Purpose
To compare the prevalence and risk factors for age-related macular degeneration (AMD) in 2 Indian populations, 1 living in urban Singapore and 1 in rural central India.
Design
Population-based, cross-sectional studies of Indians aged 40+ years.
Methods
Our analysis included 3337 Singapore-residing participants and 3422 India-residing participants. All participants underwent comprehensive systemic and ocular examinations and retinal photography. AMD was graded from retinal photographs according to the Wisconsin Age-Related Maculopathy Grading System. Systemic and ocular risk factors were assessed for association with AMD.
Results
Singapore-residing participants were older (mean age 57.8 years vs 53.8 years) and, after adjusting for age and sex, were more likely to have previous cataract surgery, higher body mass index, hypertension, diabetes, previous myocardial infarction, higher cholesterol, and lower creatinine levels, but less likely to be current smokers, than India-residing participants. The age-standardized prevalence of early and late AMD was 4.45% and 0.34%, respectively, in Singapore and 5.80% and 0.16%, respectively, in India. Shorter axial length was associated with early AMD in both Singapore and India, whereas previous cataract surgery, higher body mass index, hypertension, and lower cholesterol were associated with early AMD in Singapore but not in India.
Conclusion
The prevalence of AMD was similar among Indian adults living in urban Singapore and rural India, despite differences in cardiovascular risk factor profile and demographics.
Age-related macular degeneration (AMD) is a major cause of vision loss in elderly people. There are fewer studies of AMD in Asian populations, although a recent meta-analysis reported prevalence estimates of 6.8% for early AMD and 0.56% for late AMD in Asians, similar to rates of 8.8% for early AMD and 0.59% for late AMD in age-standardized white persons.
The number of elderly persons in Asia is expected to substantially increase in the next few decades, with an estimated 25% of Asians aged 60 years and older by 2050. Indians comprise one-fifth of the world’s population with 1.21 billion people, including 76 million persons aged 60 years and above. Population studies among Indian residents living in India have reported wide-ranging prevalence rates between 2.7% and 8.9% for early AMD and between 0.18% and 1.8% for late AMD. This variation may be at least partly explained by the difference in age groups sampled, difference in methodology (AMD grading methods and definition), and, importantly, possibly different patterns of risk factors between persons living in rural vs urban settings. For example, the Andhra Pradesh Eye Study reported an association between AMD and cigar smoking, the presence of cortical cataract, and prior cataract surgery. Lower socioeconomic status was also found to be a risk factor for AMD. The Central India Eye and Medical Study, however, did not show an association between smoking or lens thickness and AMD. Whether AMD is more frequent in persons of Indian descent who have migrated to other countries is unclear, given the differences in socioeconomic, lifestyle, and medical risk factor profiles and health care systems. With a higher prevalence of cardiovascular risk factors in these migrant populations, it is reasonable to believe AMD may be more prevalent.
To address this question, we describe the prevalence and risk factors for AMD among Indians living in urban Singapore and compare AMD prevalence and associated risk factors with Indians living in rural central India. Our study provides a unique opportunity to assess whether marked differences in environment risk factors are associated with the development of AMD.
Methods
Study Design and Population
Data from 2 population-based cross-sectional studies of Indian adults in Singapore and India were used. The Singapore Indian Eye Study examined adult Indians aged 40-83 years living in Singapore between August 2007 and December 2009 and was approved by the Singhealth Institutional Review Board. The Central India Eye and Medical Study was conducted in central India in 8 villages comprising the rural region of central Maharashtra at a distance of approximately 40 km from Nagpur from April 2006 to August 2008. Both the Medical Ethics Committee of the Medical Faculty Mannheim of the Ruprecht-Karls-University Heidelberg and the Ethical Committee of the Suraj Eye Institute (Nagpur) approved the study. All participants gave informed consent, and both studies were conducted according to the Declaration of Helsinki.
