 Premalignant and Malignant Tumors of Eyelid Epidermis
Premalignant and Malignant Tumors of Eyelid EpidermisEyelid Actinic Keratosis
General Considerations
Many aging changes in the skin, including the eyelid, are secondary to gradual damage from lifelong exposure to ultraviolet light. Such damage is particularly prone to occur in light-skinned individuals (1,2,3,4,5,6,7,8,9,10,11,12). Actinic keratosis (solar keratosis) is a common precancerous cutaneous lesion that affects face, dorsa of the hands, bald areas on the head in men, and commonly the eyelids (1). Excessive exposure to sunlight is clearly a predisposing factor. A report from Japan found a mean patient age at diagnosis of 62 years and a slight predilection for females (3). If untreated, approximately 20% are believed to progress to squamous cell carcinoma (SCC) (2).
Clinical Features
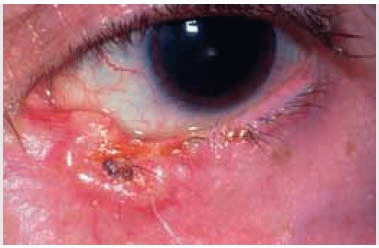
Actinic keratosis has several clinical variations, but is usually characterized by multiple, erythematous, excoriated, sessile plaques that may eventually assume a nodular, horny, or warty configuration (8). The lesions range from 1 to 10 mm in diameter and have a pink color. As mentioned, they generally occur on sun-exposed areas of older Caucasians who have had excessive sunlight exposure over a prolonged period of time (7).
Differential Diagnosis
The differential diagnosis includes most of the benign and malignant epidermal lesions mentioned in this atlas. It differs from seborrheic keratosis in that it has less distinct margins. Some actinic keratoses are pigmented, making the clinical differentiation from lentigo maligna and early melanoma difficult. The presence of multiple actinic lesions in the adjacent skin can facilitate the diagnosis.
Pathology and Pathogenesis
Histopathologically, actinic keratosis is composed of acanthosis, focal hyperkeratosis, dyskeratosis, and mildly atypical keratinocytes with epithelial buds that extend into the papillary dermis (1,2,3,4). Clefts often form as a result of dyskeratosis and disruption of intercellular bridges. A characteristic feature is orthokeratosis in the area of the ostea of the pilosebaceous structures. Such sparing of the ostea of these units is unlike true SCC. The dermis shows moderate to severe basophilic collagen degeneration and a moderate lymphoplasmacytic infiltration (1). Several histopathologic variants are described in the literature (2). Histopathologic study of eyelid SCC generally reveals evidence of actinic keratosis.
Management
There are several ways to manage actinic keratosis; treatment must be individualized. Small, asymptomatic lesions can be observed only. Larger lesions can be selectively resected with a shaving or elliptical approach, or curettage. Liquid nitrogen spray is often helpful for more indurated lesions (1). Multiple lesions or those that cannot be completely excised can be treated with topical chemotherapeutic agents or cryotherapy (1). Topical chemotherapy using 5-fluorouracil cream has been applied twice daily for 2 to 3 weeks (1).
There has been recent interest in treatment of actinic keratosis of the face and bald areas of the head with topical imiquimod (Aldara; Graceway Pharmaceuticals, Bristol, TN) cream administered 3 times weekly (11,12). In a randomized, double-blind, parallel-group, vehicle-controlled trial of 492 patients, complete and partial clearance rates for imiquimod-treated patients (48.3% and 64.0%, respectively) were clinically and statistically significantly higher than for vehicle-treated patients (7.2% and 13.6%, respectively). The median percentage reduction of baseline lesions was 86.6% for the imiquimod-treated group and 14.3% for the vehicle-treated group. It was concluded that 5% imiquimod cream applied 3 times weekly for 16 weeks is safe and effective for the treatment of actinic keratosis (11).
Prognosis
SCC that arises from actinic keratosis is low grade and offers an excellent prognosis because local invasiveness is minimal and metastasis occurs in only 1% to 3% of cases (10). In assessing SCC histopathologically, it is important to look for actinic keratosis near the margins. Such a finding imparts a better prognosis and compared with SCC that arises de novo, a condition that is somewhat more likely to metastasize.
Selected References
1. Griffith DG, Salasche SJ, Clemons DE. Cutaneous Abnormalities of the Eyelid and Face. New York: McGraw-Hill; 1987:204-207.
