Purpose
To determine the prevalence of inflammatory back pain in an anterior uveitis cohort.
Design
Retrospective cohort study.
Methods
Patients with anterior uveitis were recruited from the clinic of an ophthalmologist to complete a survey between March and December 2008. Patients were classified with inflammatory back pain if they had ≥2 positive responses to 4 validated inflammatory back pain questions: presence of morning stiffness >30 minutes in duration; improvement in back pain with exercise but not with rest; awakening from back pain during the second half of the night only; and presence of alternating buttock pain. Disease activity was assessed using the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI). The impact of disease on quality of life was measured using the EuroQOL (EQ-5D) questionnaire. Twenty-five patients underwent further rheumatologic examination.
Results
One hundred forty-one of 167 patients (84.4%) completed the survey. Sixty-six of 141 patients (46.8%) were classified to have inflammatory back pain. Mean BASDAI (4.2, SD 2.41) and EQ-5D scores (0.73, SD 0.21) were lower than patients with no inflammatory back pain (0.82, SD 0.16, P = .0048). In the subgroup that underwent rheumatologic assessment, a classification of inflammatory back pain was 92% sensitive and 67% specific for a diagnosis of inflammatory back pain.
Conclusions
The prevalence of inflammatory back pain in a cohort of anterior uveitis patients was found to be 46.8%. Patients with inflammatory back pain had worse quality of life than those without. Ophthalmologists may use these questions on back pain to select patients classified to have inflammatory back pain to refer for early rheumatologic assessment.
Depending on the predominant location of the inflammation in the eye, uveitis may be divided into anterior uveitis, intermediate uveitis, posterior uveitis, and panuveitis. Uveitis can occur as a manifestation of many diseases including infections, malignancy, and several systemic diseases. Thirty-seven percent to 50% of patients with anterior uveitis have no identifiable etiology to their inflammation and their uveitis is considered idiopathic.
The spondyloarthropathies are also known as seronegative or HLA-B27-associated arthropathies, a group of diseases that share common characteristics and preferentially involve the axial skeleton. Subcategories include ankylosing spondylitis, reactive arthritis (formerly known as Reiter syndrome), psoriatic arthritis, enteropathic spondylitis (or arthritis associated with inflammatory bowel disease), and undifferentiated spondyloarthropathies. Spondyloarthropathies overall are associated with 33% of anterior uveitis. Up to 40% of patients with ankylosing spondylitis, 26% with reactive arthritis, 25% with psoriatic arthritis, 37% with enteropathic spondylitis, and 13% of patients with undifferentiated spondyloarthropathy will develop acute anterior uveitis. Conversely, 50% of patients with anterior uveitis are HLA-B27 positive. Currently, there are limited data on the prevalence of spondyloarthropathies in an anterior uveitis population in Canada.
Spondyloarthropathy patients may develop restricted mobility and severe spinal deformity. Spinal stiffness and pain in spondyloarthropathies results in work disability being 3 times higher than the healthy population. Unfortunately, the diagnosis of spondyloarthropathies is often made late as symptoms may be overlooked or go undiagnosed until an extraspinal manifestation is identified. Uveitis, in particular anterior uveitis, is often a presenting feature of a spondyloarthropathy; so the ophthalmologist may be these patients’ earliest medical encounter. In a report of 175 consecutive patients with HLA-B27-associated uveitis, 65% of patients had uveitis prior to diagnosis of an extraocular disease.
Inflammatory back pain is defined as back pain attributable to a spondyloarthropathy. Thus, recognition that a patient’s back pain is inflammatory in nature can lead to earlier diagnosis of spondyloarthropathies. Early diagnosis is important as 1 study demonstrated that ankylosing spondylitis patients with uveitis tend to have more severe functional and radiologic outcomes than those without uveitis. Inflammatory back pain in patients with ankylosing spondylitis can be identified using validated criteria such as those defined by Rudwaleit. These criteria include positive responses to 2 out of 4 questions asked of the patient: presence of morning stiffness of more than 30 minutes in duration; improvement in back pain with exercise but not with rest; awakening because of back pain during the second half of the night only; and presence of alternating buttock pain.
