Purpose
To introduce a new approach for short-term external scleral buckling with pneumatic retinopexy for the management of rhegmatogenous retinal detachment with inferior retinal breaks.
Design
Retrospective, noncomparative, interventional case series.
Methods
A review of 33 consecutive eyes of 31 patients who underwent external buckling with pneumatic retinopexy for uncomplicated rhegmatogenous retinal detachment with inferior retinal breaks from December 2006 through December 2010. An external buckle was made of a 505 sponge sutured along the blunt side of a 279 tyre (MIRA Inc). The buckle was inserted deeply into the inferior fornix without suture after pneumatic retinopexy and was kept in place for 3 days. Primary and final anatomic outcomes, visual acuity, and adverse events were recorded.
Results
All patients tolerated the procedure. The mean follow-up period was 24.0 months (range, 9 to 61 months). Primary success, defined as successful retinal reattachment within 6 months without further treatment, was achieved in 29 (87.9%) eyes. All patients attained final retinal reattachment (100%). Overall, the mean best-corrected visual acuity improved significantly at the end of follow-up (0.30 logarithm of the minimal angle of resolution units; Snellen equivalent, 6/12), compared with the preoperative best-corrected visual acuity (0.82 logarithm of the minimal angle of resolution units; Snellen equivalent, 6/38; P < .001).
Conclusions
Short-term external buckling with pneumatic retinopexy is a novel and effective treatment for rhegmatogenous retinal detachment with inferior retinal breaks, with a comparable success rate with other treatment methods. This approach also can avoid complications of long-term buckle implantation. Further comparative cohort studies may be necessary to compare the clinical efficacy with other conventional operations.
Rhegmatogenous retinal detachment (RRD) is an important cause of visual loss worldwide, with a reported annual incidence between 6.3 and 17.9 per 100 000 persons in Western countries. Approximately 29% of cases of RRD result from inferior retinal breaks. Among the main surgical options in treating RRD with inferior retinal breaks, vitrectomy shows favorable anatomic success rates, alone or in combination with scleral buckling. However, scleral buckling may be complicated by implant displacement, strabismus, refractive change, decreased retinal blood flow, and risk of anterior segment ischemia. In addition, vitrectomy may have associated progression of cataracts, intraocular pressure fluctuations, and late-onset glaucoma.
Pneumatic retinopexy has gained increasing popularity in the surgical management of RRD, with anatomic and visual outcomes comparable with other procedures. However, it originally was contraindicated for RRD with inferior retinal breaks. Chang and associates proposed inverted pneumatic retinopexy for the management of RRD with inferior retinal breaks and reported a single operation reattachment rate of 82%. Mansour and Hwang and associates also proposed pneumatic retinopexy with a modified head tilt position for RRD with inferior breaks, with initial success rates of 76.9% to 88.2%. Because all of these procedures require neck hyperextension or downward tilting of the head, the patients’ cardiovascular function, cervical spinal fitness, and compliance are still major concerns. The purpose of this study was to introduce and investigate pneumatic retinopexy with short-term placement of an external buckle for the management of RRD with inferior breaks.
Methods
The study protocol adhered to the tenets of the Declaration of Helsinki. Before the study began, it was approved by the Institutional Review Board of the Taipei Veterans General Hospital, Taipei, Taiwan (VGHIRB no.: 2012-02-001BC). Informed consent was obtained from each patient.
Study Subjects
A retrospective review was performed for consecutive patients with RRD with inferior retinal breaks who underwent pneumatic retinopexy together with an external buckle in Taipei Veterans General Hospital from December 2006 through December 2010. An inferior retinal break was defined as a break located between the 4-o’clock and 8-o’clock positions. The patients with primary RRD were enrolled in the primary group, and the patients with recurrent RRD with causative inferior retinal breaks were enrolled in the secondary group. The exclusion criteria included RRD with breaks posterior to the equator, giant tears, proliferative vitreoretinopathy, retinoschisis, and patients who had a too loose or shallow of an inferior fornix. The inferior fornix of the patients was considered to be too loose if the buckle could not be lodged firmly or too shallow if the buckle touched the cornea after being placed.
All of the operations were performed by 1 vitreoretinal specialist (P.K.L.). Under retrobulbar anesthesia and standard sterilization, the extent of retinal detachment (RD) and location of the breaks were identified. Transconjunctival cryopexy was applied around the retinal breaks. Anterior chamber paracentesis then was performed, followed by an injection of 0.4 to 0.7 mL pure perfluoropropane gas (C 3 F 8 ).