2. Kirkham N. Tumors and cysts of the epidermis. In: Elder D, Elenitsas R, Jaworsky C, et al., eds. Lever’s Histopathology of the Skin. 8th ed. Philadelphia: Lippincott-Raven; 1997:701-705.
3. Kiyokane K, Sakatani S, Kusakabe H, et al. A statistical study on clinical findings of solar keratosis. J Med 1992;23:389-398.
4. Font RL. Eyelids and lacrimal drainage system. In: Spencer WH, ed. Ophthalmic Pathology. An Atlas and Textbook. 4th ed. Philadelphia: WB Saunders; 1996:2237-2239.
5. Scott KR, Kronish JW. Premalignant lesions and squamous cell carcinoma. In: Albert DM, Jakobiec FA, eds. Principles and Practice of Ophthalmology. Philadelphia: WB Saunders; 1994:1734.
6. Doxanas MT, Iliff WJ, Iliff NT, et al. Squamous cell carcinoma of the eyelids. Ophthalmology 1987;94:538-541.
7. Hogan RN. The eye in aging. In: Albert DM, Jakobiec FA, eds. Principles and Practice of Ophthalmology. 2nd ed. Philadelphia: WB Saunders; 2000:4786.
8. Ostler HB, Maibach HI, Hoke AW, et al. Diseases of the Skin and the Eye. Philadelphia: Lippincott Williams & Wilkins; 2004:180.
9. Lund HZ. How often does squamous cell carcinoma of the skin metastasize. Arch Dermatol 1965;92:635-637.
10. Caya JG, Hidayat AA, Weiner JM. A clinicopathologic study of 21 cases of adenoid squamous cell carcinoma of the eyelid and periorbital region. Am J Ophthalmol 1985;15;99:291-297.
11. Korman N, Moy R, Ling M, et al. Dosing with 5% imiquimod cream 3 times per week for the treatment of actinic keratosis: results of two phase 3, randomized, double-blind, parallel-group, vehicle-controlled trials. Arch Dermatol 2005;141:467-473.
12. Urosevic M, Dummer R. Role of imiquimod in skin cancer treatment. Am J Clin Dermatol 2004;5:453-458.
Eyelid Actinic Keratosis
 Figure 2.1. Actinic keratosis showing multiple excoriated lesions in the periocular region of an elderly man. There is a characteristic lesion on the left upper eyelid. The lesions on the nose are unrelated retention cysts. (Courtesy of Armed Forces Institute of Pathology, Washington, D.C.) |
 Figure 2.2. Actinic keratoses in a patient being treated with 5-fluorouracil. |
