Frontal sinus surgery continues to remain one of the most challenging areas for sinus surgeons. Many different techniques have been introduced for dealing with the frontal sinus. These can range from conservative, mucus membrane–preserving, strictly endoscopic techniques to radical endoscopic and open procedures using drills and burrs to create large openings, all with the aim of keeping the frontal sinus aerated, disease free, and functional in the long-term. This article deals not only with ways in which surgical techniques can be used to minimize or prevent complications in this difficult area but also on how to deal with complications when they occur.
Prevention of complications in frontal sinus surgery
The frontal sinus remains one of the most complex regions to operate on, with a wide array of anatomic variations between patients and even between 2 sides in the same patient. The frontal sinus surgeon needs to be extremely learned in the different anatomic challenges that may present during surgery in this area. There is no substitute for knowing the anatomy of this region in detail. Performing an adequate functional frontal sinusotomy while minimizing the risk of a complication requires proper planning that starts before the patient enters the operating room.
Preoperative Planning
Computed tomography scan review
A critical preoperative review of the computed tomography (CT) scan is vital and must be performed by the operating surgeon once a decision for surgery has been made. The frontal sinus anatomy should be reviewed on a triplanar imaging system if possible, so that sagittal, coronal, and axial cuts are visualized simultaneously. The presence or absence of cells that may potentially obstruct the frontal recess (frontal cells, intersinusseptal cells, supraorbital ethmoid cells, and so forth), upper attachment of the uncinate process, and the various possible variations of the anatomy need to be identified. It is important that the operating surgeon can mentally create a three-dimensional image of the drainage pathway. Some investigators have recommended creating square line and cube like patterns to imitate the drainage pathway. Such an exercise can be helpful for the novice frontal sinus surgeon so that they can be prepared for what might happen during the surgical dissection.
Preoperative medications
It is important to prime the mucus membrane so that it is in the best possible condition during the operation as it is difficult to operate on an inflamed frontal recess. The presence of inflammation results in increased intraoperative bleeding which, in turn, makes endoscopic exposure difficult. Any medication that may reduce the inflammation in the frontal recess results in a decreased amount of bleeding.
Antibiotics
Most sinus cavities are being operated on because they are chronically infected and inflamed. A preoperative antibiotic decreases the amount of inflammation and likely results in a cleaner field with a decreased amount of blood loss. Most of our patients being taken to the operating room for an endoscopic frontal sinusotomy are placed on a 7-day course of antibiotics preoperatively and a 7-day course of antibiotic postoperatively while any spacers or splints are in place.
Prednisone
Prednisone is a strong antiinflammatory medication and is also used to reduce the inflammation in a chronically infected and inflamed sinus cavity preoperatively. Patients who do not have a contraindication to oral steroids are started on 0.2 mg/kg of prednisone daily starting 7 days before surgery reducing to 0.1 mg/kg of prednisone daily for 7 days after surgery during the initial healing phase. This has been found to reduce bleeding intraoperatively likely secondary to the reduction in the inflammation of the tissues being operated on. The secondary gain for a significant number of patients is an improvement in their lung function preoperatively, which makes administration of their anesthesia easier and better tolerated.
Topical decongestant
Further preoperative preparation of the nasal cavity and mucus membrane is performed by instructing the patient to spray their nose with a topical decongestant (xylometazoline) starting 2 hours before surgery and every 30 minutes thereafter until the patient is wheeled into the operating room. This has a very effective decongestant effect on the mucus membrane of the nose before the operation allowing for an optimal surgical field. This is further enhanced by gently packing the nasal cavity with neuropatties lightly soaked with a topical decongestant (xylometazoline) as soon as the patient has been intubated and before the patient is draped. This results in a wide-open, well-decongested nasal cavity as the operation begins.
Intraoperative Planning
Blood pressure monitoring
We have found that keeping the systolic blood pressure less than 100 mm Hg reduces the amount of blood loss and improves visualization during surgery. We do not inject the lateral nasal wall or the nasal cavity with local anesthetic/epinephrine before beginning the operation. A recently published study from our center showed that injecting the lateral nasal wall with a xylocaine/epinephrine combination at the start of the operation actually increased the amount of blood loss during the operation. We recommend that the nasal cavity not be injected with local anesthetic/epinephrine combination at the start of the operation as long as the patient has been properly prepared for surgery as described earlier. We also recommend against using topical cocaine or topical epinephrine in the nasal or sinus cavity before or during the operation because of concerns regarding the potential for increased cardiovascular complications.
