Preoperative Evaluation and Facial Analysis in Facial Plastic Surgery
Andrew Winkler
Justin M. Wudel
CONCEPT OF BEAUTY AND DEFORMITY
Western civilization portrays facial beauty as flawless, young skin with ideal facial contours. Youth and beauty are pervasive in all forms of media, highlighting their significance to our culture and to humans in general (1). The value that our society places on beauty has lead to innumerable methods of enhancing one’s attractiveness, including cosmetic surgery. Today, the desire to change one’s appearance is considered a sufficient indication for surgery, whether or not a true “deformity” is present. The continual growth in the number of cosmetic procedures performed each year reflects the public’s rapidly growing acceptance of cosmetic surgery as a means of self-improvement.
The physician and patient usually share a perception of deformity and the correction needed. Some patients, however, perceive an abnormality not readily apparent to other people. A significant difference between the perceived deformity and the surgeon’s assessment of the feature raises warning flags that may warrant further evaluation. This chapter aids in defining what does and does not constitute deformity and how to elucidate whether a patient’s requests are within normal limits. Psychiatric conditions that may lead to a disagreement in facial assessment between patient and surgeon are also discussed. The absolute numeric values presented in this chapter allow the surgeon to determine whether or not a feature is proportionate. However, facial features must also form a harmonious union when observed together. Harmony refers to the mind’s interpretation of the facial relationships based strictly on visual observation (2). For facial beauty to exist, the proportions and architecture of the face must form a balance that is visually pleasing. When the major aesthetic masses of the face (nose, lips, ears, eyes, etc.) are individually proportionate, they are more likely to harmonize with each other to yield an aesthetically pleasing facial appearance. However, disproportionate features may also harmonize with one another, even though the feature itself falls outside of what is considered normal. Consequently, beauty is to a degree in the eye of the beholder, and aesthetic facial analysis remains a partially subjective exercise.
INITIAL CONSULTATION
Establishing a Relationship
The primary goal of the preoperative interview is to establish effective communication in order to obtain an understanding the patient’s perception of the defect, the patient’s motivations, and the patient’s expectations from surgery (3). During the interview, the patient’s thoughts and feelings about the area of concern are explored. This provides an opportunity to educate the patient about the details of potential surgery and what outcomes may be realistically achieved. The preoperative interview is also an opportunity to a review the medical history to identify conditions that may preclude surgery. Spending time with potential medical issues improves trust and rapport and may reveal issues needing further evaluation prior to undergoing elective surgery. A surgeon’s mastery of the relationship-building phase of the interview results in improved patient satisfaction, reduced legal liability, and better surgical outcomes (4, 5).
Preoperative Assessment
A commonsense approach to selecting candidates for surgery greatly reduces the chance of encountering an unhappy patient (6). In the preoperative interview, the surgeon seeks answers to the following questions:
What are the patient’s expectations?
Are the expectations realistic and reasonable?
Do I have the ability to fulfill these expectations?
Can the patient be satisfied?
TABLE 170.1 RED FLAG SYMPTOMS. PATIENTS EXHIBITING “RED FLAGS” MAY WARRANT FURTHER INVESTIGATION | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
Many tools are available to aid in obtaining this information. The Sensitization, Aesthetic self-assessment, peer Group comparison and Avoidance behaviors (SAGA) tool helps to uncover patients’ understanding of normal, their perception of deformity, and its impact on them (7). Sensitization refers to the point at which the patient becomes aware of and bothered by a deformity. The impetus for sensitization may be self-induced (intrinsic) or the result of extraneous remarks or teasing (extrinsic). Alternatively, the patient may not be sensitized to a deformity and may be requesting surgery to please someone else, a red flag symptom (Table 170.1).
The second concept evaluated by the SAGA tool is aesthetic self-assessment. This is the patient’s private evaluation of the concerning feature in a mirror. Simply inquiring about self-assessment builds rapport and reassures the patient that this is normal behavior. The self-assessment also gives an impression of the desired improvements and whether these expectations are realistic.
Peer group comparison gives insight into patient sensitization as well as their reaction to the deformity. A patient sensitized to a feature will scrutinize others in society (7). The patient desiring to appear like that of a particular movie star reveals unrealistic expectations, and such patients are likely to blame the surgeon for perceived poor results. The patients’ ability to accept the surgical result is highly correlated with the degree to which they are prepared by their surgeon. Unrealistic expectations must be discussed prior to undergoing surgery (8).
