Presbyopic Iols
Richard Tipperman
Stephen B. Lichtenstein
Many readers will be familiar with the now near-legendary story regarding Sir Harold Ridley and the development of the intraocular lens (IOL). Apparently one day Dr. Ridley was performing cataract surgery, and as had always been done, following removal of the cataractous lens the patient was left aphakic. After leaving the operating room a medical student who had been observing him asked, “When are you going to complete the surgery?” Not quite understanding what the medical student meant, Dr. Ridley asked him to explain his question, to which he replied, “Well, you removed the patient’s lens. When are you going to replace it?”
At that time no form of intraocular lens existed, and all patients received either aphakic spectacles or aphakic contact lenses. The visual disabilities associated with this form of rehabilitation were accepted as high-quality standard of care, and in fairness, for their time they were state of the art.
We are at a similar crossroads in ophthalmology where we have delivered terrific clinical results to patients with monofocal IOLs for years. However, just as intracapsular cataract extractions left patients permanently dependent on either aphakic spectacles or contact lenses, pseudophakic emmetropia leaves patients with permanently absolute presbyopia.
Present developments in IOL design have allowed anterior segment surgeons to offer their patients surgical options with significantly improved near visual function compared to standard monofocal IOLs. This chapter will review the state of the art with regard to this technology as well as future developments.
Definitions
Ophthalmologists often describe the group of IOLs that provide patients with both good distance and near vision as “multifocal IOLs”; however, a better term for this broad category is “presbyopic IOLs.” Multifocal IOLs are actually one of the large categories or subsets of presbyopic IOLs. In general, multifocal IOLs work by creating simultaneous vision wherein both the near and distance focal points are imaged on the retina at the same time. The other broad category of presbyopic IOLs are accommodating IOLs, which create a variable focus through movement or an alteration in shape of the optic.
Pseudoaccommodation is a term used to describe the ability of a lens to create a depth of focus without physically moving or changing its shape. Optical phenomena such as astigmatism, coma, and spherical aberration can all contribute to pseudoaccommodation. By definition, the near images achieved with multifocal IOLs are attained through pseudoaccommodation.
Common Concepts
Although there are differences in each of the presbyopic IOL platforms, there are also many common concepts that are critical to their clinical success. Obviously first and foremost is the successful completion of high-quality cataract surgery with creation of an appropriately sized capsulorrhexis. This not only serves the purpose of allowing the patient to achieve the best possible vision postoperatively, but it also allows for controlled centration and fixation of the IOL.
Appropriate capsulorrhexis sizing not only is necessary for the appropriate function of specific presbyopic IOL platforms, but it is also essential for accurate IOL power calculations. The most “perfect” presbyopic IOL will not function properly if the patient does not achieve the desired postoperative aim. In addition to achieving the appropriate spherical aim, it is necessary to eliminate any astigmatic component of the refractive error to achieve both the best quality vision overall and the best presbyopic function.
Surgeons performing presbyopic IOL surgery will need to treat corneal astigmatic errors with limbal relaxing incisions or even occasionally with postcataract laser vision correction.
Appropriate patient selection and education is another cornerstone of successful presbyopic IOL implementation. Various electronic and print media exist to aid with this process; however, they are not a substitute for a face-to-face discussion with the patient regarding their specific visual needs. It can be helpful to have a discussion with patients regarding not only their work and hobbies but also their expectations. Appropriate preoperative patient counseling and education ultimately makes the postoperative period easier for both the patient and the surgeon.
Presbyopic IOL Platforms
Multifocal IOLs
Within the category of multifocal IOLs there are two main subcategories: zonal refractive IOLs and diffractive IOLs. Zonal refractive IOLs create a simultaneous distance and near image by having variable radii of curvature to create different powers across the surface of the lens optic whereas diffractive IOLs use the optical principle of diffraction to create these images. Multifocal IOLs do not rely on ciliary body function or capsular contraction to create the near image.
Zonal Refractive IOLs
Array
The Array Multifocal IOL was the first FDA-approved multifocal IOL. It was a three-piece foldable silicone IOL with five distinct zones to create both distance and near vision.1 The IOL was designed so that the central zone was designed for distance vision and then the rings alternated for zones 1, 3, and 5 for distance and zones 2 and 4 for near (Fig. 14A.1). Although clinicians and their patients could achieve excellent clinical results with the Array IOL, many patients either noted significant halo and glare or could not achieve unaided functional reading vision.2 For its time the Array was a revolutionary first step in the development of presbyopic IOLs; however, presently it is of historical interest only.
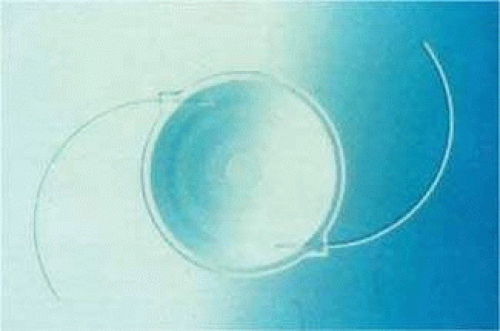 Figure 14A.1. Array IOL |
ReZoom
The ReZoom IOL is also a zonal refractive IOL. It is a three-piece hydrophobic acrylic IOL with a 6-mm optic. (Fig. 14A.2).3 The lens is designed with five concentric refractive zones: Zones 1, 3, and 5 are distant dominant whereas zones 2 and 4 are near dominant. Compared to the Array lens, there is an aspheric transition between zones, which is designed to provide intermediate vision.4
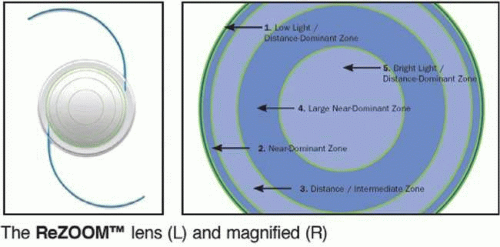 Figure 14A.2. ReZoom IOL |
Diffractive IOLs
ReSTOR Multifocal IOL
The ReSTOR IOL is a diffractive-based IOL that is available in both an aspheric and conventional design. The diffractive rings of the ReSTOR IOL are “apodized.”6
Apodization is an optical term that describes how the strength of a lens property (e.g., filter) varies over the dimension of the lens from center to periphery. Apodization allows for lenses to produce higher-quality images than nonapodized lenses.7,8 The diffractive rings are on the central 3.6 mm of the anterior optic surface, whereas the remainder of the peripheral lens optic is purely refractive and dedicated toward distance vision. (Fig. 14A.3).9,10,11 VIDEO LINK
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