Details of study methodology have been reported. Briefly, for the Singapore cohort, from a list of 12 000 Indians residing in southwest Singapore provided by the Ministry of Home Affairs, an age-stratified random sampling strategy was conducted to select 6350 subjects aged 40 years or older, of which 4497 subjects were eligible. Of these, 3400 (75.6%) participated in the study. A total of 3337 (98.1%) subjects had fundus photographs of adequate quality for AMD grading. For the rural India cohort, 5885 subjects aged above 30 years were invited to participate, of which 4711 (80.1%) participated. For the purpose of the current analysis on AMD, only subjects aged 40 years and above (3591; 76.2%) were included. Of these, 3422 eyes (95.3%) had fundus photographs of adequate quality for AMD grading. Singapore-residing participants were generally older (57.8 years, SD 10.1 vs 53.8 years, SD 11.1; P < .001) and more likely to be male (50.2% vs 47.3%; P = .02) than India-residing participants ( Supplemental Table 1 , available at AJO.com ).
Retinal Photography and Age-Related Macular Degeneration Grading
In both studies, digital retinal photographs were taken after pupil dilation and grading was performed following a modification of the Wisconsin age-related maculopathy grading system. In Singapore, color photographs of Early Treatment Diabetic Retinopathy Study (ETDRS) standard field 1 (centered on the optic disc) and ETDRS standard field 2 (centered on the fovea) of each eye were obtained (Canon CR-DGi with a 10-D SLR back; Canon, Tokyo, Japan). The photographs were graded for AMD signs at the Centre for Vision Research, University of Sydney, Australia. In India, digital photography of the lens, optic disc (20-degree), and the disc and macula (50-degree) was captured (Zeiss FF450 telecentric fundus camera; Zeiss Meditec, Oberkochen, Germany). For the assessment of AMD, the international classification of the Wisconsin age-related maculopathy grading system was used and performed in Nagpur. Each photograph was independently adjudicated by 2 senior graders (V.N. and J.J.). Differences in final classification were discussed and resolved.
Among the AMD features evaluated were drusen size, type, and area; increased retinal pigment; retinal pigment epithelial depigmentation; pure geographic atrophy; and signs of exudative macular degeneration. Drusen were classified as hard or soft; then soft drusen were divided into distinct and indistinct soft drusen. Retinal pigmentary abnormalities were graded as hypopigmentation and hyperpigmentation. Early AMD was defined by either any soft drusen (distinct or indistinct) and pigmentary abnormalities or large soft drusen 125 μm or more in diameter with a large drusen area (>500-μm-diameter circle) or large soft indistinct drusen in the absence of signs of late AMD, following the definitions used in the Blue Mountains Eye Study. Neovascular AMD lesions were defined as the presence of retinal pigment epithelium (RPE) detachment, neurosensory detachment, subretinal or sub-RPE hemorrhages, or intraretinal, subretinal, or sub-RPE scar tissue. Subretinal hemorrhages or hard exudates within the macular area were also considered signs of neovascular AMD if other retinal vascular diseases as alternative causes were ruled out. Geographic atrophy was defined by presence of visible choroidal vessels and a discrete atrophic area with sharp border and an area at ≥175 μm diameter. Late AMD was defined as having either neovascular AMD or geographic atrophy.
Risk Factors
We defined risk factors using similar definitions for the purpose of this analysis. All examinations were performed in the Singapore Eye Research Institute (for Singapore-residing participants) or Suraj Eye Institute (for India-residing participants) by trained research staff. Trained interviewers administered questionnaires at the respective site, to collect information on sociodemographic and lifestyle factors. Demographic variables included age, sex, marital status, education level, occupation, income, and family history of diabetes and hypertension. Age was defined as the age at examination. Lifestyle questions were asked about smoking habits and alcohol consumption. Physical examination included anthropometric measurements, blood pressure (BP), and a detailed ocular examination. In the Singapore-residing participants, blood pressure was measured using a digital automatic blood pressure monitor (Dinamap model Pro100V2; Criticon GmbH, Norderstedt, Germany), following the protocol used in the Multi-Ethnic Study of Atherosclerosis. The average of the 2 systolic and diastolic BP measurements, taken with participant sitting down, was used. In the India-residing participants, BP was measured by a trained technician. The study participants were sitting for at least 5 minutes and had refrained from smoking and drinking of coffee, tea, or alcohol for at least 3 hours. In addition, no exercise was performed for the last 30 minutes prior to the BP measurements. An automated mercury sphygmomanometer (Model IA2 [HEM-7011-C1]; Omron Healthcare Co Ltd, Kyoto, Japan) was used and the cuff size was chosen according to the measured circumference of the upper arm. Laboratory examination included measurement of fasting plasma glucose and lipids.
