Purpose
To examine the distribution of intraocular pressure (IOP) and its related systemic and ocular biometric factors in a population-based study in a southwestern island of Japan.
Design
Cross-sectional, population-based study.
Methods
All residents of Kumejima Island, Japan, located in southwestern Japan (eastern longitude, 126 degrees 48 minutes and northern latitude 26 degrees 20 minutes), 40 years of age and older were asked to undergo a comprehensive questionnaire and ocular examination, including measurement of IOP with Goldmann applanation tonometry.
Results
Of the 4632 eligible residents, 3762 (81.2%) underwent the examination. In 2838 nonglaucomatous subjects from whom reliable measurements of IOP were obtained, the mean IOPs ± standard deviation in all, men, and women were 15.1 ± 3.1 mm Hg (n = 2838), 15.2 ± 3.1 mm Hg (n = 1450), and 15.1 ± 3.0 mm Hg (n = 1388), respectively, with no significant intersex difference ( P = .63). Multivariate regression analysis demonstrated that higher IOP was significantly correlated with younger age ( P < .001), higher body mass index ( P < .001), higher systolic blood pressure (P < .001), history of diabetes mellitus ( P = .001), thicker central corneal thickness ( P < .001), steeper corneal curvature ( P < .001), and longer axial length ( P < .018), but not with anterior chamber depth and the Shaffer angle width grade.
Conclusions
Younger age, higher body mass index, higher systolic blood pressure, diabetes, thicker central corneal thickness, and steeper corneal curvature were significantly correlated with higher IOP. The present results confirm that IOP is associated with systemic and ocular biometric factors and may define specific subgroups most likely to have an elevated IOP.
Intraocular pressure (IOP) is generated by the flow of aqueous humor against resistance and is necessary for the proper shape and optical properties of the globe. Regulation of IOP is a complex physiologic trait that depends on the production of aqueous humor, resistance to aqueous humor outflow, and episcleral venous pressure. From a clinical point of view, IOP is a major risk factor for glaucoma, and thus the correlation of various systemic and ocular factors with IOP has been investigated. The results vary in different races and regions. For example, although several population-based studies have shown that IOP and age are 2 major risk factors of glaucoma, the relationship between IOP and age varies in different populations. Studies conducted in Western countries, Iran, and Barbados show a positive correlation between IOP and age. However, studies conducted in East Asia report a statistically significant decrease in IOP with increasing age. Considering these discrepancies in relation to IOP and other variables, it is important to investigate the distribution of IOP and its correlating factors in various populations. Furthermore, as ocular biometric factors possibly relating with IOP, only corneal curvature, central corneal thickness (CCT), and refraction have been taken into consideration in previous studies. The present study examined the distribution of IOP and its relating systemic and ocular biometric factors in ophthalmologically normal participants of a population-based study carried out in a southwestern island of Japan. In addition to CCT, corneal curvature, and refraction, systemic factors, such as age, sex, blood pressure, and body mass index (BMI), were included and ocular biometric factors, such as anterior chamber depth, angle width, and axial length, were taken into account.
Methods
Study Population
A population-based epidemiologic survey of ocular diseases was conducted in residents of Kumejima Island 40 years of age or older. Kumejima is a 63.2-km island located in the southwestern part of Japan (eastern longitude of 126 degrees 48 minutes and northern latitude of 26 degrees 20 minutes) west of the main island of Okinawa and has a population size of approximately 9000, with most residents originating from the Okinawa prefecture. The weather is warm and humid, with mean daily temperatures of 22.7 C and yearly total rainfall of 2138 mm. This study was conducted between May 1, 2005, and August 31, 2006. According to the official household registration database, Kumejima had 5249 residents 40 years of age or older in 2005. After excluding residents who died, moved, or could not be located in Kumejima during the study period (n = 617), 4632 residents were eligible for the study. All of these residents were asked by letter, telephone, or both to undergo the examinations held at the public hospital of Kumejima. Home visits and examinations were performed for inpatient, paralyzed, and disabled residents.
Examinations and Glaucoma Diagnosis
After weight, height, and brachial blood pressure measurements were obtained, a structured questionnaire was administered that included questions about occupation, health history, surgery and trauma history, smoking habit, history of outdoor work, and use of hats and sunglasses. Weight and height were determined with an analog stadiometer and a digital weight scale, respectively. Blood pressure was measured with an electronic sphygmomanometer (ES-P1000; Terumo Corp, Tokyo, Japan) in a sitting position after approximately a 5-minute rest.
