Purpose
To evaluate and compare the recurrence rates and complications between 2 therapeutic methods for primary pterygium: subconjunctival injection of mitomycin C (MMC) 1 month before bare scleral excision and conjunctival rotational flap with intraoperative MMC use.
Design
Prospective, interventional, randomized clinical trial.
Methods
setting: Institutional clinical trial in a tertiary, specialty eye hospital. study population and intervention: We included 82 eyes diagnosed with primary pterygium and randomly allocated them into 2 groups. Group A consisted of 36 eyes treated with subconjunctival injection of 0.02% MMC 1 month before bare scleral excision, and group B comprised 46 eyes that underwent conjunctival rotational flap with intraoperative 0.02% MMC for 2 minutes. Follow-up periods were at least 12 months (range, 12 to 18 months). main outcome measure: Recurrence and complication rate in each arm of study.
Results
During the 1-year follow-up, 2 cases of clinical recurrence in third and sixth month of follow-up occurred in group B (recurrence rate, 4.3%). In group A, there was no clinically significant recurrence, but 2 cases of hypovascularity and whitening of sclera at the site of pterygium excision was observed. There was no other serious complication. There was no statistically significant difference between groups for recurrence rate, mean age, sex, or pterygium area.
Conclusions
Subconjunctival injection of MMC 0.02% (0.1 ml of 0.02% solution) 1 month before bare scleral excision is a quick, easy, and safe surgical procedure and is at least as effective as conjunctival rotational flap with intraoperative MMC for 2 minutes.
Pterygium is a fibrovascular overgrowth of conjunctival tissue encroaching on the cornea from limbus toward the center that resembles an insect wing. Overall prevalence of the disease is 5% to 15% and increases in tropical areas, which may suggest the pivotal role of ultraviolet (UV) light as the cause of the disease. UV exposure is widely accepted to be the single most important etiologic factor in pterygium pathogenesis. UV light may produce damage to the cellular DNA, RNA, and extracellular matrix and may induce expression of cytokines and growth factors important in the development of pterygium. However, the exact pathogenesis of pterygium remains uncertain. Other mechanisms have been proposed, including the role of cellular immunity through pathways involving cyclooxygenase-2 and matrix metalloproteinases. Another proposed mechanism focuses on the role of vascular proliferation in the development of pterygium. Generally, pterygium can be considered a proliferative, invasive lesion with focal limbal breakdown associated with excessive UV exposure.
There are several indications for pterygium excision, such as decreased visual acuity resulting from visual axis involvement, tear film break-up, and/or irregular eye movement limitation; eye irritation and discomfort; inability to wear contact lenses; difficulty in performing refractive surgery; uncertainty about the diagnosis; and cosmetic concerns.
Many different surgical techniques have been tried for pterygium removal with variable success rates. The most convenient technique is simple excision of pterygium. However, bare sclera technique of pterygium excision without adjuvant therapies (chemotherapy and radiation) has recurrence rates of 29.7% to 88.9%. In different studies, the adjuvant therapy with different concentrations (0.01% to 0.4%) of mitomycin C (MMC) has been associated with a 2.7% to 42.9% decrease in recurrence rate. Concerns about the sight-threatening side effects of adjuvant therapy have made alternative therapeutic measures as a popular research topic. In an attempt to decrease ocular surface exposure to intraoperative antimetabolites, subconjunctival injection of MMC has been proposed with a recurrence rate of 6%. Recently, combination of intraoperative MMC and rotational conjunctival flap has been reported as a highly efficacious treatment for pterygium, with a reported recurrence rate of 3%. However, differences in patient inclusion criteria and the noncomparative nature of these studies have made conclusive decisions about the choice procedure difficult, if not impossible. The purpose of this study was to compare the 2 recently introduced surgical approaches (i.e., preoperative subpterygeal MMC injection with later bare sclera excision and intraoperative MMC application with conjunctival rotational flap) in terms of complications and recurrence rates.
Methods
This was a randomized clinical trial conducted on all eligible patients referred with a diagnosis of primary pterygium to a tertiary referral eye hospital in northeastern Iran (Khatam Anbia Eye Hospital) from October 2007 through June 2009. Pregnant or breast-feeding women and patients with a history of previous ocular surgeries; ocular diseases such as glaucoma, herpetic keratitis, and trachoma; or any autoimmune disease were excluded.