Cigarette smoking was categorized into current smokers, former smokers, or nonsmokers and alcohol consumption into drinkers (irrespective of quantity) and nondrinkers. Cardiovascular disease (CVD) was defined as self-reported myocardial infarction or angina or stroke. Hypertension was defined as systolic BP ≥140 mm Hg or diastolic BP ≥90 mm Hg or self-reported physician-diagnosed hypertension. For the Singapore-residing participants, diabetes mellitus was defined as random glucose of 11.1 mmol/L or more, a self-reported physician diagnosis of diabetes, or use of glucose-lowering medication. For the India-residing participants, diabetes mellitus was defined as hemoglobin A1C (HbA1C) ≥6.0% (performed in only 2423 participants) or random blood glucose ≥200 mg/dL or self-reported physician diagnosis. Dyslipidemia was defined as total cholesterol ≥6.2 mmol/L, low-density lipoprotein (LDL) cholesterol ≥4.1 mmol/L, high-density lipoprotein (HDL) cholesterol <1.0 mmol/L, or self-reported physician-diagnosed dyslipidemia.
Ocular Parameters
Refractive error in both eyes of each subject was determined by a trained technician using an autorefractor (Canon RK-5 Auto Ref-Keratometer; Canon Inc, Ltd, Tokyo, Japan) (both Singapore-residing and India-residing participants), after which subjective refraction was performed by an optometrist to achieve best-corrected visual acuity. The final subjective refraction result was used in the analysis. Spherical equivalent (SE) was defined as sphere plus half negative cylinder. Refractive errors were analyzed as a continuous variable.
Axial length (AL) and anterior chamber depth (ACD) were measured by trained technicians using noncontact partial coherence laser interferometry (IOLMaster version 3.01; Carl Zeiss Meditec AG, Jena, Germany) (for Singapore-residing participants). Corneal pachymetry was measured with US-1800 Echoscan (Nidek, Fremont, California, USA) in the Singapore cohort. Corneal pachymetry and ocular biometry were obtained by trained technicians with Pacscan (Sonomed, Lake Success, New York, USA) in the India cohort.
Statistical Analyses
All statistical analyses were performed using R version 2.13.2 (R Development Core Team, 2011; R Foundation for Statistical Computing, Vienna, Austria). Characteristics of the study population were described using proportions or means and standard deviation (SD). Age-standardized prevalence estimates were calculated using the direct method. The 2010 Singapore Indian population was used as the standard population for comparison of the Singapore and India cohort. Age strata–specific prevalence rates were weighted by the proportions of the corresponding strata in the population census, and then summed to give a summary prevalence rate. The relationship between early AMD and risk factors was analyzed using logistic regression adjusting for age and sex. Mixed-effects logistic regression was used to model combined data from Singapore site and India site with study effect as the random effect to control for heterogeneity between 2 studies. Age- and sex-adjusted mixed-effects logistic regression was performed to select potential confounders ( P < .05) for multivariate analysis, with final covariates selected including age, sex, body mass index (BMI), cholesterol, arterial hypertension, refractive error, myocardial infarction, intraocular pressure (IOP), central corneal thickness, and study effect.