Extent of surgery
It is important to determine the extent of surgery that is necessary before beginning the operation. If the disease is confined strictly to the frontal sinus, then the surgeon may carry out an ethmoid bulla-intact frontal sinusotomy and not disturb the ethmoid cells. On the other hand, if the anterior (and posterior) ethmoid cells are involved, then it is important to complete the ethmoidectomy before focusing on the frontal recess. In such a situation, the surgeon should not start working on the frontal recess before the ethmoidectomy has been completed. Leaving behind shelves at the skull base and starting the frontal sinusotomy with an incomplete ethmoidectomy compromises visualization and access to the frontal recess as well as promoting future scarring.
Approaching the frontal recess
Once the ethmoidectomy is completed, the frontal recess should be approached from a posterior to anterior direction along the skull base. It is important to use through-cutting instrumentation when removing the ethmoid bulla lamellae and other vertical shelves during the approach to the frontal recess. Meticulous preservation of the mucus membrane is important to avoid creating areas of bare bone and therefore the future potential of osteoneogenesis and subsequent iatrogenic scarring that can occur in the frontal recess. If a large, pneumatized agger nasi cell is encountered, it is important to try and identify the posterior or medial edge of the shelf. This allows the surgeon to carefully remove the agger nasi cap in a systematic manner while preserving the mucus membrane within the frontal recess. It is important that the surgeon, with the help of a tridimensional CT scan, creates an imaginary three-dimensional picture of the frontal recess and associated cells in their head. If an image guidance system is being used during the operation, it should simply be used as a guide and not as a final acceptance of the anatomy. The surgeon’s own knowledge and instinct should be the most important guide in working on the frontal recess.
It is important to move the instruments from posterior to anterior or from medial to lateral. This reduces the likelihood of mistakenly entering the intracranial cavity. The lateral cribriform plate lamellae can be very thin in the region of the frontal recess where the anterior ethmoid artery crosses the skull base. Using sharp instruments in a rough manner at the level of the anterior ethmoid artery can result in a cerebrospinal fluid (CSF) leak or bleeding from the anterior ethmoid artery. It is also important to identify the anterior ethmoid artery on the CT scan and recognize how low it sits in the skull base so that it is not transected or traumatized during the dissection. Entry into the orbit is difficult because the orbital bone or laminae papyracea is not as thin in the region of the frontal recess as it is in the region of the lacrimal sac or ethmoid region. In rare cases the bone over the orbit can be dehiscent. In such cases it is extremely important to be aware of the dehiscence and to avoid using a powered instrument or microdebrider near the dehiscent area.
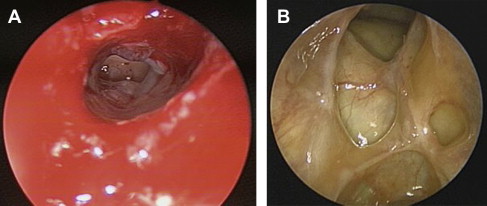
At the completion of the endoscopic frontal sinusotomy, the endoscopic surgeon should be able to see a nicely opened internal frontal sinus ostium with well-preserved circumferential mucus membrane. This allows for a well-healed successfully functioning frontal sinus ( Fig. 1 ).
Use of powered instrumentation in the frontal recess
At the St Paul’s Sinus Center, use of powered instrumentation in the frontal recess is generally avoided. All dissection is performed with 30° or 70° endoscopes complemented with 45° and 90° giraffe forceps and through-cut instruments with meticulous mucus membrane preservation. Advances in angled instrumentation have allowed the frontal sinus surgeons to reach into the frontal recess and sinus at angles previously believed to be unreachable ( Fig. 2 ). This has allowed for greater endoscopic success for frontal sinus surgery that previously would have seemed unoperable via an endoscopic-only route.

Powered instrumentation and drilling in the frontal recess can result in bare bone within the frontal recess and ostium. This can lead to scarring and osteoneogenesis with subsequent failure of the frontal sinus from staying open. Use of powered instrumentation in the frontal recess should therefore be avoided as much as possible. A recent, yet unpublished, study of 200 patients at our institution who had undergone endoscopic frontal sinusotomy showed the success rate of endoscopic sinus surgery in a previously unoperated patient was in the 90% plus range. Only 8% of patients in the primary group required a return to the operating room compared with 21% in the group undergoing a revision frontal dissection. Revision surgery, as one would expect, results in a higher failure rate simply from an increased risk of scarring. A modified Lothrop procedure is therefore never indicated for a primary operation in the frontal sinus regardless of how bad the inflammatory disease is in the frontal recess/sinus.