A detailed screening ophthalmic examination was performed by an experienced examiner and ophthalmologist (S.A.) and included uncorrected and best-corrected visual acuity, refraction, slit-lamp examination of the anterior segment, IOP, gonioscopy, CCT, anterior chamber depth, axial length of the eye, ophthalmoscopy, photography of ocular fundus, and visual field. Corneal curvature was measured using an autorefractometer (ARK-730; Topcon, Tokyo, Japan). Mean corneal curvature was calculated with the steepest and the flattest corneal curvatures in each eye. IOP was measured 3 times using a Goldmann applanation tonometer under topical anesthesia and the median value was adopted. CCT was measured with specular microscopy (SP-2000; Topcon), with which CCT measurement was confirmed to be highly correlated with that obtained using ultrasound pachymetry in a previous study. Anterior chamber depth and axial length of the eye were measured with the IOL Master (Carl Zeiss Meditec, Dublin, California, USA). Digital sequential stereoscopic color fundus photographs (30 degrees and 45 degrees) were obtained using a nonmydriatic ocular fundus camera system (Image Net TRC-NW7; Topcon). In the screening examination, examinations that did not require direct eye contact, including tests of refraction, visual acuity, and specular microscopy; IOL Master, fundus photography, and slit-lamp examination were performed first. IOP measurement in both eyes followed by gonioscopy in both eyes with a Goldmann 2-mirror gonioscopy lens were performed last. In static gonioscopy, the angle width first was determined subjectively according to the (original) Schaffer grading system and simultaneously the visibility of the ciliary band, scleral spur, trabecular meshwork, and Schwalbe line was evaluated based on the modified Shaffer grading (South East Asia Glaucoma Interest Group website; available at http://www.seagig.org/pdf/APGGuidelinesNMview.pdf ; accessed May 20, 2008). If necessary, compression gonioscopy was also was performed. In the statistical analyses below, Shaffer angle width was averaged in the superior, inferior, temporal, and nasal quadrants. The visual fields were evaluated with frequency doubling perimetry using the screening program C-20-1 (Carl Zeiss Meditec). These measurements were performed first in the right eyes.
When participants could not visit the hospital, ophthalmologists visited their homes and performed the examinations, including the slit-lamp examination with a hand-held slit lamp (SL-15; Kowa, Tokyo, Japan), IOP measurements with a Perkins tonometer (JFC Sales Plan Co, Tokyo, Japan) or hand-held tonometer (Tono-Pen XL; Bio-Rad Laboratories, Hercules, California, USA), and indirect and direct ophthalmoscopy (BS-II and BXα-13; Neitz, Tokyo, Japan).
Participants were referred for definitive examinations if they were suspected of having ocular disorders or related conditions or if at least 1 eye met 1 or more of the following criteria: corrected visual acuity worse than 20/30; abnormal findings during the slit-lamp examinations or on fundus photographs; IOP of more than 19 mm Hg; angle width grade of 2 or less of the van Herick method; findings in the optic disc, retina, or both suggestive of glaucoma or other ocular diseases; and at least 1 abnormal test point in the visual field test. The definitive examination included slit-lamp examination, gonioscopy, optic nerve head and posterior pole fundus evaluation with a Goldmann 2-mirror lens, applanation tonometry, and visual field testing with the Humphrey Field Analyzer central 24-2 Swedish interactive threshold algorithm standard program (Carl Zeiss Meditec). Unless gonioscopy revealed an occludable angle, the pupil was dilated to observe the ocular fundus in detail by indirect ophthalmoscopy. When the angle was thought to be occludable, the same examinations were carried out with undilated pupils.
A panel of 6 glaucoma specialists determined final glaucoma diagnosis based on clinical records obtained through all the examinations. The presence of glaucoma was diagnosed according to the results of evaluation of the optic disc and retinal nerve fiber layer and the visual field. Because the distribution of the cup-to-disk ratio, cup-to-disk ratio asymmetry, and IOP in the Kumejima population was not known before the present study, the criteria for glaucoma diagnosis were based on the criteria of the International Society of Geographical and Epidemiological Ophthalmology criteria as follows. First (category 1), the eye was diagnosed as having glaucoma when the vertical cup-to-disc ratio of the optic nerve head was ≥ 0.7, the rim width at the superior portion (from the 11- to 1-o’clock position) or inferior portion (from the 5- to 7-o’clock position) was ≤ 0.1 of the disc diameter, the difference of the vertical cup-to-disk ratio was ≥ 0.2 between both eyes, or a nerve fiber layer defect was found, and the hemifield-based visual field abnormality was compatible with the optic disc appearance or nerve fiber layer defect. Second (category 2), when the visual field test was not reliable or available, the diagnosis was obtained when the vertical cup-to-disk ratio was ≥ 0.9, the rim width at the superior portion (from 11- to 1-o’clock position) or inferior portion (from 5- to 7-o’clock position) was ≤ 0.05, or the difference of the vertical cup-to-disk ratio was ≥ 0.3 between both eyes. Third (category 3), when a participant could not complete the visual field testing and his or her optic disc was not visible, the diagnosis was made if the visual acuity was ≤ 20/400 and the IOP was higher than the 99.5 percentile value for Japanese, that is, ≥ 23 mm Hg, or if the participant had a history of glaucoma surgery. In glaucoma diagnosis, anomalous discs, including tilted discs, were excluded carefully.