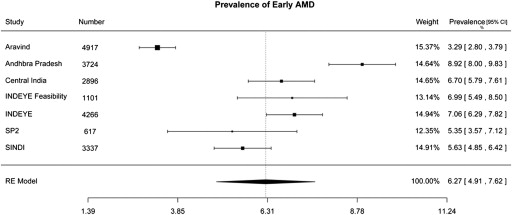
Finally, we performed a comparative analysis of the age-specific prevalence of AMD from Indian subjects aged 40 years and above. We performed a PubMed search for relevant papers of population-based studies reporting AMD prevalence in Indians published from January 1, 1990 through September 18, 2012, using the terms “age-related macular degeneration” AND “prevalence” AND “population study” AND (“Indian” OR “Indians” OR “India”). Twenty-six articles were identified initially, of which 17 were assessed as relevant (C.M.G.C.) for the purpose of reporting prevalence of AMD among Indian persons within a population-based study sample. All 17 articles were from one of the 6 population studies, namely the Aravind Comprehensive Eye Study, the Andhra Pradesh Eye Disease Study, the Central India Eye and Medical Study, the INDEYE feasibility study, the INDEYE study, and the Singapore Prospective Study Program. These studies were included in the meta-analysis.
We used a random-effects model because of the heterogeneity among these studies. These studies were selected after publication bias was assessed in a funnel plot, using Egger’s test. For ocular parameter analysis, data of the eyes with AMD was selected. If both eyes or neither eye had AMD, then data of the right eye were used for analysis.
Results
Characteristics of the participants are summarized in Table 1 . There are marked differences in body weight, height, and BMI; smoking and alcohol intake; medical history (blood pressure, diabetes, cholesterol, history of myocardial infarction); ocular measurements (axial length, central corneal thickness, IOP); and lens status. In particular, the prevalence of diabetes and hypertension were noted to be markedly lower in the India cohort than in the Singapore cohort. We therefore present the prevalence defined by self-reported diagnoses and also by objective disease definition criteria stated above. After adjusting for age and sex, Singapore-residing participants were more likely to have higher BMI, hypertension, diabetes, previous myocardial infarction, higher cholesterol, and lower creatinine levels, but were less likely to consume alcohol or to be current smokers. Singapore-residing participants also tended to have longer axial length, deeper anterior chambers, and thicker central corneal thickness. A significantly higher proportion of Singapore-residing participants had previous cataract surgery (12.2%) compared with the India-residing participants (4.5%) ( P < .001).
| Singapore Indian Eye Study (N = 3337) | Central India Eye & Medical Study (N = 3422) | P Value a | ||
|---|---|---|---|---|
| BMI, kg/m 2 | 26.18 (4.75), n = 3323 | 19.76 (3.54), n = 3421 | <.001 | |
| Diastolic blood pressure, mm Hg | 77.41 (10.09), n = 3337 | 75.03 (12.11), n = 3422 | <.001 | |
| Systolic blood pressure, mm Hg | 135.32 (19.59), n = 3337 | 126.7 (22.24), n = 3422 | <.001 | |
| Total cholesterol, mmol/L | 5.19 (1.1), n = 3203 | 4.57 (0.76), n = 3249 | <.001 | |
| HDL, mmol/L | 1.07 (0.32), n = 3203 | 0.9 (1.75), n = 3250 | <.001 | |
| Creatinine, mmol/L | 77.75 (33.7), n = 3202 | 92.27 (198.2), n = 3245 | <.001 | |
| Never smoked | ||||
| No | 886 (26.6%) | 717 (21.9%) | ||
| Yes | 2449 (73.4%) | 2562 (78.1%) | <.001 | |
| Current smoking | ||||
| No | 2843 (85.3%) | 2712 (82.7%) | .003 | |