Sinus packing
A middle meatal spacer made out of a downsized merocel sponge placed inside a glove finger is placed within the middle meatus. The objective of the spacer is to allow the middle meatus to stay patent and free of clots. It also allows the middle turbinate to stay medialized during the early healing process. The spacer is removed at the first postoperative visit between 5 and 7 days after surgery. We are currently investigating medicated merocel sponges as spacers in the early postoperative period, but it is too early to make any conclusive comments.
Postoperative Planning
Postoperative irrigation
Patients are instructed to start irrigating their nasal/sinus cavities 3 times a day with saline starting on the first postoperative day. This allows for autodebridement of the nasal cavity washing out all clots and fibrin debris. After the first visit at 6 days postoperatively, irrigation is reduced to once a day for the next 6 to 12 weeks. We have found that heavy irrigation (more than once a day) after the first 2 weeks can actually result in significant discomfort for the patient.
Postoperative medication
All patients are started on a 7-day course of prednisone at 0.1 mg /kg and antibiotics. This keeps the early postoperative inflammation under control while the sinuses are actively draining mucus and blood clots. If the patient has met the criteria for a diagnosis of allergic fungal sinusitis, then the patient is instructed to place 2 mL of budesonide (0.5 mg/2 mL) into 240 mL of isotonic saline for irrigation of the sinonasal cavity twice a day.
Postoperative visits
Patients are seen at 6 days postoperatively (5 to 7 days) at which time the middle meatal spacers are removed and the sinus cavities are very gently suctioned free of clots and mucus. It is important to avoid creating new bleeding in the frontal recess at this visit because this will obscure the surgeons view and create further clotting. Leaving clots behind in the frontal recess risks the formation of fibrin and therefore scarring, and increases the risk of infection. The frontal recess and sinus are visualized with a pediatric 45° or 70° scope to ensure patency and absence of infection. Any evidence of purulence results in cultures being taken and the sinuses being lavaged with saline using double curved suctions or Van Alyea cannulas, followed by placement of a topical steroid and antibiotic mixture within the affected sinus cavity.
The second and third visits are planned depending on what the cavity looks like at the first visit. In most cases, if all looks well, the second visit is at 4 weeks postoperatively and the third visit at 12 weeks postoperatively at which point the sinuses are usually well healed and patent as shown in Fig. 1 B. The frontal recess and ostium are visualized at each visit and if needed the frontal sinus is lavaged with saline. If edema is identified within the recess or sinus, a mixture of gentamycin and a topical nasal steroid is placed within the sinus with the patient in a dependent position. If scar bands or remnant slivers of bone are seen within the frontal recess during the first few visits, they are removed in the clinic under local anesthesia.
Complications in frontal sinus surgery
Several major intraoperative complications can occur during frontal sinus surgery depending on the approach used (endoscopic vs external). Although, these different types of approaches may share some of the general complications (eg, bleeding and CSF leak), each technique can also have specific complications related to it. These can be broadly divided into 2 categories
- (1)
Transnasal endoscopic procedures:
- •
Endoscopic frontal sinusotomy
- •
Modified endoscopic Lothrop procedure (MEL).
- •
- (2)
External procedures:
- •
Frontal sinus trephine
- •
Osteoplastic flap with/without obliteration
- •
Frontal sinus cranialization
- •
- •
Combined above and below approaches (external plus endoscopic).
The complications from each type of surgical technique can be further subdivided into intraoperative complications and early and late postoperative complications.
Endoscopic Frontal Sinusotomy Complications
- (1)
Entry into the orbit
- (2)
Excessive bleeding from transection of the anterior ethmoid artery
- (3)
Intracranial entry
- (4)
Excessive denudation of the mucosal membrane.
