated without much difficulty. Bleeding in the region of the os can obstruct visualization. If not performed already, a transoral pterygopalatine fossa injection with 1% lidocaine and 1:100,000 epinephrine may help constrict the sphenopalatine artery and its branches, and additional injection around the septal branch of the sphenopalatine artery may further induce vasoconstriction. Pledgets moistened with 0.05% oxymetazoline or a mixture of 1:1000 epinephrine and 10,000 units of thrombin are also useful to help control bleeding. If bleeding near or on the skull base cannot be controlled with pledgets, cautery may be necessary. Electrocautery should be used with discretion around the sphenoid sinus and, when necessary, bipolar electrocautery should be used, because monopolar cautery can cause inadvertent CSF leak when used close to the skull base.
After the sphenoid sinus is entered through the ostium, it is enlarged superiorly and laterally using a circular sphenoid punch. When opened maximally, the superior limit of the sphenoidotomy is the roof of the sinus, which is an invaluable landmark and particularly useful when clearing posterior ethmoid cells from the skull base. Laterally, the sphenoidotomy can be widened to the lateral wall of the sinus, taking care to note the position of the optic nerve, the presence or absence of a sphenoethmoidal (Onodi ) cell, and the position of the pterygopalatine neurovascular bundle. Aggressive enlargement inferiorly is discouraged to avoid the septal branch of the sphenopalatine artery. Furthermore, the vidian nerve runs along the inferolateral floor of the sinus and could be damaged if the sphenoidotomy is extended too far inferiorly and laterally.
When performing surgery for mild to moderate chronic sinusitis, opening and widening the natural os is typically all that is required. When polyps are present or if inspissated secretions or fungal material may need to be extracted, a larger sphenoidotomy is performed. Instrumentation within the sphenoid sinus, however, is fraught with potential complications and should be avoided.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


