Orbital hematoma is an uncommon but serious complication of sinus surgery. Appropriate perioperative attention may minimize risk, but early diagnosis and appropriate management are crucial to preventing vision loss. The surgeon, postoperative care staff, and patient must be aware of the signs and symptoms. Immediate examination must be performed, including pupil size, symmetry, and reactivity, visual acuity, and measurement of intraocular pressure. Immediate consultation from an ophthalmologist or oculoplastic surgeon is mandatory if the diagnosis is suspected. The surgeon and ophthalmologist should follow an algorithm of advancing therapies based on serial examination, ranging from observation only to immediate surgical intervention.
Orbital hematoma is defined as a collection of blood inside the orbit, and the major adverse sequelae that develop arise because the orbit is a bony cone with tight fascial attachments holding the globe at its anterior edge. Therefore, the occurrence of orbital bleeding and hematoma formation can cause the pressure in the globe to increase rapidly, causing damage to sensitive structures inside the orbit. Orbital hematoma is best grouped into categories of spontaneous, traumatic, or iatrogenic. The iatrogenic category is a feared complication of endoscopic sinus surgery (ESS), blepharoplasty, or reconstructive trauma surgery. Awareness, diagnosis, and management of this complication is essential for every head and neck surgeon when operating near or in the orbit. Orbital complications of ESS occur in fewer than 0.4% of cases. Known contributing factors to orbital complications during ESS are surgeon disorientation, bleeding, scarring from prior surgery, and preexisting medial wall abnormality. Some surgeons believe orbital complications occur more frequently on the right side for right-handed surgeons because of the loss of orientation performing surgical dissection towards oneself.
The most commonly described mechanism for orbital hemorrhage during ESS is transection of the anterior ethmoid artery and subsequent retraction of the bleeding artery into the orbit. Increased intraorbital pressure or vasospasm of the central retinal artery then causes blindness from retinal or optic nerve ischemia. Animal models of central retinal artery ischemia suggest that irreversible blindness may occur within 100 minutes. However, clinical reports of permanent blindness have occurred within 1 hour. Early diagnosis and therapy are essential, because permanent sequelae, such as vision loss, are reversible or preventable. This article first reviews the surgical anatomy and strategies for preventing orbital hemorrhage, and then reviews immediate evaluation and treatment strategies for this dreaded complication of ESS.
Surgical anatomy
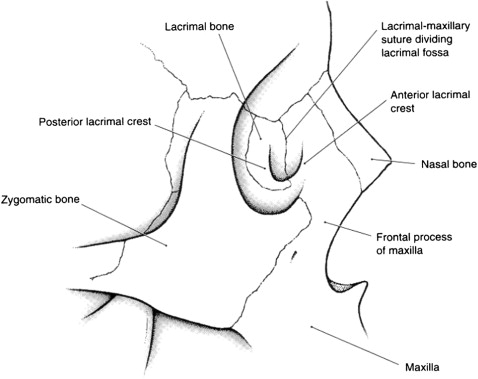
The orbit is a conical shaped cavity roughly 4 x 5 cm in size. Seven bones contribute to the orbit: maxillary, lacrimal, ethmoid, frontal, zygomatic, sphenoid, and palatine ( Fig. 1 ). The thickness of these bones along the orbit is variable, but the medial and inferior walls are the thinnest, less than 1 mm in certain places. Natural dehiscences are uncommon in the medial orbital wall, also known as the lamina papyracea . The orbit is surrounded by bony walls on all sides except anteriorly, where fascial planes hold the globe in position. The globe is supported by the extraocular muscles, which are suspended by several ligaments to the bony orbit. Increased intraorbital pressure therefore causes proptosis, but the amount of globe protrusion is limited by these tendons and ligaments. As pressures approach mean arterial pressure, decreased arterial perfusion of the retina and optic nerve occur, and venous outflow may also be impaired. To release the globe anteriorly for temporary pressure relief, division of the medial or lateral canthal connections is required.