A customized external buckle was made from a 505 sponge sutured along the blunt side of a 279 tyre (MIRA Inc, Uxbridge, Massachusetts, USA) with several stitches of 6-0 black silk ( Figure 1 , Top left). The diameter of the 505 sponge was 5 mm and the width of the 279 tyre was 9 mm. The length of this complex buckle was trimmed to approximate the horizontal distance of the patient’s inferior fornix. The buckle then was disinfected with 10% povidone iodine (Sindine; Sinphar Pharmaceutical Co, Ltd, I-Lan, Taiwan) and rinsed with balanced salt solution (BSS Plus; Alcon Laboratories Inc, Fort Worth, Texas, USA). The buckle finally was covered with 0.3% gentamicin ointment (Oftalmolosa Cusi Gentamicin 0.3%; Alcon Cusi S.A., Barcelona, Spain) and was inserted deeply into the inferior fornix without sutures. The sponge part of this complex buckle was directed toward the inferior fornix and made contact with the eyeball ( Figure 1 , Top right and Bottom).
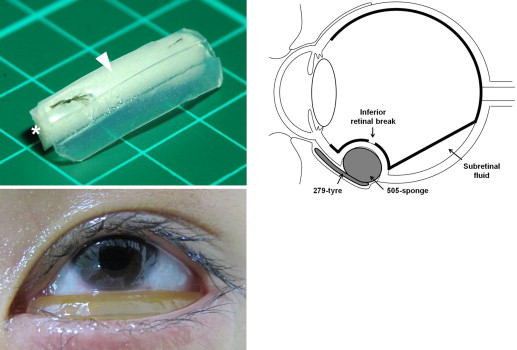
After the operation, the buckle was kept in place with the eye patched, and the patients remained in a face-down position with 5 to 10 degrees of neck flexion for 3 days. The postoperative in-hospital regimen included 1% prednisolone acetate (Pred Forte Ophthalmic Suspension 1%; Allergan Pharmaceuticals, Westport County, Ireland) 4 times daily, 0.25% chloramphenicol (Chloramphenicol Ophthalmic Solution 0.25%; Synpac-Kingdom Pharmaceutical Co, Ltd, Taipei, Taiwan) 4 times daily, and 0.3% gentamicin ointment every night. After removal of the buckle, the patients remained in the face-down position without neck flexion for another 7 days. If the buckle was found to be dislodged, it was disinfected immediately, covered with 0.3% gentamicin ointment, and inserted again by 1 of the authors (P.K.L.) or a doctor on duty. Supplementary laser photocoagulation around the breaks was carried out after the retina had reattached and the buckle had been removed. The postoperative intraocular ocular pressure (IOP) was monitored and kept to less than 25 mm Hg with IOP-lowering agents. All patients were hospitalized for 3 to 7 days, and they were followed up at 1 week and 2 weeks and then 1, 2, 3, and 6 months after discharge.
Primary anatomic success was defined as retinal reattachment at 6 months after a single operation without additional vitreoretinal surgery. Primary failure was defined as retinal redetachment within 6 months after the operation. Vitrectomy and endolaser photocoagulation then was arranged for these patients. Recurrence was defined as retinal redetachment at 6 months or more after the initial operation. The definition of final anatomic success was retinal reattachment at the end of follow-up. Clinical characteristics including age, gender, medical history, refraction status, laterality, history of trauma, lens status, macular involvement, extent of RRD, type and number of breaks, duration of follow-up, preoperative and postoperative best-corrected visual acuity (BCVA), IOP, use of IOP-lowering agents, and associated adverse events were recorded.
Statistical Analysis
Continuous and categorical variables of the demographic and medical characteristics were compared using the Student t test and Fisher exact test, respectively. Preoperative and postoperative BCVA, IOP, and number of IOP-lowering agents were compared using the paired t test. Measured Snellen visual acuities were converted to logarithm of the minimal angle of resolution (logMAR) values. Visual acuities of counting fingers and hand movements were assigned logMAR values of 2.0 and 3.0, respectively (Snellen equivalent, 6/600 and 6/6000, respectively). SPSS software for Windows version 18 (SPSS Inc, Chicago, Illinois, USA) was used for all calculations. A P value less than .05 was considered to be statistically significant.
Results
A total of 33 consecutive eyes in 31 patients were enrolled in this study, subdivided into 26 eyes in the primary group and 7 eyes in the secondary group. Two patients with proliferative vitreoretinopathy change and 1 patient with a shallow inferior fornix were excluded. The mean age of the enrolled patients was 48.8 years (range, 17 to 81 years), with a mean follow-up time of 24.0 months (range, 9 to 61 months). The proportion of pseudophakic RRD was higher in the secondary group than in the primary group (42.9% vs 23.1%; P = .36). The average extent of RD was 5.0 clock hours (range, 1 to 12 clock hours), with a mean of 1.6 breaks (range, 1 to 4 breaks). Of the 33 eyes, 20 (60.6%) had macular detachment, of which 14 (70%) were in the primary group and 6 (30%) were in the secondary group ( Table 1 ). The mean duration from onset of symptoms to seeking medical help in the patients with macular detachment was 15.7 days (range, 1 to 60 days). All patients were hospitalized for 3 to 7 days (mean, 5.5 days). Postoperative lid swelling and chemosis can prohibit fundus examination to some extent. In the patients with mild lid swelling, retinal indentation from the buckle with a correct location relative to the breaks was observed.
