4 Preoperative Endocrine Evaluation
The preoperative evaluation of a patient with a pituitary tumor or sellar mass should involve the combined efforts of a neurosurgeon and an endocrinologist.1 The first priority is to assess the stability of the patient from a neurologic perspective to gauge the urgency with which surgery should be undertaken. This task can be accomplished with a history and physical examination, coupled with a pituitary-cut magnetic resonance imaging (MRI) with gadolinium to evaluate the size and anatomical location of the tumor. In most patients with acute neurologic compromise or acute visual loss due to chiasmal involvement of the mass, emergent surgery should be pursued, irrespective of the tumor etiology. A possible exception to this rule is a patient with a macroprolactinoma, because such patients can have rapid improvement in visual field loss with dopamine agonist therapy. The majority of sellar masses, however, are diagnosed in neurologically stable patients, and it is the preoperative endocrine evaluation of these cases that is the focus of this chapter.
From an endocrine perspective, the preoperative evaluation of a patient with a known pituitary or sellar mass has two essential goals: to determine the functionality of the tumor and to assess the integrity of critical hormonal axes. Hormone-producing pituitary masses include prolactinomas, adrenocorticotropic hormone (ACTH)-secreting tumors (Cushing’s disease), growth hormone (GH)-secreting tumors (acromegaly), thyroid-stimulating hormone (TSH)-secreting tumors, and gonadotropin (luteinizing hormone [LH] or follicle-stimulating hormone [FSH])–secreting tumors (Table 4.1). Many patients with a hormonally active tumor, with the exception of those with a gonadotropin-secreting tumor, present with clear signs and symptoms of hormone hypersecretion, making the history and physical examination an important component of the initial preoperative evaluation. However, some patients may present with more subtle findings that are not immediately attributable to the hormone excess. Therefore, additional endocrine laboratory studies should be performed preoperatively to confirm the diagnosis of a suspected functional mass or to detect a clinically silent tumor. At our institution, our preoperative testing typically includes measurements of serum levels of prolactin and cortisol, plasma ACTH, and serum free thyroxine (T4), TSH, LH, FSH, GH, and insulin-like growth factor-1 (IGF-1) and in some cases α-subunit (Table 4.2).
Table 4.1 Clinical Characteristics and Initial Laboratory Evaluations for Secretory Pituitary Adenomas
| Tumor Type | Clinical Signs and Symptoms | Laboratory Testing |
|---|---|---|
| Prolactin-secreting (prolactinoma) | Oligo- or amenorrhea | Prolactin level (at dilutions)—persistently elevated |
| Impaired libido | Rule out medication-induced and other causes of | |
| Infertility | hyperprolac tinemia | |
| Galactorrhea | Consider stalk compression versus prolactinoma etiology (see text) | |
| ACTH-secreting (Cushing’s disease) | Central obesity | 24-hour UFC—elevated |
| Supraclavicular/dorsocervical fat pads | Overnight (1 mg) dexamethasone suppression test—cortisol ≤1.8 μg/dL excludes Cushing’s | |
| Thin skin, bruising, striae | Nighttime salivary cortisol—elevated | |
| Proximal muscle weakness | ACTH level—normal or elevated | |
| Hypertension, diabetes | ||
| GH-secreting (acromegaly) | Acral enlargement | IGF-1—elevated above age-adjusted normal range |
| Coarsening of facial features | GH suppression during an OGTT (criteria see text) | |
| Hyperhidrosis | ||
| Snoring, sleep apnea | ||
| New hypertension or DM | ||
| TSH-secreting | Hyperthyroidism symptoms | TSH—normal or high (not suppressed) |
| Weight loss, tremor, sweating | Free thyroxine (FT4)—elevated | |
| Goiter | ||
| Gonadotropin | Rare clinical features | LH and FSH—circulating level may be high α-Subunit—circulating level may be high |
Abbreviations: ACTH, adrenocorticotropic hormone; DM, diabetes mellitus; FSH, follicle-stimulating hormone; GH, growth hormone; IGF, insulin-like growth factor; LH, luteinizing hormone; OGTT, oral glucose tolerance test; TSH, thyroid-stimulating hormone; UFC, urine free cortisol.
Table 4.2 Routine Initial Laboratory Evaluation in a Patient with a Pituitary or Sellar Mass
| Prolactin (at dilutions) |
| Cortisol (a.m.) |
| ACTH |
| IGF-1, GH |
| TSH, FT4 |
| LH, FSH |
| α-subunit |
| Testosterone (males) |
| Serum sodium level |
Abbreviations: ACTH, adrenocorticotropic hormone; FSH, follicle-stimulating hormone; FT4, freethyroxine; GH, growth hormone; IGF-1, insulin-like growth factor-1; LH, luteinizing hormone; TSH, thyroid-stimulating hormone.