Data Analysis
All data were preserved at the University of Ryukyus and University of Tokyo. Data analyses were performed using SPSS software version 15.0J for Windows (SPSS Japan Inc, Tokyo, Japan). Eyes in which reliable IOP measurement with a Goldman applanation tonometer was not performed and eyes having eye diseases that could affect IOP such as glaucoma and uveitis were excluded from the analysis ( Table 1 ). The relation between IOP and systemic or ocular factors was assessed using the Pearson correlation analysis and analysis of variance (ANOVA) to adjust for age and gender. Multivariate regression analysis with stepwise selection of explaining variables (probability of F to enter, ≤ 0.050; probability of F to remove, ≥ 0.100), including age, BMI, systolic and diastolic blood pressure, self-reported history of diabetes mellitus, current habit of smoking, corneal curvature, CCT, anterior chamber depth, axial length, average Shaffer angle width grade, also was carried out. Because the interviews regarding educational history, current income, and other socioeconomic factors were not permitted by the ethical committee according to a national law regarding personal information, these factors could not be included in the explanatory variables. Because refraction in normal eyes can be roughly approximated using corneal curvature and axial length, spherical equivalent of refraction was not incorporated into the multivariate regression analysis. Data are shown as mean ± standard deviation unless otherwise specified.
| Reasons | Right Eyes | Left Eyes |
|---|---|---|
| Screened in own homes | 192 | 192 |
| Phthisis or prosthesis | 5 | 6 |
| Difficulties in measuring IOP | 45 | 43 |
| History of intraocular surgeries including laser iridotomy | 564 | 565 |
| Glaucoma | 76 | 75 |
| Uveitis | 5 | 7 |
| Pterygium (severe) | 17 | 9 |
| Corneal opacity | 14 | 12 |
| Strabismus (moderate or severe) | 3 | 5 |
| Total | 924 | 914 |
Results
Of the 4632 eligible residents, 3762 (81.2%) underwent the examination. The 3762 participants were younger than the 870 nonparticipants (59.1 ± 14.9 years vs 61.8 ± 14.0 years; P < .001, unpaired t test), and women were more common among the participants (male-to-female ratio, 1833:1929 vs 555:315; P < .001, chi-square test).
Of the 7524 eyes (3762 participants), 924 right eyes and 914 left eyes were excluded ( Table 1 ). As a result, 2838 right eyes and 2848 left eyes of 3045 participants (both eyes were eligible in 2641 subjects, only the right eye was eligible in 197 subjects, and only the left eye was eligible in 207 subjects) were included in the analysis.
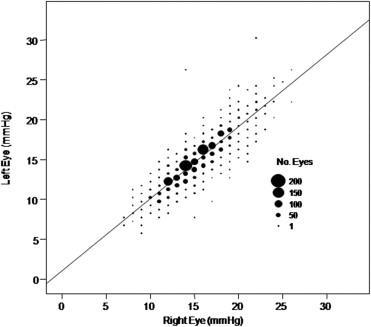
Among the 2641 subjects in whom both eyes were eligible, the mean IOP in the right eyes was 15.1 ± 3.1 mm Hg (95% confidence interval, 15.0 to 15.2) and that in the left eye was 14.8 ± 3.1 mm Hg (95% confidence interval, 14.6 to 14.9); the difference between right and left eyes was significant ( P < .001, paired t test). Because IOP in the right eyes and left eyes was strongly correlated ( R = 0.885; P < .001; Figure 1 ) and the results in the left eyes were similar to those in the right eyes, the results in the right eyes are shown below.