| Total (n = 33) | Primary Group (n = 26) | Secondary Group (n = 7) | |
|---|---|---|---|
| Age (y) | 48.8 ± 19.9 (17 to 81) | 47.0 ± 20.8 (17 to 81) | 55.3 ± 15.7 (35 to 81) |
| Spherical equivalent (D) | −4.83 ± 4.72 (−13.50 to 4) | −4.52 ± 4.33 (−12.25 to 4) | −6.63 ± 7.08 (−13.50 to 1.5) |
| Male gender (%) | 20 (60.6%) | 15 (57.7%) | 5 (71.4%) |
| Laterality (% right eye) | 16 (48.5%) | 11 (42.3%) | 5 (71.4%) |
| Trauma | 4 (12.1%) | 3 (11.5%) | 1 (14.3%) |
| Lens status (% pseudophakic) | 9 (27.3%) | 6 (23.1%) | 3 (42.9%) |
| Macular status (% off) | 20 (60.6%) | 14 (53.8%) | 6 (85.7%) |
| RD extent (clock hours) | 5.0 ± 2.5 (1.0 to 12) | 5.2 ± 2.7 (1.0 to 12) | 4.2 ± 1.0 (3.3 to 6) |
| Break types a | |||
| Flap tear | 11 (33.3%) | 6 (23.1%) | 5 (71.4%) |
| Round hole | 22 (66.7%) | 20 (76.9%) | 2 (28.6%) |
| No. of breaks | 1.6 ± 1.0 (1 to 4) | 1.8 ± 1.1 (1 to 4) | 1.1 ± 0.4 (1 to 2) |
| Follow-up (mos) | 24.0 ± 17.5 (9 to 61) | 22.5 ± 17.4 (9 to 61) | 29.7 ± 18.1 (12 to 60) |
a There was a significant difference in break types between the primary and secondary groups ( P = .027).
In the secondary group, 4 patients underwent vitrectomy with endolaser photocoagulation, and 3 patients received pneumatic retinopexy as the primary operation. However, all 7 patients demonstrated recurrent RRD 1 to 4 months later as a result of new inferior breaks and underwent pneumatic retinopexy with external buckling as salvage management.
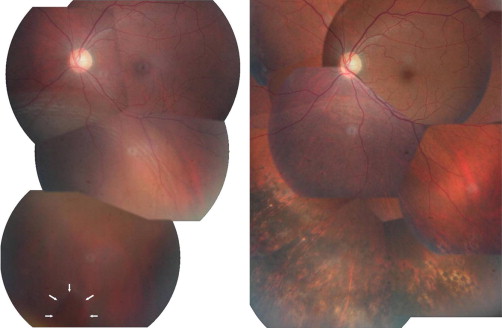
Primary anatomic success was attained in 29 (87.9%) of 33 eyes, with 23 (88.5%) of 26 eyes in the primary group and 6 (85.7%) of 7 eyes in the secondary group ( Table 2 ). In all of these eyes, the subretinal fluid (SRF) was completely absorbed and the retina reattached within 3 days after the operation. The external buckle then was removed, followed by adjunctive laser retinopexy ( Figure 2 ).
| Total (n = 33) | Primary Group (n = 26) | Secondary Group (n = 7) | |
|---|---|---|---|
| Primary anatomic success | 29 (87.9%) | 23 (88.5%) | 6 (85.7%) |
| Recurrence | 1 (3.0%) | 1 (3.8%) | 0 (0%) |
| Final anatomic success | 33 (100%) | 26 (100%) | 7 (100%) |
Of the 33 eyes, 4 (12.1%) experienced primary failure, with breaks located between 6 and 7 o’clock and an average RD extent of 7 clock hours (range, 4.5 to 12 clock hours). Three of these 4 patients were in the primary group, and they had persistent SRF for approximately 4 days (range, 3 to 5 days) after the first operation. Of these 3 patients, 2 had causative flap tears and 1 had a round hole. The fourth patient was in the secondary group and had initial success with the SRF absorbed within 3 days. However, retinal redetachment occurred 2 months after surgery because of subsequent proliferative vitreoretinopathy change without breaks. All 4 patients ultimately attained retinal reattachment after further vitrectomy, endolaser photocoagulation, and gas tamponade. One patient in the primary group had recurrent RRD with 2 new breaks supratemporally 2 years later. In this case, the retina was reattached after conventional pneumatic retinopexy. All of the patients had completely attached retinas and achieved final anatomic success at the end of the follow-up period ( Table 2 ).
Overall, the mean BCVA improved significantly at the end of follow-up (0.30 logMAR; Snellen equivalent, 6/12) compared with the preoperative BCVA (0.82 logMAR; Snellen equivalent, 6/38; P < .001). A similarly significant improvement was seen in the primary, secondary, and macula-off subgroups ( P < .05). However, the eyes with macula-on RD showed no significant change in BCVA ( P = .26; Table 3 ).



