This article is divided into six sections that are related to six commonly used operations for surgery on the maxillary sinus. The authors discuss maxillary sinoscopy, the Caldwell-Luc procedure, extended middle meatus antrostomy, endoscopic maxillary sinus antrostomy, minimally invasive sinus technique, and balloon sinus procedures. In each of these procedures, the authors discuss potential complications and address prevention and management strategies. Maxillary sinus surgery can greatly improve patients’ symptoms and disease process. The authors encourage the surgeon to take great care in ensuring sound surgical principles. Understanding the potential areas in which surgery can fail will help tremendously in preventing complications.
Maxillary sinus surgery has continued to evolve ever since George Caldwell and Henri Luc described an anterior approach to the maxillary sinus in the late 1800s. Notable changes came in the 1980s with the introduction of endoscopes for use in the paranasal sinuses. The use of angled endoscopes gave the surgeon views of the middle meatus and maxillary ostium that were previously not possible. The development of the coronal bone window for CT scans, introduced in 1987, also gave sinus surgeons a much-needed diagnostic test for the maxillary sinus.
This article is divided into six sections that are related to six commonly used operations for surgery on the maxillary sinus. The authors discuss maxillary sinoscopy, the Caldwell-Luc procedure, extended middle meatus antrostomy, endoscopic maxillary sinus antrostomy, minimally invasive sinus technique, and balloon sinus procedures. In each of these procedures, the authors discuss potential complications ( Table 1 ) and address prevention and management strategies.
| Procedure | Complication |
|---|---|
| Maxillary sinoscopy | Pain, facial swelling, dental numbness, facial numbness |
| Caldwell-Luc | Pain, facial swelling, dental numbness, facial numbness, facial asymmetry, oroantral fistula, gingival-labial wound dehiscence, dacryocystitis, devitalized tooth, bleeding, persistent sinusitis |
| Extended middle meatus antrostomy | Chronic crusting, empty nose syndrome, circular flow around stump, injury to nasolacrimal duct |
| Endoscopic middle meatus antrostomy | Missed natural os, scarring, injury to nasolacrimal duct-epiphora, orbital penetration, facial numbness |
| Balloon dilatation (Acclarent) | Missed natural os, submucosal passage of balloon, orbital penetration |
| Balloon dilation (Entellus) | Pain, facial swelling, dental numbness, facial numbness, failure to pass balloon catheter |
| Minimally invasive sinus technique | Missed natural os, scarring, circular flow |
Maxillary sinoscopy
Maxillary sinoscopy is a surgical technique that allows the surgeon to look inside the maxillary sinus with a telescope and to treat the diseased anterior half of the maxillary sinus. This procedure is often performed in association with an endoscopic endonasal middle meatal approach. For the sinoscopy, the surgeon uses an endoscopic trocar to traverse the canine fossa into the maxillary sinus. During this approach, branches of the infraorbital and anterior superior alveolar nerve (ASAN) may be harmed because of their proximity to the canine fossa. Resultant complications from injury to these nerves include facial pain, dental numbness, and local hypoesthesia. Other notable complications of the sinoscopy procedure include facial swelling and cellulitis.
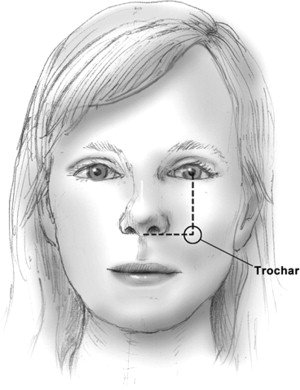
Robinson and Wormald described an ideal point of anterior entry into the sinus at the intersection of the mid-pupillary line and the horizontal line through the floor of the nasal vestibule. Fig. 1 depicts this point. Once this landmark is identified, a trocar is twisted to remove bone of the anterior wall of the maxillary sinus. The trocar should not be hammered into the sinus because of the possibility of fracture of the anterior wall through the branches of the infraorbital nerve and ASAN with resultant facial numbness. Careful attention to these guidelines will diminish the risk for dental numbness and facial hypoesthesia. To decrease postoperative facial emphysema, patients should be instructed to not blow their nose for 24 hours after surgery. Pre- and postoperative antibiotics should also be considered to prevent facial cellulitis as a consequence of dragging the trocar through the facial soft tissues. In the authors’ experience, placing ice over the cheek area postoperatively has reduced the bruising and swelling often associated with this approach.
Caldwell-Luc
Until the mid 1980s, the Caldwell-Luc operation was the main operation used to manage maxillary sinus disease. Currently, it is rare for the sinus surgeon to resort to the Caldwell-Luc operation. The Caldwell-Luc operation is, however, the authors’ mainstay of surgical treatment for failed middle meatus antrostomy maxillary sinus disease. This procedure is the authors’ last-resort operation after exhausting surgical and medical treatments of the diseased sinus, including revision antrostomies, biofilm management, use of culture-directed antibiotics, nasal irrigations, systemic steroids, multiple office debridements, and intravenous antibiotics on occasion. When patients state that they are tired of all the treatment, it becomes time to look at other options: the authors offer Caldwell-Luc at this point.