In this study, we sought to determine the prevalence of inflammatory back pain using validated critieria in a population of anterior uveitis patients from a mixed community academic practice over 7.5 years (from September 2000 to March 2008). The degree of the patients’ inflammatory disease activity and impact of uveitis and back pain on their quality of life was also measured. We aim to determine the role that ophthalmologists can play to increase earlier detection of spondyloarthropathy so that the rheumatologist can intervene earlier in the disease process. We also examine the sensitivity and specificity of the 4-question survey to identify patients with inflammatory back pain in this anterior uveitis population.
Methods
Patient Selection
Three hundred and forty-four patients with a diagnosis of anterior uveitis from the clinical uveitis database of a mixed community and academic practicing ophthalmologist (L.D.) were invited to participate in a survey from March to December 2008. This database included all patients who received a diagnosis of anterior uveitis in the ophthalmology practice over a 7.5-year period. Inclusion criteria included being 18 years old or over and patient ability to complete an English-language questionnaire. Patients were mailed an introductory letter from their ophthalmologist and 10 days later were contacted by phone by research staff. If no phone contact had been made by the researchers after 2 weeks of calling at various times (day and evening), or if an automated message indicated the number was no longer in use, a copy of the informed consent form and study survey were mailed to the patient’s last known address. Reminder letters were mailed 14 days later if there had been no response. If all these attempts to contact the patients failed, they were considered uncontactable.
Patients were excluded if they could not be reached by mail or phone (up to 20 repeated phone calls per patient were made), declined to participate, claimed to have no uveitis, were deceased, were unable to complete an English-language questionnaire, or were mentally or physically unable to participate. Clinic chart review was performed for the patients who completed the informed consent process and survey. A sample of 25 patients who completed the survey also underwent a complete rheumatologic examination (by M.S.) to verify their diagnosis of inflammatory back pain, to determine if they had a spondyloarthropathy, and to rule out back pain caused by other sources. Where clinically indicated, patients underwent laboratory and radiographic examination to confirm the presence of sacroilitis and disease subclassification. This allowed for data analysis to determine the sensitivity and specificity of the 4-question survey to identify patients with inflammatory back pain in this anterior uveitis population. The diagnosis of a spondyloarthropathy was made using the European Spondyloarthropathy Study Group criteria as the Assessment for Ankylosing Spondylitis criteria were not published at the time this study began.
Survey Content
Demographic information was collected and previously described and validated questions for inflammatory back pain were used in our questionnaire. As noted above, the back pain questions consisted of 4 items: 1) presence of morning stiffness of more than 30 minutes in duration; 2) improvement in back pain with exercise but not with rest; 3) awakening because of back pain during the second half of the night only; and 4) presence of alternating buttock pain. The author of these criteria has since updated and published new criteria, but at the time of our study design, these were the criteria available.
The degree of inflammatory disease activity was assessed using the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI). The BASDAI series of questions has been validated to demonstrate sensitivity to changes in treatment in patients with ankylosing spondylitis. According to international guidelines for commencement of biologic agents, one of the criteria for suitability is disease activity greater than 4 on the BASDAI.
The impact of uveitis and back pain on patients’ quality of life was measured using the EuroQOL (EQ-5D utility/health index, a weighted score) questionnaire. Patients rated the state of their health in 5 categories: mobility; ability with self-care; ability to perform usual activities such as work, study, housework, family, or leisure; amount of pain or discomfort; and presence of anxiety or depression. A score of 0 meant the worst health state and a score of 1 meant the best health state.
Patient Chart Review
Patients’ ophthalmology charts were retrospectively reviewed for clinical information on results of investigations performed, including human leukocyte antigen (HLA-B27), and etiology of the anterior uveitis.
Data Analysis
Data analysis was conducted using SAS v9.1 (SAS Institute Inc, Cary, North Carolina, USA). The specificity and sensitivity of having a positive response to 2 of the 4 back pain questions was calculated for the 25 patients who underwent complete rheumatologic examination.