Managing Complications
Orbital entry
Orbital entry can range from simple orbital fat exposure to intraorbital hemorrhage to actual damage to the intraorbital muscles with powered instrumentation. Analysis of the preoperative CT scan to identify any areas of dehiscence of the lamina papyracea should be performed before surgery. Exposure of the periorbita can usually be identified endoscopically and confirmed by palpation of the orbit with associated movement of the periorbita. If the periorbita has been violated and fat exposed, it should be immediately recognized and the use of any suction and/or powered instrumentation in the area should be strictly avoided. The area of orbital fat exposure should be covered with a small piece of silastic or epifilm (Medtronic Xomed) and, if there is adequate space around it, the operation can be carefully completed. Once surgery is complete, the exposed area should be covered with a small piece of epifilm. On the other hand, if there is a major orbital complication (ie, intraorbital hemorrhage from a retracted and resected anterior ethmoid artery), then the surgeon should be prepared to carry out a lateral canthotomy and cantholysis and follow the protocol outlined in the next section.
A medial rectus muscle injury caused by suction-assisted powered instruments (debriders) is considered the most devastating complication from sinus surgery. The resulting diplopia is permanent and devastating to the patient’s quality of life and its treatment is seldom successful. When it does occur, immediate ophthalmology consultation should be obtained ( Fig. 3 ).

Hemorrhage from anterior ethmoid artery
If the anterior ethmoid artery is low lying in the skull base, it can easily be damaged with through-cut instruments or the debrider during approach to the frontal sinus. It is therefore extremely important for the operating surgeon to have critically analyzed the preoperative CT scan to determine the position of the anterior ethmoid artery, the presence or absence of bone over the artery, the possible presence of more than 1 branch, and any other oddities in the anatomy of the artery before attempting surgery in the frontal recess. A partial transection of the artery can result in a significant amount of bleeding but as long as the artery does not retract into the orbital cavity there is no significant danger posed to the patient’s vision. A bipolar or unipolar suction cautery can be used to cauterize and control the bleeding vessel.
Complete transection of the anterior ethmoid artery may result in retraction of the artery. Retraction into the orbit may produce the rapid onset of an orbital hematoma. Orbital hematomas may be either arterial or venous in origin. Arterial bleeds are of rapid onset and usually present with intraoperative proptosis. The globe usually becomes rock hard within seconds to minutes. The most important factor in managing these patients is maintaining or restoring blood flow to the optic nerve, thereby preventing visual compromise. Because vision cannot be assessed while the patient is under a general anesthetic, decisions on hematoma management must be made as if the least favorable outcome is likely. Ophthalmology assistance should be sought immediately. In reality, immediate ophthalmologic assistance may not always be available or the ophthalmologist may have limited expertise in orbital surgery. In such situations, the patient relies on the judgment and skills of the otolaryngologist. Surgical and medical management should commence immediately because ischemia time to the optic nerve is an essential factor. A lateral canthotomy with upper and/or lower cantholysis is indicated and should be performed immediately. This immediately increases orbital volume and decreases orbital pressure thereby allowing blood flow to the optic nerve once again. Simultaneous medical management includes intravenous mannitol (1 g/kg intravenously), which also decreases intraorbital pressure. The use of intravenous steroids in such a situation remains unproven and controversial. If the intraorbital pressure does not decrease despite these measures, endoscopic orbital decompression with removal of lamina papyracea should be considered.
Orbital hematomas as a result of a venous bleed usually occur in the postoperative period and present as a slowly progressive proptosis and visual loss. The patient’s vision should be closely assessed, especially the color vision, because it is first to deteriorate. If the vision is within normal limits and the proptosis is mild, the patient should be observed very closely. Any nasal/sinus packing on the ipsilateral side should be removed. Orbital massage has been suggested in the literature to redistribute the blood clot within the orbit; we do not recommend this technique at our center. Ophthalmology should be consulted to assess vision, do a fundoscopy, as well as measure intraocular pressure. Medical management, including mannitol, may be started if the situation continues to worsen. If the patient’s vision starts deteriorating, then surgical intervention should be performed as discussed earlier.
Intracranial entry/CSF leak
If intracranial entry and a resulting CSF leak occurs, it should be recognized and dealt with immediately. The violated region of the skull base should be cleared of any sinus disease and the site of entry prepared for repair. Site preparation is the most important aspect for successfully repairing a CSF leak. The immediate area around the defect should be denuded of mucus membrane as a first step in the repair. Depending on the skull base defect and the skill of the surgeon, a variety of underlay and overlay options using autograft and allograft material can be used for the repair. At our institution, a 2- to 3-layer repair using septal bone, temporalis fascia, and a mucosal membrane graft is usually used and has been found to be very successful. A lumbar drain is not required if the repair is performed immediately. The sinus operation can then be continued and completed in the usual manner. Support to the repair site is essential. A merocel sponge in a finger glove cot is placed against the repair site for the first 7 days. Another sponge may be placed under the first one to create snug support for the repair site. During this time the patient is given oral antibiotics and advised on the importance of minimal activity and reduced physical stressors.