| Yes | 489 (14.7%) | 567 (17.3%) | ||
| Alcohol consumption | ||||
| No | 2912 (87.4%) | 2524 (77%) | <.001 | |
| Yes | 421 (12.6%) | 755 (23%) | ||
| Hypertension | Self-Reported | Measured and Self-Reported | ||
| No | 1450 (43.5%) | 3049 (93%) | 2546 (74.4%) | <.001 |
| Yes | 1881 (56.5%) | 230 (7%) | 876 (25.6%) | |
| Diabetes | Self-Reported | Measured and Self-Reported | ||
| No | 2137 (65.9%) | 3226 (98.4%) | 1369 (93.6%) | <.001 |
| Yes | 1105 (34.1%) | 53 (1.6%) | 94 (6.4%) | |
| Angina (self-reported) | ||||
| No | 3138 (94.3%) | 3108 (94.8%) | .88 | |
| Yes | 190 (5.7%) | 171 (5.2%) | ||
| Myocardial infraction (self-reported) | ||||
| No | 3030 (91%) | 3234 (98.6%) | <.001 | |
| Yes | 298 (9%) | 45 (1.4%) | ||
| Cataract surgery | ||||
| No | 2927 (87.8%) | 3259 (95.5%) | <.001 | |
| Yes | 408 (12.2%) | 155 (4.5%) | ||
| Refractive error, b diopter | −0.07 (2.17), n = 3290 | −0.03 (1.9), n = 3399 | .46 | |
| Axial length, mm | 23.41 (1.12), n = 3326 | 22.63 (0.9), n = 3400 | <.001 | |
Early AMD was present in 188 subjects in the Singapore cohort and 209 subjects in the India cohort, giving crude prevalence rates of 5.6% and 6.1%, respectively. Both crude and age-standardized prevalence of AMD are summarized in Table 2 . Age-standardized prevalence for early AMD was lower in the Singapore cohort (4.45%) than in the India cohort (5.80%) ( P = .01). Prevalence of early AMD was associated with increasing age in both populations ( P < .001), though this was less marked in India-residing participants. There was no significant difference in the prevalence of early AMD between men and women in either study. Late AMD was present in 14 Singapore-residing participants and 8 India-residing participants, giving a crude prevalence of 0.42% and 0.23%, respectively. The corresponding age-standardized prevalence of late AMD was 0.34% (Singapore) and 0.16% (India) ( P = .46). Prevalence of combined early and late AMD increased significantly with increasing age in both cohorts ( P < .001).
| Singapore Indian Eye Study (N = 3337) | Central India Eye & Medical Study (N = 3422) | |
|---|---|---|
| Early AMD Cases | Early AMD Cases | |
| 40-49 | 20 (2.3%) | 41 (3.0%) |
| 50-59 | 35 (3.2%) | 63 (8.0%) |
| 60-69 | 62 (7.1%) | 68 (8.1%) |
| 70-79 | 57 (13.7%) | 33 (9.0%) |
| 80+ | 14 (19.4%) | 4 (7.3%) |
| P value a | <.001 | <.001 |
| Crude prevalence | 188 (5.6%) | 209 (6.1%) |
| Age-standardized prevalence b | 4.45% (3.78, 5.23) | 5.80% (5.00, 6.71) |
| Male N = 1674 | Female N = 1663 | P | Male N = 1619 | Female N = 1803 | P | |
|---|---|---|---|---|---|---|
| 40-49 | 11 (2.6%) | 9 (2.0%) | 24 (3.8%) | 17 (2.3%) | ||
| 50-59 | 21 (3.9%) | 14 (2.5%) | 29 (7.4%) | 34 (8.6%) | ||
| 60-69 | 33 (7.2%) | 29 (7.0%) | 30 (9.0%) | 38 (7.5%) | ||
| 70-79 | 31 (14.8%) | 26 (12.6%) | 23 (10.4%) | 10 (6.4%) | ||
| 80+ | 9 (23.1%) | 5 (15.2%) | 4 (9.1%) | 0 (0.0%) | ||
| P value a | <.001 | <.001 | <.001 | <.001 | ||
| Crude prevalence | 105 (6.3%) | 83 (5.0%) | .11 | 110 (6.2%) | 99 (5.5%) | .33 |
| Age-standardized prevalence b | 4.83% (3.83, 6.07) | 4.08% (3.20, 5.17) | 6.14% (4.98, 7.51) | 5.42% (4.34, 6.84) |
a P value of test for linear trend for age group.
b Estimated prevalence (95% confidence interval) for projection by age standardized to the Singapore Census 2010 Indian population.