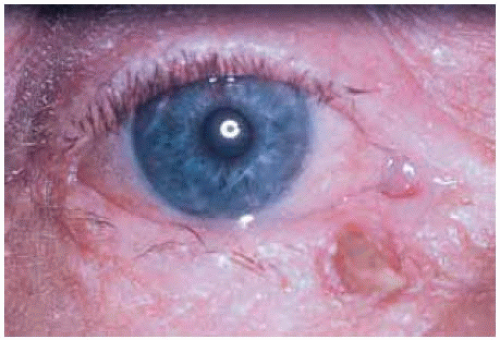 Figure 2.3. Close up view of slightly larger actinic keratosis near medial canthus. |
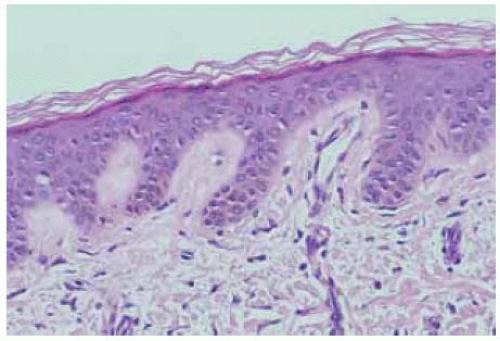 Figure 2.4. Histopathology of actinic keratosis. Note the epithelial buds that extend into the papillary dermis. (Hematoxylin-eosin 20.) |
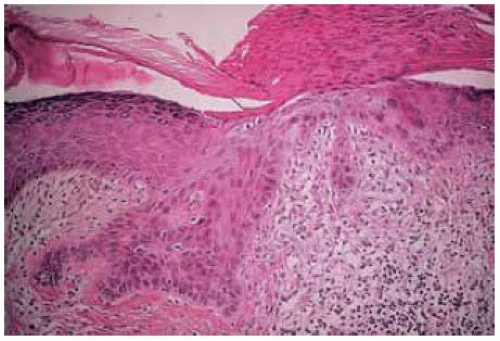 Figure 2.5. Histopathology of more severe actinic keratosis. (Hematoxylin-eosin 25.) |
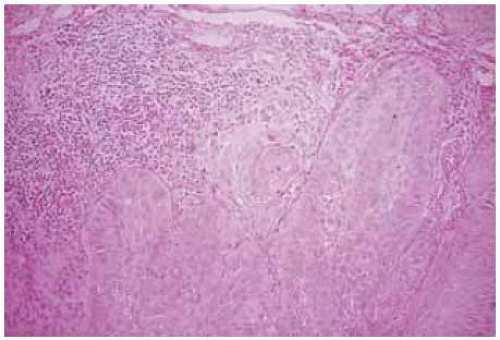 Figure 2.6. Histopathology of actinic keratosis with chronic inflammatory cells. (Hematoxylin-eosin 20.) |
Cutaneous Actinic Keratosis: Association With Conjunctival Squamous Cell Carcinoma
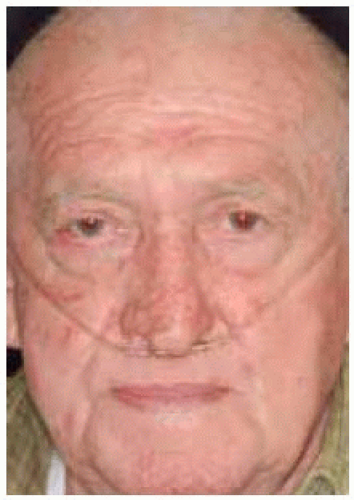 Figure 2.7. Elderly man with rosacea and chronic obstructive lung disease using oxygen. Note the numerous foci of actinic keratosis on face, especially the forehead. |
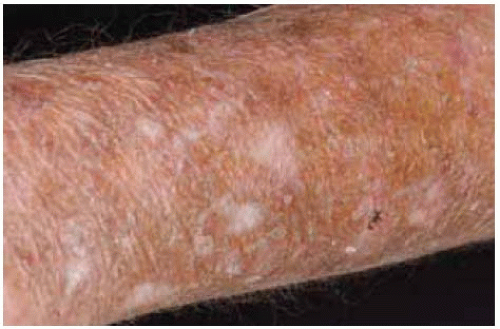 Figure 2.8. Skin involvement on forearm of patient shown in Figure 2.7, showing similar lesions. |
 Figure 2.9. Hand of same patient, showing white scales on dorsum of hand. |
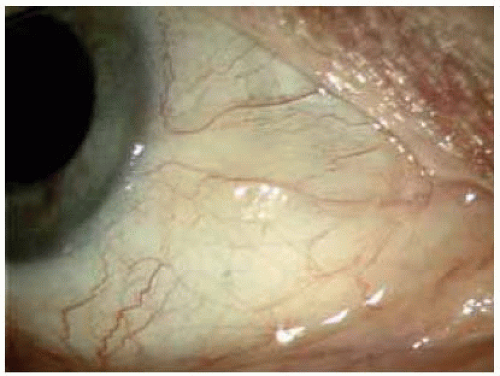 Figure 2.10. Same patient showing actinic keratosis of conjunctiva. |
 Figure 2.11. Face of another patient showing features of rosacea and actinic keratosis, most pronounced near lateral canthus of right eye. |
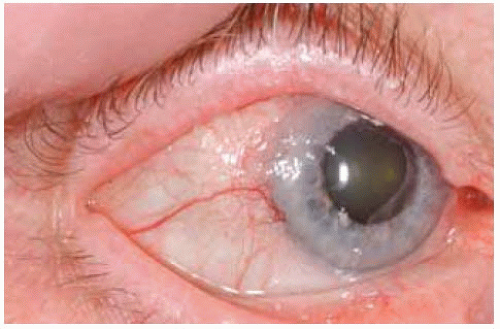 Figure 2.12. Conjunctiva of patient in Figure 2.11 showing SCC of conjunctiva (biopsy proven) on the right eye. Conjunctival SCC has a tendency to occur in patients with actinic keratosis of the skin. |
Radiation Blepharopathy
General Considerations
In addition to excessive sunlight exposure, there are miscellaneous other insults that can predispose the eyelid to malignant neoplasms. Selected examples include radiation blepharopathy, xeroderma pigmentosum, and the nevus sebaceous of Jadassohn, each of which are discussed. In addition, patients who are immunosuppressed for any reason have an increased risk of developing a number of benign and malignant eyelid lesions (1,2,3,4,5,6).