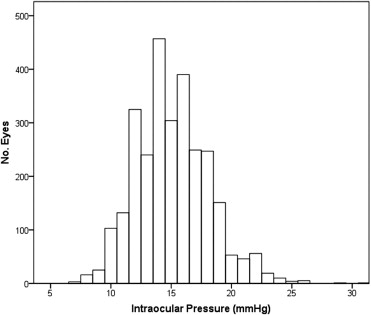
The demographic data from the 2838 participants in which the right eyes were eligible are shown in Table 2 . The mean IOP in all participants, men, and women was 15.1 ± 3.1 mm Hg (n = 2838; Figure 2 ), 15.2 ± 3.1 mm Hg (n = 1450), and 15.1 ± 3.0 mm Hg (n = 1388), respectively, with no significant intergender difference after adjusting for age ( P = .632, ANOVA). Mean IOP in the 253 participants who had a self-reported history of diabetes was significantly higher after adjusting for age and gender than that in the 2585 participants who did not report a history of diabetes (15.8 ± 3.1 mm Hg vs 15.0 ± 3.0 mm Hg; P < .001, ANOVA). The mean IOP in the 1100 participants with a smoking habit was not significantly different from that in 1738 participants who did not smoke (15.1 ± 3.1 mm Hg vs 15.1 ± 3.0 mm Hg; P = .835, ANOVA).
| Parameters | Mean ± Standard Deviation |
|---|---|
| Age (years) | 58.4 ± 12.5 |
| Height (cm) | 155.9 ± 9.2 |
| Weight (kg) | 61.4 ± 11.8 |
| Body mass index | 25.1 ± 3.6 |
| Systolic blood pressure (mm Hg) | 141.3 ± 24 |
| Diastolic blood pressure (mm Hg) | 79.1 ± 13.4 |
| Intraocular pressure (mm Hg) | 15.1 ± 3.1 |
| Spherical refraction (diopters) | 0.02 ± 1.86 |
| Mean corneal curvature (diopters) a | 44.2 ± 1.4 |
| Central corneal thickness (μm) a | 510 ± 34 |
| Anterior chamber depth (mm) a | 3.10 ± 0.38 |
| Axial length (mm) a | 23.43 ± 0.93 |
| Shaffer angle width grade a , b | 3.0 ± 0.8 |
a Data are from the right eyes.
b Shaffer angle width was averaged in the superior, inferior, temporal, and nasal quadrants.
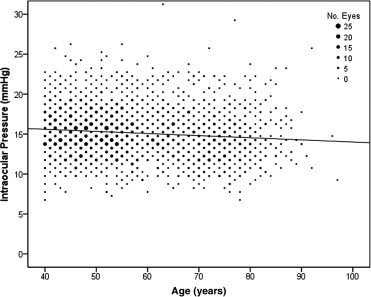
With regard to the results of Pearson correlation analysis, older age was significantly correlated with lower IOP ( Figure 3 ; P < .001). After adjusting for age and gender, higher BMI, higher systolic and diastolic blood pressure, steeper corneal curvature, and thicker corneal curvature were significantly correlated with higher IOP (all P < .001), whereas height, spherical refraction, anterior chamber depth, axial length, and Shaffer angle grading were not (all P > .065; Table 3 ). The correlations were basically the same in the younger and older age groups, except for spherical equivalent and Shaffer grading, both of which were significantly correlated with IOP only in the younger age group.
| Parameters | All (N = 2838) | Younger Age Group (n = 1639) | Older Age Group (n = 1199) |
|---|---|---|---|
| Age | –0.11 ( P < .001) a | –0.02 ( P = .284) a | –0.09 ( P = .001) a |
| Height | –0.035 ( P = .065) | –0.07 ( P = .003) | 0.02 ( P = .504) |
| Weight | 0.12 ( P < .001) | 0.11 ( P < .001) | 0.13 ( P < .001) |
| Body mass index | 0.16 ( P < .001) | 0.17 ( P < .001) | 0.13 ( P < .001) |
| Systolic blood pressure | 0.23 ( P < .001) | 0.24 ( P < .001) | 0.21 ( P < .001) |
| Diastolic blood pressure | 0.19 ( P < .001) | 0.19 ( P < .001) | 0.17 ( P < .001) |
| Spherical refraction | –0.032 ( P = .091) | –0.06 ( P = .009) | –0.01 ( P = .782) |
| Mean corneal curvature b | 0.08 ( P < .001) | 0.08 ( P = .002) | 0.08 ( P = .004) |
| Central corneal thickness b | 0.23 ( P < .001) | 0.22 ( P < .001) | 0.24 ( P < .001) |
| Anterior chamber depth b | 0.004 ( P = .833) | 0.04 ( P = .142) | –0.03 ( P = .238) |
| Axial length b | 0.005 ( P = .792) | 0.06 ( P = .02) | –0.04 ( P = .143) |
| Shaffer grade b , c | 0.006 ( P = .760) | –0.07 ( P = .003) | 0.02 ( P = .504) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