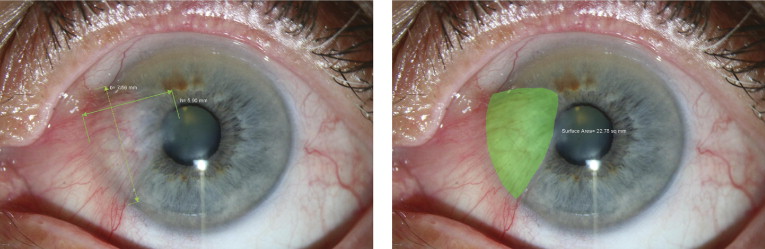
Patients were allocated randomly into 2 groups. Randomization was carried out using envelopes containing random digits. Group A patients (envelopes with odd digits) underwent subconjunctival injection of 0.02% MMC 1 month before bare scleral excision. Group B patients (envelopes with even digits) underwent conjunctival excision with a rotational flap from the superior conjunctiva and intraoperative 0.02% MMC. A comprehensive ophthalmic examination, including best-corrected visual acuity testing, slit-lamp examination, Goldmann applanation tonometry, and fundus examination, was carried out for all participants. Assuming a pterygium to have a triangular shape, corneal surface area covered by pterygium, a , was estimated by multiplying maximum width, b , at pterygium base to half of its length, h : a = bh /2. We found this approximation to be a user-friendly approach with acceptable accuracy. We checked the precision of the method with the Measuring Tool of Adobe Acrobat software (version 9 Pro Extended; Adobe System Incorporated, Burlington, New Jersey, USA). As evident in Figure 1 , the surface area calculated with the equation is in close approximation to the actual surface area calculated by the software.
All of the operations were performed by 2 of the authors (H.K. and M.E.R.), both skillful in pterygium surgery with a surgical experience of more than 15 years. In group A, the surgery was performed in 2 stages: in the first, office-based stage, the conjunctiva was anesthetized with instillation of tetracaine eye drops followed by local injection of lidocaine 2%. After waiting for 5 minutes to achieve sufficient anesthesia, and under the slit-lamp viewing, 0.1 mL 0.02% MMC solution (Mitomycin-C Kyowa; Kyowa Hakko Kogyo Co, Ltd, Tokyo, Japan) was injected sublesionally via a 30-gauge insulin syringe and along the limbus at the site of pterygium overgrowth over the cornea. A cotton-tip applicator then was used to compress the needle entry site to prevent MMC egress on the ocular surface. In the end, and in a recombinant position, the eye was irrigated copiously with at least 30 mL balanced salt solution. After injection, all patients received 0.5% chloramphenicol (Sina Darou, Tehran, Iran) and 0.1% betamethasone (Sina Darou) eye drops every 6 hours for 1 week. Follow-up visits were scheduled for 1 day, 1 week, and 1 month later. In the second stage, 1 month after the initial injection, bare scleral excision of pterygium was performed, as has been described previously. The eye was pressure patched and topical medications were restarted at the first postoperative day. At the second postoperative visit 1 week later, chloramphenicol eye drop was discontinued and betamethasone was substituted with topical 0.1% fluorometholone (Fluocort; Sina Darou) every 6 hours for 1 month.
In group B, with a modified Pico technique, the patients underwent pterygium excision after local anesthesia with topical tetracaine and local subconjunctival injection of lidocaine 2%. Pterygium was grasped at the limbus and avulsed from corneal surface with a muscle hook. A Wescott scissors was used to remove the pterygium body, and the corneal and sclera surfaces were polished with a no. 15 Bard-Parker blade. Minimal cautery was performed to control bleeding, and 0.02% MMC solution was applied to the bared scleral bed for 2 minutes, followed by copious irrigation of the ocular surface with at least 30 mL balanced salt solution. After releasing the superior conjunctiva, a conjunctival flap was rotated and fixed over the bare sclera using 8-0 Vicryl (Surgicryl; SMI AG, Hünningen, Belgium) stitches to cover the resection site, except a 2-mm zone adjacent to the limbus. Finally, topical ointments of erythromycin and hydrocortisone were applied and the eye was pressure patched. On the first postoperative day, 0.5% chloramphenicol and 0.1% betamethasone eye drops were administered every 6 hours for 1 week. The patients were visited 1 week later, and fluorometholone eye drops were administered (every 6 hours for 1 month) instead of betamethasone. If not degraded, the Vicryl sutures were removed at the third postoperative week.