Radiation blepharopathy occurs secondary to therapeutic irradiation to the ocular region for a variety of conditions (1,2,3,4,5). A number of years ago, facial radiation was often used for acne and other benign conditions. This led to acute and chronic changes that predisposed the facial skin to the long-term development of several “radiation-induced” epithelial and glandular neoplasms, as well as soft tissue sarcomas. Ocular irradiation for retinoblastoma, particularly in patients with the germline mutation for that disease, can contribute to a variety of neoplasms, including eyelid tumors (1,2,3,4,5,6). In addition, irradiation for malignancies of the paranasal sinuses or nasopharynx can predispose to radiation blepharopathy and subsequent eyelid malignancies. Sebaceous carcinoma of the eyelid, normally a disease of older individuals, can occur at a young age in children who have undergone irradiation for retinoblastoma (5,6). Many of these neoplasms were more common many years ago when .80 Gy was used in some cases of retinoblastoma. Most radiation today employs a dose of 25 to 40 Gy, depending on the disease being treated.
Clinical Features
The acute stage of radiation blepharopathy develops about a week after initiation of irradiation. It is characterized by eyelid erythema, loss of cilia, and occasional excoriation or ulcer. Chronic radiation blepharopathy can show only minimal abnormalities, with skin atrophy and loss of cilia.
Diagnostic Approaches
The diagnosis of radiation blepharopathy lies mainly in taking a patient history for prior irradiation, combined with the clinical findings mentioned. We have found that some patients who develop eyelid malignancies in middle age may not immediately recall having had irradiation for acne or other reasons when they were young.
Pathology
Acute radiation blepharopathy shows edema and early degenerative changes in the epidermis, and epithelium of sebaceous glands and hair follicles. Late radiation blepharopathy is similar histopathologically to actinic keratosis, with nuclear atypia in the epidermal cells and individual cell keratinization. There may be scattered macrophages in the papillary dermis, fibrosis in the dermis, and atrophy of adnexal structures. The blood vessels become telangiectatic and may show individual cell swelling and thrombosis and recanalization. Squamous cell carcinoma that arises from these changes is generally of spindle cell type with a higher degree of malignancy and a greater tendency to metastasize than ordinary SCC. Atrophy of sebaceous gland is often profound (3).
Management
Management is directed toward prevention of cutaneous erosion, infection, and long-term cancers. Topical lubrication with antibiotics tends to soothe the site and prevent infection. Avoidance of steroid preparations is advised. The patient should avoid excess exposure to sunlight because actinic stimulation can further increase the chance of malignant transformation. Advanced cases with excoriation or ulceration may require more aggressive management with surgical intervention to restore vascular supply to the site. It is most important to check the patient yearly and to advise the patient to return earlier should there be any suspicious symptoms or signs.
Selected References
1. Font RT. Eyelids and lacrimal drainage system. In: Spencer WH, ed. Ophthalmic Pathology. An Atlas and Textbook. Philadelphia: 4th ed. WB Saunders; 1996:2242-2247.
2. Hawk JL, Smith NP, Black MM. The photosensitivity disorders. Radiation dermatitis. In: Elder D, Elenitsas R, Jaworsky C, et al., eds. Lever’s Histopathology of the Skin. 8th ed. Philadelphia: Lippincott-Raven; 1997: 313-315.
3. Karp LA, Streeten BW, Cogan DG. Radiation-induced atrophy of the meibomian glands. Arch Ophthalmol 1979;97:303-305.
4. Abramson DH, Ellsworth RM, Zimmerman LE. Nonocular cancer in retinoblastoma survivors. Trans Am Acad Ophthalmol 1976;81:454-456.
5. Rundle P, Shields JA, Shields CL, et al. Sebaceous gland carcinoma of the eyelid 16 years after irradiation for retinoblastoma. Eye 1999;13:109-110.
6. Kivela T, Asko-Seljavaara S, Pihkala U, et al. Sebaceous carcinoma of the eyelid associated with retinoblastoma. Ophthalmology 2001;108:1124-1128.
Eyelid Radiation Blepharopathy
Radiation blepharopathy can cause acute and chronic changes in the eyelids that can predispose to the development of squamous and sebaceous neoplasms later in life.