Results
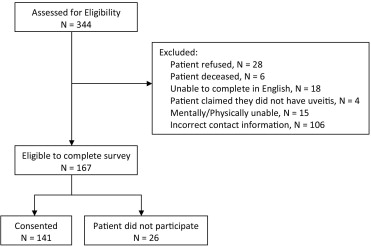
Of the 344 patients who had a diagnosis of anterior uveitis in the clinical database, 177 (51%) were excluded because they could not be reached by multiple phone and mailing attempts (106), declined to participate (28), claimed to have no uveitis (4), were deceased (6), were unable to complete an English-language questionnaire (18), and were mentally or physically unable to participate (15). Patients for whom phone contact was never made received an average of 6.5 calls at various times of the day and evening. The response rate was 84% (141/167) for the remaining 167 patients who were invited to complete the survey. Twenty-six patients (16%) did not return the survey ( Figure ).
Sixty-six of 141 patients (46.8%) had 2 or more positive responses to the questions about their back pain and were thus classified to have inflammatory back pain. Improvement of back pain with exercise was answered most often positively in 58 of 66 patients (87.9%). The distribution of all patients’ responses is shown in Table 1 . Patient demographic information and clinical outcomes such as disease activity as measured by BASDAI and health-related quality of life (HRQOL), as measured by EQ-5D and HLA-B27 positivity, are presented in Table 2 . Patients with inflammatory back pain had a significantly lower HRQOL with a mean EQ-5D score of 0.72 compared to patients without inflammatory back pain (0.82, P = .005). HLA-B27 was positive in 28 of 54 tested patients (52%) with inflammatory back pain compared to 17 of 55 tested patients (31%) without inflammatory back pain ( P = .033). Overall, an HLA-B27-related association was found in 45 of 141 patients (31.9%), although 33 of 141 patients (23%) did not undergo HLA-B27 testing and other diagnostic investigations by ophthalmology, especially if the patient had a previous rheumatologic diagnosis. Seventy-six of 141 patients (54.3%) had bilateral anterior uveitis disease. The most common anterior uveitis etiologies or associations found in our cohort included idiopathic, HLA-B27-positive without a spondyloarthropathy diagnosis, ankylosing spondylitis, and infectious causes ( Table 3 ). Idiopathic means HLA-B27-negative and also negative for other causes of uveitis by review of systems, examination, and lab testing. HLA-B27-positive means HLA-B27-positive serology. In situations where a systemic diagnosis (ankylosing spondylitis, Crohn, psoriasis, sarcoidosis, Reiter syndrome) was already made, HLA-B27 test was not always done.
| Question | Response | % Yes | |
|---|---|---|---|
| Yes | No | ||
| Do you ever have a “stiff” back in the morning that lasts more than 30 minutes? | 54 | 86 | 38.3% |
| Do you ever have back pain that gets better when you exercise and not when you rest? | 74 | 65 | 52.5% |
| Does your back pain ever wake you up in the middle of the night (after you have slept for a few hours)? | 43 | 97 | 30.5% |
| Do you have buttock pain that moves from side to side? | 38 | 102 | 27.0% |
| Inflammatory Back Pain (N = 66) | No Inflammatory Back Pain (N = 75) | |
|---|---|---|
| Mean age at survey, years (SD) | 45.6 (13.4) | 51.4 (16.0) |
| # Male (%) | 22 (33.3) | 42 (56) |
| # Female (%) | 44 (66.7) | 42 (56) |
| # White (%) | 55 (83.3) | 49 (65.3) |
| Mean BASDAI Score (SD) a | 4.2 (2.4) | Test does not apply to patients with noninflammatory back pain |
| Mean EuroQOL-5D Score (SD) b, c | 0.72 (0.21) | 0.82 (0.16) |
| # Patients tested for HLA-B27 (%) d | 54 (82) | 55 (73) |
| # Patients HLA-B27-positive (%) e | 28 (42) | 17 (23) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