Avoidance behaviors examine the techniques and strategies used by the patient to camouflage or conceal their imperfections. This may include makeup, clothing, or a hairstyle used to cover up or draw attention away from the featured complaint. Avoidance behaviors should resolve with surgery and may provide an objective measure of success postoperatively.
The experienced surgeon develops wariness for patients who create a sense of uneasiness. Situations that raise caution flags include a history of having sued another surgeon, extreme demands of support staff, or evidence of “doctor-shopping” in search of someone who will perform the desired surgery. Such patients should be approached with extreme care and often require further evaluation (Table 170.1).
PSYCHOPATHOLOGY IN THE AESTHETIC PATIENT
It was not long ago that patients seeking aesthetic surgery were assumed to have deeply seated psychological issues. In 1960, Jacobson et al. (9), suggested that most cosmetic surgery patients required psychological evaluation because psychiatric problems were almost certainly present. As cultural norms have evolved, the level of concern about physical appearance that was once deemed psychologically abnormal is now acceptable and it is rare for a patient to require preoperative psychiatric evaluation. The rate of psychopathology in cosmetic surgery patients today approaches that of the general population. Nevertheless, only a small percentage of the population actively seeks surgery despite a continual increase in popularity. This is due to personality characteristics that differentiate those who seek cosmetic surgery from those who do not (4, 10). On the extreme end of the personality spectrum are patients with diagnosable psychiatric conditions. The following section describes important pathologic conditions to consider during the initial consultation.
Depression
Traditionally, patients carrying a diagnosis of depression were rejected for facial cosmetic surgery as it was feared this would trigger deeper depression (11). In a study from 1960, patients with late-onset and prolonged depression after cosmetic procedures exhibited a causal relation between surgery and depression. This group of patients received support in the immediate postoperative period that was initially satisfying. As the sought-after attention waned, however, the patients realized that surgery had not fulfilled their desires, and they became more depressed. While a diagnosis of depression is not a contraindication to surgery, there remains a risk of depression intensifying following surgery. We now know that almost half of aesthetic surgery patients display clinically apparent postoperative depression, even with a good outcome (11, 12). Despite this finding, Moss and Harris (13) demonstrated a significant improvement in patient’s postoperative Beck Depression Inventory score following cosmetic surgery in comparison to their preoperative scores. It is generally accepted that patients with a preoperative diagnosis of depression can undergo cosmetic surgery without fear of long-term intensification of their symptoms, although coordination between the surgeon and psychiatrist yields the best results.
Personality Disorder
Personality disorders are psychiatric conditions in which a person’s behaviors, emotions, and thoughts are markedly different from that of their culture, causing serious problems with relationships and work. Personality disorders are the most common psychopathology seen in patients seeking cosmetic surgery (14). These patients are manipulative, demanding, and difficult to please. Of all personality disorders, narcissistic and histrionic personality disorders are most commonly encountered by facial plastic surgeons (15). Although the overall prevalence of narcissistic personality disorder in the general population is 1%, up to 25% of patients who present to a plastic surgery practice display hallmarks of the diagnosis, including unexplained grandiosity accompanied by a need for admiration (14, 16). Similarly, although the incidence of histrionic personality disorder in the general population is 1.8%, up to 10% of cosmetic surgery patients have this condition, marked by attention-seeking behavior, excessive emotionality, and sexual forwardness (15, 16). A third personality disorder to consider is borderline personality disorder (BPD). People with BPD are uncertain about their identity, and as a result their interests and values change rapidly. These patients perceive their environment in terms of extremes, leading to rapidly shifting feelings and unstable relationships (16). The encounter with a patient who has a personality disorder can be one of frustration and aggravation. Nevertheless, an appropriate doctor-patient relationship must be established. If the surgeon is not confident that this relationship can be maintained or the patient will not cooperate, surgery should not be performed.