Among the hyperfunctional tumors, excluding or diagnosing a prolactinoma preoperatively is particularly important because most can be managed with dopamine agonists, thus obviating the need for surgery.2 The remaining hormonally active pituitary tumors are typically treated with surgery if specific clinical, visual, and neurologic features of the patient are present, although it is important to recognize that some hormone-secreting tumors are clinically silent (typically the gonadotropin-secreting tumors). If circulating levels of none of the aforementioned hormones are elevated, the tumor may be a nonsecreting pituitary adenoma, which is often managed with surgery as well. Thus, preoperative knowledge of the tumor type is beneficial, as it may impact the preoperative, perioperative, and postoperative management of the patient.3
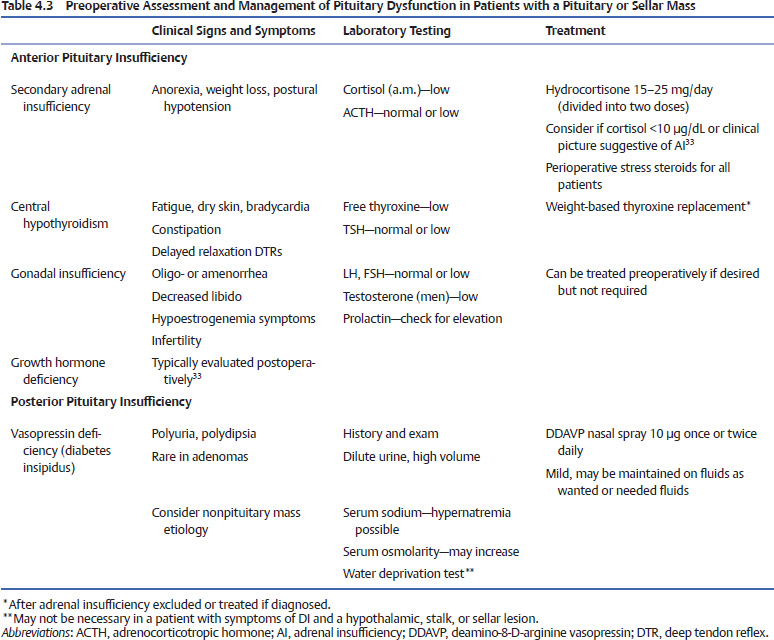
All patients, regardless of the tumor type, require preoperative assessment of the integrity of pituitary function to exclude partial or complete hypopituitarism (Table 4.3). With regard to anterior pituitary function, it is most important preoperatively to ensure the adequacy of the adrenal and thyroid axes, because untreated adrenal insufficiency or hypothyroidism can be clinically significant and potentially life threatening in the perioperative period. Evaluations for deficiencies in the remaining anterior pituitary hormone axes can be pursued after surgery.3 Posterior pituitary dysfunction most commonly manifests itself in the form of diabetes insipidus (DI), which is suggested by the history and physical examination. Preoperative DI is extremely uncommon in patients with pituitary tumors, and its presence should raise the suspicion for another etiology of the sellar mass, such as a craniopharyngioma or an infectious or inflammatory lesion.4
This chapter describes the endocrinologic characterization of the nature of the pituitary tumor and the evaluations that should be undertaken to screen for hypopituitarism and the need for perioperative hormone replacement therapy.
 Hormone-Secreting Pituitary Tumors Prolactinomas
Hormone-Secreting Pituitary Tumors Prolactinomas
The most common pituitary tumors are prolactinomas accounting for approximately 40% of all adenomas.5 Presenting symptoms of prolactinomas vary and often differ between men and premenopausal women. A man with a prolactinoma often presents with symptoms of gonadal dysfunction, such as decreased libido, impotence, or infertility, or with neurologic or visual symptoms because the tumors tend to be macroadenomas by the time medical care is sought.5 Among premeno-pausal women, symptoms of gonadal dysfunction typically bring them to medical attention earlier when their tumors are microadenomas. Up to 90% of premenopausal women present with oligo/amenorrhea and up to 80% with galactorrhea.5 In contrast, postmenopausal women may not come to medical attention until symptoms of a macroadenoma are present, such as a headache, visual disturbances, or other neurologic sequelae.5 Given this variability in clinical presentation, it is imperative to measure a prolactin level in all patients with pituitary masses prior to pursuing surgery, especially because the vast majority of prolactinomas can be managed medically.2
In interpreting the prolactin level, it is important to note that the differential diagnosis of hyperprolactinemia remains broad. Prolactin can be physiologically elevated in pregnancy or during the postpartum period if a woman is nursing.6 A pathologic elevation of prolactin can occur from the use of prescription medications, including neuroleptics, antidepressants, metoclopramide, methyldopa, reserpine, and verapamil, or from the use of illicit drugs such as cocaine or opiates.6 Finally, hyperprolactinemia can occur in the setting of cirrhosis, renal failure, or hypothyroidism, or it can occur idiopathically or in the setting of nonpituitary lesions or pituitary adenomas other than prolactinomas that involve the hypothalamus or hypothalamic-pituitary stalk.6
The presence of an adenoma on MRI in the setting of a sustained elevation of serum prolactin in a patient for whom secondary causes of hyperprolactinemia have been excluded is consistent with a prolactinoma. Typically, a single measurement of prolactin is sufficient for diagnosis, but ideally blood should be drawn at least 1 hour after the patient’s awakening or eating, and excessive venipuncture stress should be avoided.5 Recent guidelines for the diagnosis and management of prolactinomas suggest that prolactin levels greater than 150 μg/L are very suggestive of a prolactinoma and levels greater than 250 μg/L are suggestive of a prolactin-secreting macroadenoma.5 Prolactin levels less than 150 μg/L are seen in patients with microprolactinomas, as well as in those with stalk compression from any pituitary or sellar mass, making this distinction difficult. Definitive proof of a prolactinoma comes from the demonstration of a clinical response to a dopamine agonist because biopsy is not routinely pursued. A trial of a dopamine agonist in unclear cases may be informative because a prolactinoma should regress in size, whereas a nonsecreting mass would remain unchanged. Close follow-up of such patients with endocrinologic assessments and serial MRI should be undertaken.