This procedure has been noted to have varying rates of complication and morbidity in the literature. Cutler and Duncavage reviewed 133 Caldwell-Luc procedures with a follow-up of 1 to 6 years. They found a 92% success rate with an average follow-up of 23.5 months. The most common risk for the Caldwell-Luc procedure is the failure of the surgery to cure the infection. Eight percent (n = 3) of subjects in this review did not respond to the surgery. In two of these three cases, failure was caused by trapped mucosa and these cases were successfully salvaged with a repeat Caldwell-Luc procedure. Mild postoperative discomfort was reported in 37% and facial numbness or deformity was identified in 2%. Defreitas and Lucente published the largest, single institutional review of 670 cases of the Caldwell-Luc operation in 1988. The immediate postoperative complications in 522 subjects were facial swelling in 89% of subjects, cheek discomfort in 33% of subjects, temperature more than 101°F in 12% of subjects, and significant hemorrhage in 3% of subjects. They reported long-term complications of facial asymmetry in 0.7% of subjects, facial numbness or paresthesia in 9.0% of subjects, oral antral fistula in 1.0% of subjects, gingival-labial wound dehiscence in 1.0% of subjects, dacryocystitis in 2.0% of subjects, devitalized dentition in 0.4% of subjects, recurrent sinusitis in 12.0% of subjects, and recurrent polyposis in 5.0% of subjects.
How do we prevent the previously mentioned complications? The authors recommend using the previously described anatomic landmarks for entry into the maxillary sinus to minimize injury to branches of the infraorbital nerve and ASAN. By twisting the trocar through the canine fossa, one can avoid fracture of surrounding bone. Care must also be taken when elevating the periosteum to avoid injury to the adjacent nerves. The authors do not extend the bone removal lateral to the point of entry to protect the lateral maxillary buttress and to minimize potential facial asymmetry. Bleeding is minimized by the use of the topical clotting agents and, at the end of the procedure, the sinus is filled with hemostatic agents, such as Surgifoam (Ethicon, Inc, Somerville, NJ, USA).
To avoid an oroantral fistula, the authors perform an inferior meatal antrostomy at the time of the Caldwell-Luc procedure to assist with sinus drainage. The placement of this antrostomy is important to not injure the valve of Hasner, and should be directed in the posterior two thirds of the inferior meatus. Patients are seen postoperatively at 1 week to remove and debride crusts that block the middle meatus, which seems to help with postoperative pain and pressure over the maxillary sinus. Wound dehiscence is prevented by closure with absorbable suture using a running, non-locking, horizontal mattress closure.
Caldwell-Luc
Until the mid 1980s, the Caldwell-Luc operation was the main operation used to manage maxillary sinus disease. Currently, it is rare for the sinus surgeon to resort to the Caldwell-Luc operation. The Caldwell-Luc operation is, however, the authors’ mainstay of surgical treatment for failed middle meatus antrostomy maxillary sinus disease. This procedure is the authors’ last-resort operation after exhausting surgical and medical treatments of the diseased sinus, including revision antrostomies, biofilm management, use of culture-directed antibiotics, nasal irrigations, systemic steroids, multiple office debridements, and intravenous antibiotics on occasion. When patients state that they are tired of all the treatment, it becomes time to look at other options: the authors offer Caldwell-Luc at this point.
This procedure has been noted to have varying rates of complication and morbidity in the literature. Cutler and Duncavage reviewed 133 Caldwell-Luc procedures with a follow-up of 1 to 6 years. They found a 92% success rate with an average follow-up of 23.5 months. The most common risk for the Caldwell-Luc procedure is the failure of the surgery to cure the infection. Eight percent (n = 3) of subjects in this review did not respond to the surgery. In two of these three cases, failure was caused by trapped mucosa and these cases were successfully salvaged with a repeat Caldwell-Luc procedure. Mild postoperative discomfort was reported in 37% and facial numbness or deformity was identified in 2%. Defreitas and Lucente published the largest, single institutional review of 670 cases of the Caldwell-Luc operation in 1988. The immediate postoperative complications in 522 subjects were facial swelling in 89% of subjects, cheek discomfort in 33% of subjects, temperature more than 101°F in 12% of subjects, and significant hemorrhage in 3% of subjects. They reported long-term complications of facial asymmetry in 0.7% of subjects, facial numbness or paresthesia in 9.0% of subjects, oral antral fistula in 1.0% of subjects, gingival-labial wound dehiscence in 1.0% of subjects, dacryocystitis in 2.0% of subjects, devitalized dentition in 0.4% of subjects, recurrent sinusitis in 12.0% of subjects, and recurrent polyposis in 5.0% of subjects.
How do we prevent the previously mentioned complications? The authors recommend using the previously described anatomic landmarks for entry into the maxillary sinus to minimize injury to branches of the infraorbital nerve and ASAN. By twisting the trocar through the canine fossa, one can avoid fracture of surrounding bone. Care must also be taken when elevating the periosteum to avoid injury to the adjacent nerves. The authors do not extend the bone removal lateral to the point of entry to protect the lateral maxillary buttress and to minimize potential facial asymmetry. Bleeding is minimized by the use of the topical clotting agents and, at the end of the procedure, the sinus is filled with hemostatic agents, such as Surgifoam (Ethicon, Inc, Somerville, NJ, USA).
To avoid an oroantral fistula, the authors perform an inferior meatal antrostomy at the time of the Caldwell-Luc procedure to assist with sinus drainage. The placement of this antrostomy is important to not injure the valve of Hasner, and should be directed in the posterior two thirds of the inferior meatus. Patients are seen postoperatively at 1 week to remove and debride crusts that block the middle meatus, which seems to help with postoperative pain and pressure over the maxillary sinus. Wound dehiscence is prevented by closure with absorbable suture using a running, non-locking, horizontal mattress closure.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