Analysis of the relationship between risk factors for AMD is summarized in Table 3 . After adjusting for age and sex, only increasing hyperopic refractive error and shorter axial length were associated with early AMD in both cohorts. In addition, previous cataract surgery, hypertension, previous myocardial infarction, higher BMI, and lower cholesterol were associated with early AMD in Singapore but not in India. Within the Singapore population, there was no significant difference in the risk for AMD between subjects born in Singapore and those born outside, or in the duration of years living in Singapore among the latter group (data not shown).
| Singapore Indian Eye Study (N = 3337) | Central India Eye & Medical Study (N = 3422) | |||
|---|---|---|---|---|
| OR (95% CI) a | P Value | OR (95% CI) a | P Value | |
| Age, per year | 1.08 (1.06, 1.09) | <.001 | 1.04 (1.02, 1.05) | <.001 |
| Sex, female vs male | 0.82 (0.61, 1.11) | .20 | 0.87 (0.65, 1.15) | .33 |
| BMI, per 1 unit | 1.03 (1.00, 1.06) | .04 | 1.01 (0.97, 1.05) | .66 |
| Diastolic blood pressure, per mm Hg | 1.00 (0.99, 1.02) | .58 | 0.99 (0.98, 1) | .20 |
| Systolic blood pressure, per mm Hg | 1.00 (1.00, 1.01) | .26 | 1 (0.99, 1.01) | .76 |
| Total cholesterol | 0.8 (0.69, 0.93) | .003 | 1.14 (0.89, 1.46) | .30 |
| HDL | 0.77 (0.46, 1.26) | .31 | 0.99 (0.78, 1.25) | .90 |
| Creatinine | 1 (0.99, 1) | .21 | 1 (0.99, 1) | .79 |
| Never smoked | 0.96 (0.65, 1.43) | .86 | 1.19 (0.73, 1.98) | .49 |
| Current smoking | 0.84 (0.51, 1.36) | .50 | 0.7 (0.39, 1.2) | .21 |
| Alcohol consumption | 1.03 (0.63, 1.62) | .91 | 1.47 (0.89, 2.43) | .14 |
| Hypertension (measured and self-reported) | 1.48 (1.03, 2.15) | .04 | 0.96 (0.69, 1.32) | .80 |
| Diabetes (measured and self-reported) | 0.94 (0.68, 1.28) | .68 | 1.24 (0.47, 2.77) | .63 |
| Angina | 1.14 (0.64, 1.91) | .64 | 1.6 (0.74, 3.06) | .19 |
| Myocardial infarction | 1.52 (1, 2.26) | .04 | 0.45 (0.03, 2.13) | .44 |
| Cataract surgery | 1.62 (1.09, 2.38) | .016 | 0.89 (0.46, 1.57) | .70 |
| Refractive error, per diopter b | 1.15 (1.05, 1.29) | .006 | 1.15 (1.05, 1.25) | .003 |
| Axial length, per 1 mm | 0.83 (0.7, 0.97) | .02 | 0.78 (0.65, 0.92) | .004 |
Multivariate-adjusted odds ratios for association between risk factors for early AMD are summarized in Supplemental Table 2 (available at AJO.com ). Early AMD was associated with increasing age and shorter axial length in both studies. After adjusting for age, sex, BMI, cholesterol, hypertension, myocardial infarction, axial length, IOP, and central corneal thickness, the “study effect” variable was not significant, suggesting that there is no significant difference in the risk for early AMD between the 2 cohorts.
Finally, in a meta-analysis of age-specific prevalence of AMD from 20 920 Indian subjects aged 40 years and above from 7 studies, we estimated a 6.27% (95% CI, 4.91%-7.62%) pooled prevalence estimate for early AMD in Indian people ( Figure ).