 Figure 2.13. Acute radiation blepharitis following external beam irradiation for retinoblastoma. |
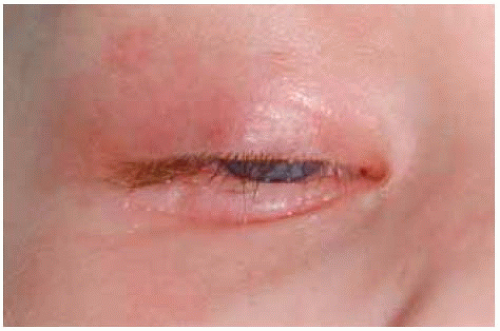 Figure 2.14. Close up view of patient in Figure 2.13, showing erythema, excoriation, and loss of cilia. |
 Figure 2.15. Early radiation blepharopathy after irradiation for retinoblastom a in a young child showing eyelid erythema. |
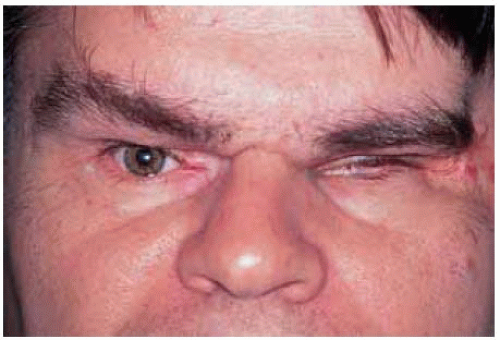 Figure 2.16. Radiation blepharopathy 43 years after treatm ent for retinoblastoma showing thickening and contraction of eyelid tissues. |
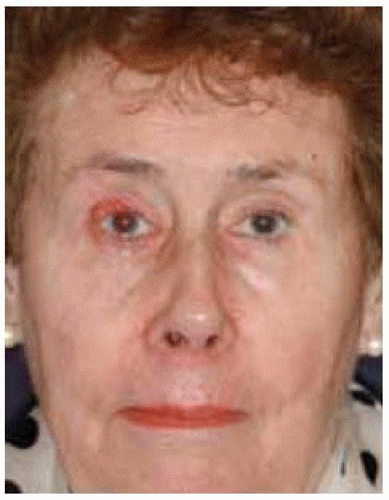 Figure 2.17. Chronic blepharopathy in right eye of a 72-year-old woman who had irradiation for facial acne as a child. Note the thin skin and telangiectasia on nasolabial fold and chin. |
 Figure 2.18. Closer view of right eye in patient shown in Figure 2.17. The blepharopathy was worse in the eyelids of right eye and eventual biopsy showed diffuse sebaceous carcinoma. |
Eyelid Xeroderma Pigmentosum
General Considerations
Xeroderma pigmentosum (XP) is an autosomal-recessive disorder that is not a specific eyelid lesion like other conditions discussed in this atlas. However, it is appropriate to discuss this disease because affected patients have a marked sensitivity to ultraviolet light that can predispose them to a variety of skin cancers, many of which involve the eyelid and conjunctiva (1,2,3,4,5,6,7). Cultures of skin fibroblasts and blood lymphocytes have demonstrated a deficiency in repair of damaged DNA. Death often occurs by the age of 20 years and, occasionally, by the age of 10 years, usually owing to metastasis from cutaneous squamous cell carcinoma or malignant melanoma.
Clinical Features
Six progressive stages of XP are identified, the details of which are beyond the scope of this atlas. In the earlier stages, the exposed skin shows numerous freckles, erythema, and scaling (4). Later, there is mottled pigmentation with telangiectasia that resembles radiation dermatopathy. The final stage is characterized by the development of a variety of malignant neoplasms often in the second or third decade of life, including squamous cell carcinoma, basal cell carcinoma, malignant melanoma, and some sarcomas (1). These multiple benign and malignant tumors can cause bothersome cosmetic problems.
Diagnosis
The diagnosis of XP can generally be made by the classic cutaneous features described, a positive family history, or both. Some patients have associated noncutaneous abnormalities, including mental deficiency, retarded growth, and delayed sexual development. The de Sanctis-Cacchione syndrome is characterized by XP, mental deficiency, microcephaly, dwarfism, hypogonadism, deafness, and ataxia (4).
Pathology
Histopathologically, the earlier stages are characterized by nonspecific changes, such as hyperkeratosis and hyperpigmentation of the basal layer of the epidermis. Later, there are irregular patches of hyperpigmentation with acanthosis and atypical downward proliferation of epidermis similar to actinic keratosis. The final stages are characterized by eruption of the various neoplasms mentioned (1).