Body Dysmorphic Disorder
One of the most difficult challenges facing a plastic surgeon occurs when there is disagreement with a patient regarding the degree of deformity. While it is not uncommon to encounter patients who would like to have minor deformities corrected or improved, it is important to recognize patients who fall outside of the normal spectrum. The extreme example of this is body dysmorphic disorder (BDD), a condition characterized by the unhealthy obsession with one or more body parts (16). Patients with BDD have a preoccupation with some slight or perceived flaw in their physical appearance. These individuals spend an excessive amount of time thinking about their personal appearance and methods to change it. BDD is estimated to occur in approximately 1% of the general population, but the incidence is up to 16 times higher in patients desiring plastic surgery (17). When a patient demonstrates profound emotional distress and behavioral impairment out of proportion to the actual defect, the plastic surgeon is wise to refer the patient for psychiatric evaluation. The mainstay of treatment for the behavioral components of BDD is cognitive behavior therapy (18). BDD is a somatoform disorder that cannot be effectively treated with surgery and therefore these patients are not surgical candidates. BDD patients are more likely to move to litigation, and may even threaten physical violence.
FACIAL ANALYSIS
History
The desire to identify ideal facial aesthetics dates to antiquity. Greek artists sought to identify ideal facial proportions and began to formally analyze beauty. The classical Greek canons of facial balance that were developed consequently influenced anatomic scholars of the Renaissance period, and many of these form the foundation of facial analysis today.
Ricketts (19) supported the Greek concept that facial attractiveness is related to the repetition of proportions throughout the face. The ideal or “divine” proportion equates to the mathematical ratio of 1:1.618 (phi), which was believed to be the rate of mathematical progression most pleasing to the eye. The ratio refers to the point along a line at which the ratio of the smaller portion to the larger portion is the same as the ratio of the larger portion to the original line (Fig. 170.1) (20).
Farkas et al. (21) performed detailed anthropometric studies of different ethnic populations to assess the validity of the classical Greek canons for beauty and determined multiple “normal” values for various facial proportions. Measurement and memorization of normal values is cumbersome and quickly becomes impractical for everyday use by aesthetic surgeons.
Modern science defines beauty as a biologic and crosscultural concept of attractiveness. In one study (22), infants preferred looking at aesthetically pleasing adult faces. Other studies (23) note a preference for symmetry in facial architecture (24, 25). Another (26) found that test subjects preferred a composite of attractive faces to a composite of average faces, which was consistent across ethnic boundaries. Ethnic differences in aesthetic ideals exist, however, and must be considered during facial analysis to avoid inappropriate “Westernization” of ethnic features (27, 28, 29, 30, 31).
Defining Terms
The face is a complex balance of multiple aesthetic units that when taken together produces a unique appearance. Facial analysis uses standardized points to determine
relationships between various aesthetic masses, and to determine the proportions of each feature individually. The following tables define standard reference points used in facial analysis (Tables 170.1 and 170.2, Fig. 170.2). Using these standard points, reference angles are constructed to analyze interfacial relationships. These values serve as a general reference, but values vary from male to female and between ethnic groups. Men tend to have sharper angles and more prominent features than women. These differences help us subconsciously determine gender, as well as the degree of masculinity and femininity.
relationships between various aesthetic masses, and to determine the proportions of each feature individually. The following tables define standard reference points used in facial analysis (Tables 170.1 and 170.2, Fig. 170.2). Using these standard points, reference angles are constructed to analyze interfacial relationships. These values serve as a general reference, but values vary from male to female and between ethnic groups. Men tend to have sharper angles and more prominent features than women. These differences help us subconsciously determine gender, as well as the degree of masculinity and femininity.
 Figure 170.1 When the ratio of the long segment to the short segment (AB/BC) is the same as the ratio of the whole line to the long segment (AC/AB), the ratio is equivalent to the divine ratio, phi (1.618). (Adapted from Ricketts RM. Divine proportions in facial esthetics. Clin Plast Surg 1982;9:401-422, with permission.) |
TABLE 170.2 BASIC ANATOMIC LANDMARKS AS SEEN ON FRONTAL VIEW | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
General Facial Assessment
Facial assessment begins with an evaluation of symmetry. A line drawn through the midsagittal plane on frontal view provides a side-by-side comparison of symmetry. The midline points of the forehead, nose, lips, and chin should lie on this axis. Subtle asymmetries are expected and it is helpful to point these out to the patient preoperatively.