In both groups, follow-up visits were scheduled 1, 3, 6, 9, and 12 months after surgery, and a complete set of ophthalmic examinations was repeated with special focus on probable complications such as dellen formation, persistent corneal epithelial defect, recurrence, and scleral necrosis. After surgery, an overgrowth of fibrovascular tissue over the corneal surface of more than 1.0 mm was considered a recurrence, as has been described previously. One of the authors (M.F.G.), blinded about the study groups, performed all ophthalmic examinations; however, because of apparent differences between the ocular surface appearance of the study groups, especially in the early phase, there was practical limitation to the blinding procedure at the postoperative first month visit.
In patients with bilateral pterygium requiring surgical intervention, a similar procedure was performed on both eyes; however, only 1 eye per subject was included randomly in the final analysis. Patients without regular follow-up were omitted from the study. Because some of participants were Afghani refugees, recruitment for follow-up examination was impossible after the first postoperative visits. We could assume that they had no major complication or recurrence; however, to be precise, we did not include them in the final analysis. The complication rate was compared between the 2 groups using chi-square and Fisher exact tests. Intergroup changes for continuous parametric variables were evaluated by the unpaired Student t test. All statistical analyses was performed with SPSS version 15 (SPSS Science Inc, Chicago, Illinois, USA). For all measurements, a 2-tailed test was used, and the statistical significance level was set at P < .05.
Results
Eighty-two eyes of 82 patients were enrolled in the study, including 36 eyes in group A and 46 eyes in group B. Initially, group A comprised of 66 eyes; however, 18 eyes were excluded because of incomplete follow-up and 12 eyes were omitted randomly in bilateral cases, leaving 36 eyes of 36 patients for the final analysis. Group B included 51 patients; however, 7 eyes of 5 patients with incomplete follow-up visits and 4 randomly selected eyes in bilateral cases were excluded from the final analysis. Finally, 46 eyes of 46 patients were evaluated in group B.
There were 18 (50%) and 24 (52.2%) females in groups A and B, respectively ( P = .840). The mean age of all patients was 48.48 ± 13.67 years (range, 20 to 80 years). The mean ages in groups A and B were 49.37 ± 13.61 years and 47.80 ± 13.82 years, respectively ( P = .612).
The estimated pterygium area over the cornea in group A was 11.38 ± 5.58 mm 2 (range, 4.83 to 26.52 mm 2 ; 95% confidence interval, 9.50 to 13.27). This value in group B was 10.44 ± 4.03 mm 2 (range, 4.41 to 19.12 mm 2 ; 95% confidence interval, 9.24 to 11.63; P = .375).
One month after surgery, 17 patients (47.2%) in group A and 23 patients (50%) in group B reported foreign body sensation ( P = .803). At this time, 4 cases (11.1%) in group A and 7 cases (15.2%) in group B had red eye ( P = .419). In the following months, there was neither clinically or statistically significant difference in red eye or foreign body sensation between the groups. No case of complication such as dellen formation, persistent corneal epithelial defect, corneal or sclera melting, or infection was noted during 1-year follow-up.
In group A, 3 months after the surgical procedure, we found a case with fibrovascular overgrowth over the cornea measuring 0.8 × 0.9 mm; however, considering our definition for recurrence of at least 1 mm progression of fibrovascular tissue over the cornea, this situation was not clinically significant. A case with a small conjunctival cyst near the caruncle was found in group A, which was clinically unremarkable. In group A, 2 patients had whitening of sclera and hypovascularity at the site of excision ( Figure 2 ), which persist at last follow-up (12 months). In a young patient, this was cosmetically unpleasant (a similar whitening developed in the opposite operated eye, too; however, only 1 eye was selected randomly for the analysis).