Results
Characteristics of the participants are summarized in Table 1 . There are marked differences in body weight, height, and BMI; smoking and alcohol intake; medical history (blood pressure, diabetes, cholesterol, history of myocardial infarction); ocular measurements (axial length, central corneal thickness, IOP); and lens status. In particular, the prevalence of diabetes and hypertension were noted to be markedly lower in the India cohort than in the Singapore cohort. We therefore present the prevalence defined by self-reported diagnoses and also by objective disease definition criteria stated above. After adjusting for age and sex, Singapore-residing participants were more likely to have higher BMI, hypertension, diabetes, previous myocardial infarction, higher cholesterol, and lower creatinine levels, but were less likely to consume alcohol or to be current smokers. Singapore-residing participants also tended to have longer axial length, deeper anterior chambers, and thicker central corneal thickness. A significantly higher proportion of Singapore-residing participants had previous cataract surgery (12.2%) compared with the India-residing participants (4.5%) ( P < .001).
| Singapore Indian Eye Study (N = 3337) | Central India Eye & Medical Study (N = 3422) | P Value a | ||
|---|---|---|---|---|
| BMI, kg/m 2 | 26.18 (4.75), n = 3323 | 19.76 (3.54), n = 3421 | <.001 | |
| Diastolic blood pressure, mm Hg | 77.41 (10.09), n = 3337 | 75.03 (12.11), n = 3422 | <.001 | |
| Systolic blood pressure, mm Hg | 135.32 (19.59), n = 3337 | 126.7 (22.24), n = 3422 | <.001 | |
| Total cholesterol, mmol/L | 5.19 (1.1), n = 3203 | 4.57 (0.76), n = 3249 | <.001 | |
| HDL, mmol/L | 1.07 (0.32), n = 3203 | 0.9 (1.75), n = 3250 | <.001 | |
| Creatinine, mmol/L | 77.75 (33.7), n = 3202 | 92.27 (198.2), n = 3245 | <.001 | |
| Never smoked | ||||
| No | 886 (26.6%) | 717 (21.9%) | ||
| Yes | 2449 (73.4%) | 2562 (78.1%) | <.001 | |
| Current smoking | ||||
| No | 2843 (85.3%) | 2712 (82.7%) | .003 | |
| Yes | 489 (14.7%) | 567 (17.3%) | ||
| Alcohol consumption | ||||
| No | 2912 (87.4%) | 2524 (77%) | <.001 | |
| Yes | 421 (12.6%) | 755 (23%) | ||
| Hypertension | Self-Reported | Measured and Self-Reported | ||
| No | 1450 (43.5%) | 3049 (93%) | 2546 (74.4%) | <.001 |
| Yes | 1881 (56.5%) | 230 (7%) | 876 (25.6%) | |
| Diabetes | Self-Reported | Measured and Self-Reported | ||
| No | 2137 (65.9%) | 3226 (98.4%) | 1369 (93.6%) | <.001 |
| Yes | 1105 (34.1%) | 53 (1.6%) | 94 (6.4%) | |
| Angina (self-reported) | ||||
| No | 3138 (94.3%) | 3108 (94.8%) | .88 | |
| Yes | 190 (5.7%) | 171 (5.2%) | ||
| Myocardial infraction (self-reported) | ||||
| No | 3030 (91%) | 3234 (98.6%) | <.001 | |
| Yes | 298 (9%) | 45 (1.4%) | ||
| Cataract surgery | ||||
| No | 2927 (87.8%) | 3259 (95.5%) | <.001 | |
| Yes | 408 (12.2%) | 155 (4.5%) | ||
| Refractive error, b diopter | −0.07 (2.17), n = 3290 | −0.03 (1.9), n = 3399 | .46 | |
| Axial length, mm | 23.41 (1.12), n = 3326 | 22.63 (0.9), n = 3400 | <.001 | |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