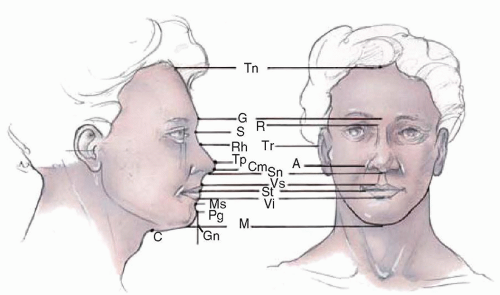 Figure 170.2 Basic anatomic landmarks for facial analysis. See Tables 170.2 and 170.3 for explanation. |
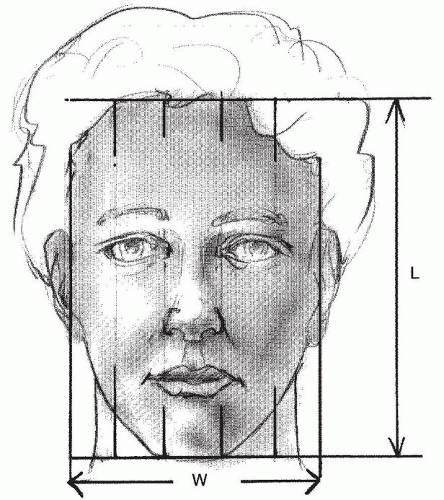 Figure 170.3 Ideal frontal symmetry and proportion is approximated by dividing the face into vertical fifths, with each fifth approximating the width of the eye. The overall width-to-length ratio should approximate 3:4. |
Assessment of symmetry and proportion is further accomplished by dividing the face into vertical fifths equal to the width of one eye, or the intercanthal distance. Vertical lines at the lateral canthus should approximate the width of the neck (32). The lateral-most fifth extends from the lateral canthus to the lateral most point of the helical rim (Fig. 170.3).
Facial height is examined by dividing the face into horizontal thirds on the frontal and lateral views (Fig. 170.4). The total facial height is the distance from the trichion to the menton. However, the trichion can be an inaccurate landmark due to receding hairlines in some individuals. In these cases the trichion is approximated by marking the uppermost extent of frontalis movement. The face is
then divided into horizontal thirds at the glabella and the subnasale. This creates an upper third from trichion to glabella, a middle third from the glabella to the subnasale and a lower third from subnasale to menton.
then divided into horizontal thirds at the glabella and the subnasale. This creates an upper third from trichion to glabella, a middle third from the glabella to the subnasale and a lower third from subnasale to menton.
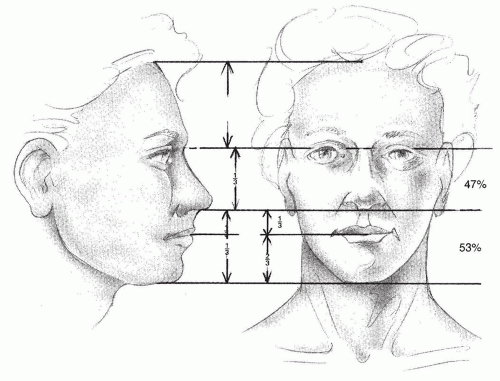 Figure 170.4 The facial thirds: trichion to glabella, glabella to subnasale, subnasale to menton. The lower face also is divided into thirds: The upper lip from subnasale to stomion is one-third, and the lower lip and chin is two-thirds. The face from nasion to subnasale is 47% and from subnasale to menton is 53% of the total height from nasion to menton. (From Powell N, Humphries B. Proportions of the aesthetic face. New York: Thieme-Stratton, 1984, with permission.) |
Lower facial symmetry can be further assessed by subdividing this region in thirds as well. The upper third is equal to the distance from the subnasale to the stomion, while the lower two-thirds are equal to the distance from the stomion to the menton (33).
The facial profile assessment examines the relationships of individual components to the face as a whole. Lateral view assessment begins with positioning of the patient in the Frankfort horizontal (Fig. 170.5) (Tables 170.3 and 170.4). When a line from the inferior orbital rim to the tragion is parallel to the horizon, the patient is said to be in the Frankfort horizontal. This provides a reproducible posture for comparison between patients and over time.