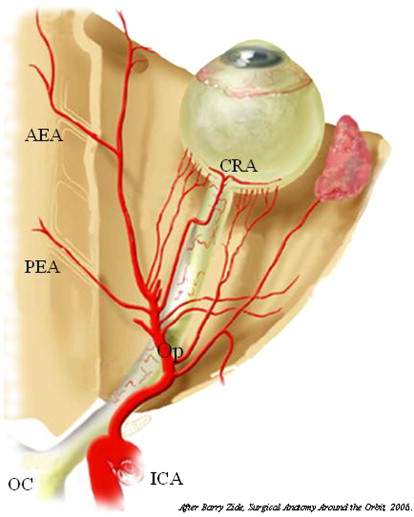
The arterial supply of the orbit and neighboring ethmoid region comes from the internal carotid artery distribution ( Fig. 2 ). The anterior and posterior ethmoid arteries arise from the internal carotid artery through the ophthalmic branch, therefore embolization is not recommended because of the risk for blindness, embolus, and stroke. If needed, these arteries may be ligated through transcutaneous or transconjunctival approaches to the medial orbit. In certain cases, endoscopic transethmoid ligation is possible. The anterior ethmoidal foramen is found on the medial orbital wall 24 mm back from the anterior orbital margin. The posterior ethmoidal foramen is located another 12 mm posteriorly, and the optic foramen another 6 mm posteriorly. The optic foramen typically transmits the ophthalmic artery on the inferolateral aspect of the optic nerve, but it may enter on the inferomedial side in rare cases. When viewed from the lateral aspect, the axial plane containing the anterior and posterior ethmoid arteries corresponds roughly to the level of the skull base. Venous drainage lies within the connective tissue septa of the orbital fat, making extensive fat manipulation at surgery a risk factor for hemorrhage.
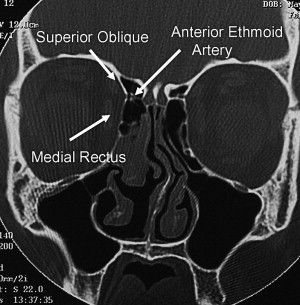
The anterior ethmoid artery is considered the posterior boundary of the frontal recess, and is often encountered in complete ethmoid and frontal dissections. Cadaveric study has shown that 91% of anterior ethmoid arteries are located within the skull base or 1 to 2 mm below, whereas 9% are suspended in a mesentery artery. The precise location of the anterior ethmoid artery can be found on coronal CT scan as a pinch or “nipple” between the medial rectus and superior oblique muscles ( Fig. 3 ). The posterior ethmoid artery travels in a less accessible bony canal just anterior to the sphenoid face.
Prevention
Meticulous perioperative planning is crucial to avoid complication, and prevention of orbital hemorrhage is no different. Optimization of hemostasis and visualization will help avoid entrance into the orbit or injury to the anterior and posterior ethmoid arteries. Preoperative review of patient-specific anatomy should identify the location or presence of (1) the anterior ethmoid artery, (2) the posterior ethmoid artery, (3) medial orbital slope and dehiscence, and (4) atelectasis of the uncinate process ( Fig. 4 ). Image guidance may assist certain cases, but is primarily a tool to verify anatomy. The operating surgeon should never rely solely on the image guidance for dissection. At the onset of the case, the registration accuracy should be checked by comparing it with fixed intranasal anatomy, such as the floor of the nasal cavity, the posterior wall of the maxillary sinus, or the anterior face of the sphenoid.
Certain preferences of surgical technique may also minimize the risk for orbital hemorrhage. For instance, the uncinate process may be safely removed in an anterograde fashion with a sickle knife. However, the blind insertion of the knife into the infundibulum is associated with an inherent risk to the orbit. The authors prefer to remove the uncinate process in a retrograde fashion with backbiting forceps. As the infundibulum is opened and the medial orbit is visualized, the remainder of the uncinate can be removed with a through-cutting forceps. During the subsequent ethmoid dissection, identifying the medial orbital wall early is preferable, rather than avoiding it altogether. In this fashion, the orbit can be followed and protected. This philosophy is similar to that for parotid surgery: better to identify the facial nerve and protect it than to blindly try to avoid the nerve, or in this case the lamina papyracea and the medial orbital wall.
After the skull base is identified in the sphenoid or posterior ethmoid sinus, retrograde dissection along the skull base must be performed with care to identify and preserve the anterior and posterior ethmoid arteries. The posterior ethmoid artery is rarely encountered, but the anterior ethmoid artery is reliably encountered posterior to the frontal recess, and can often be on a pedicle that is easily damaged. Use of through-cutting forceps or a curette along the skull base in these regions can directly injure these arteries. In this setting, bipolar electrocautery is preferred over monopolar cautery for hemostasis to prevent current running through the orbit.
Early detection of violation of the lamina papyracea and possible fat exposure is key to avoiding a more serious complication. In the setting of medial orbital wall dehiscence or fat exposure, the microdebrider should not be used, because rapid debridement of soft tissue (fat, muscle, nerve) can occur ( Fig. 5 ). The suction portion of the microdebrider can pull not only fat but also the medial rectus muscle into the cutting blade. When the lamina is intact, the microdebrider is used with extreme caution along the medial orbit, and the opening of the debrider tip is never turned toward the orbit. Free mucosa, polyps, and thin bony partitions along the orbit are removed with through-cutting forceps or a microdebrider turned perpendicular to the orbit.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