In addition to the challenges discussed above, on occasion, prolactin levels can be reported incorrectly as low in the setting of a large prolactinoma. This phenomenon, the “hook effect,” is well documented and is secondary to antibody saturation by the high prolactin concentration in a immunoradiometric assay, which leads to artificially low prolactin values. To address this possibility, dilutions of the patient’s serum to 1:100 should be performed on all patients with large tumors but normal to mildly elevated prolactin levels.5 Finally, GH and IGF-1 levels should be assessed in all subjects in whom a prolactinoma is being considered. Approximately 20% of patients with acromegaly have elevations in prolactin,7 making it necessary to rule out this condition in patients with an elevated prolactin level. For patients with a co-secreting tumor, definitive therapy is generally focused on the GH-secreting component.
Once the diagnosis is confirmed, most prolactinomas can be medically managed with bromocriptine or cabergoline. Indications for surgery include failure of medical therapy to normalize prolactin levels when hyperprolactinemia is clinically significant, intolerance of medical therapy, visual field or other neurologic deficits that do not respond to medical therapy, or the presence of apoplexy with neurologic symptoms.5
Cushing’s Disease
The possibility of an ACTH-secreting pituitary tumor leading to Cushing’s disease should be considered in all patients presenting with a pituitary tumor. The evaluation for Cushing’s should begin with a complete history and physical examination. Patients with hypercortisolism in general (including Cushing’s disease) may present with a variety of signs and symptoms, including the nonspecific features of hypertension, fatigue, irritability, depression, weight gain, and new-onset or worsening of existing diabetes. More specific features of hypercortisolism include abnormal fat accumulation, particularly in the supraclavicular fossae, dorsocervical region, and centrally, as well as proximal muscle weakness, thin skin, bruising, and purple striae.8 A wide spectrum in the severity of these clinical manifestations at presentation makes screening often necessary.9
If a clinical suspicion of Cushing’s disease emerges, further laboratory evaluation should be pursued. A random elevated serum cortisol is not sufficient to confirm a diagnosis because the stress from venipuncture alone may increase cortisol levels.7 Instead, screening is typically performed with one of three tests: a 24-hour urine free cortisol (UFC) level, a dexamethasone suppression test (DST), or a nighttime salivary cortisol level.9 A 24-hour UFC level provides a reflection of the free cortisol circulating in the blood, and therefore its use is not hindered by conditions affecting cortisol-binding globulin (CBG) levels.9 A single assessment of 24-hour UFC levels, however, may not be sufficient, given the presence of mild Cushing’s disease in some patients10 and the intermittent nature of hypercortisolemia in other patients.11 Recent guidelines recommend checking up to three 24-hour UFCs in patients for whom clinical suspicion is high and in whom the first test is normal. If all three tests are normal, then Cushing’s is unlikely, assuming the glomerular filtration rate (GFR) is greater than 30 mL/min.9 Interpretation of the results of a 24-hour UFC should also consider the assay methodology used, as newer methods of high-performance liquid chromatography (HPLC) in tandem with mass spectroscopy appear to have the best specificity.11 Using the HPLC assay, a level greater than 50 μg/24 hours is typically considered elevated.12
Screening for Cushing’s disease with a DST is also commonly undertaken. One method is the overnight suppression test, which involves the administration of 1 mg of dexamethasone at 11 p.m. followed by a measurement of cortisol at 8 a.m. the next morning. The 48-hour test, still performed at some centers,9
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