The only exception to not repairing the defect intraoperatively is if the surgeon remains anatomically disoriented. In such a case, any attempt at surgical repair could result in further complications, such as brain parenchymal injury or orbital injury. It is recommended that the patient be transferred to the nearest tertiary sinus center where a properly trained team can complete the repair.
If the CSF leak is not diagnosed until the postoperative period, the patient usually presents with unilateral rhinorrhea. If not identified early, the patient may suffer from serious sequelae, including meningitis, pneumocephalus, and possibly coma or death. All patients suspicious of having a CSF leak should have the secretions tested for β2-transferrin. Once a CSF leak is confirmed, investigation to seek the exact site of the leak should be sought. High-resolution, fine-cut coronal CT scan of the sinuses is performed. A search for bony defects in the area of previous surgery is attempted. The most common location for an iatrogenic CSF leak is the lateral lamella of the cribiform plate where the anterior ethmoid artery enters the intracranial cavity. Special attention should be given to opacification or air fluid levels within sinuses that may give a clue to a leak in the area.
If the site of the leak is not apparent on CT, then a magnetic resonance cisternogram should be performed. It is a highly sensitive and specific test if done when the patient is actively leaking and will identify any CSF that has pooled within the sinuses. All patients with suspected meningoceles or meningoencephaloceles should undergo magnetic resonance imaging to confirm the diagnosis and for proper management.
We usually use pre- or intraoperative placement of a lumbar drain and intrathecal fluorescein for patients undergoing a CSF leak repair. Because intravenous fluorescein is not approved for intrathecal use, a separate consent designed specifically for this purpose is obtained. A lumbar puncture and placement of drain is performed while the patient is awake. Ten milliliters of CSF are removed and mixed with 0.1 mL of 10% intravenous fluorescein using a tuberculin syringe. The mixture is then re-injected into the intrathecal space at a rate of 1 mL per minute (ie, 10 minutes). Potential risks of intrathecal fluorescein injection include parasthesias and convulsions. These side effects have been reported in the past but with much higher doses of fluorescein than used currently. The fluorescein stains the CSF a fluorescent yellow-green color allowing precise confirmation of the leak site. A blue light filter placed on the light source helps to identify the presence of fluorescein even in very small quantities. If the leak is not visible, the patient may be placed in a head down position and the anesthesiologist may perform a valsalva maneuver. Once the site of the leak is identified, the repair process is similar to that described earlier for CSF leaks diagnosed intraoperatively.
Bone denudation of mucus membrane
If the mucus membrane is inadvertently damaged/removed during the dissection in the frontal recess, the risk of osteoneogenesis and scarring of the frontal recess increases significantly. This requires that the surgeon be very careful when dissecting in the frontal recess/sinus region. If an area of denudation does occur and it is in the region of the frontal sinus ostium, a free mucosal membrane graft can be considered to cover the area and thereby avoid osteoneogenesis and scar formation. If it is not possible to cover the denuded area then the denuded area should be washed out with an antibiotic/steroid gel at the end of the operation and watched carefully during the postoperative period.
MEL Procedure Complications
The MEL procedure is a more extensive form of endoscopic frontal sinusotomy with loss of mucus membrane in a critical area with the possibility of significant potential complications. Re-stenosis of the frontal recess secondary to denudation of the bone from this procedure continues to remain high. Long-term patency and re-stenosis is the most concerning complication and has received a good deal of attention. The drilling in the agger and anterior buttress region destroys the lateral frontal recess mucous membrane. This particular mucous membrane carries the ciliary mucous transport mechanism for exit out of the frontal sinus. Destruction of this important mucus membrane puts the frontal sinus at risk for mucociliary clearance failure, neoosteogenesis, and re-stenosis ( Fig. 4 ). Denuded bone results in the formation of crusting, chronic infections, and persistent symptoms. Wormald showed that 21 out of the 83 patients who had MEL procedures continued to have symptoms. Their group also demonstrated in another study that all patients undergoing MEL procedures had a 33% narrowing of the neoostium at 1 year after surgery. Twenty-two of 77 patients had significant stenosis (>60%) and 9 patients (12%) required revision surgery. The accompanying endoscopic picture (see Fig. 4 ) shows extensive scarring from a MEL procedure after 2 years.