Management
Management mainly includes avoidance of sunlight, topical sunscreens, protective clothing, ultraviolet blocking spectacles, and early removal of premalignant and malignant skin lesions. Some workers have published extensively on treatment of the lesions in the early stages, using a variety of oral and topical agents (6,7). The specific treatments are complex and beyond the scope of this atlas.
Selected References
1. Font RT. Eyelids and lacrimal drainage system. In: Spencer WH, ed. Ophthalmic Pathology. An Atlas and Textbook. 4th ed. Philadelphia: WB Saunders; 1996:2242-2247.
2. Gaasterland DE, Rodrigues MM, Moshell AN. Ocular involvement in xeroderma pigmentosum. Ophthalmology 1982;89:980-986.
3. Newsome DA, Kraemer KH, Robbins JH. Repair of DNA in xeroderma pigmentosum conjunctiva. Arch Ophthalmol 1975;93:660-662.
4. Ostler HB, Maibach HI, Hoke AW, et al. The genodermotoses. In: Diseases of the Skin and the Eye. Philadelphia: Lippincott Williams & Wilkins; 2004:87.
5. Iseroff RR, Galustian JC. Xeroderma pigmentosum. In: Mannis MJ, Masai MS, Huntley AC, eds. Eye and Skin Disease. Philadelphia: Lippincott-Raven; 1996:39-43.
6. Kraemer KH, DiGiovanna JJ, Moshell AN, et al. Prevention of skin cancer in xeroderma pigmentosum with the use of oral isotretinoin. N Engl J Med 1998;318:1633-1637.
7. Kraemer KH, DiGiovanna JJ. Topical enzyme therapy for skin diseases? J Am Acad Dermatol 2002;46:463-466.
Eyelid Xeroderma Pigmentosum
Like radiation blepharopathy, XP can also predispose the eyelids and conjunctiva to squamous cell carcinoma, basal cell carcinoma, malignant melanoma and other skin malignancies.
 Figure 2.19. Multiple facial lesions in a child with XP. |
 Figure 2.20. Face view of 15-year-old boy with XP showing scars from multiple skin grafts after surgical resections of melanoma and squamous cell carcinoma. |
 Figure 2.21. Multiple facial lesions in African-American patient with XP. |
 Figure 2.22. Multiple facial lesions in a child with XP. His head is turned downward and eyelids are closed because of photophobia. (Courtesy of Herman Grill, MD.) |
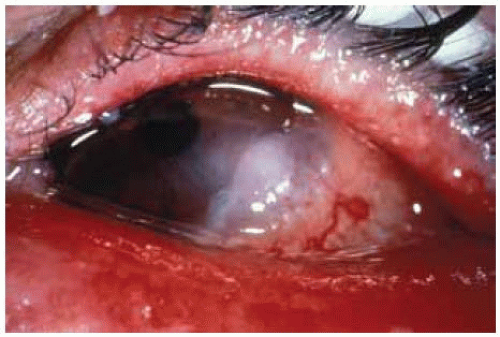 Figure 2.23. SCC of conjunctiva in patient with XP. Note the periocular skin changes. (Courtesy of Michael Zegans, MD.) |
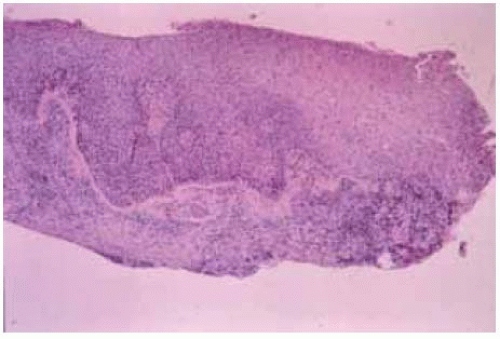 Figure 2.24. Histopathology of SCC in patient with XP shown in Figure 2.23, dem onstrating proliferation of m alignant squam ous cells. (Hematoxylin-eosin 200.) (Courtesy of M ichael Zegans, M D.) |
Sebaceous Nevus
General Considerations
Nevus sebaceous of Jadassohn (epidermal nevus syndrome) is an intriguing syndrome that has received attention in the recent literature (1,2,3,4,5,6,7,8,9,10,11,12,13). Sebaceous nevus can be an isolated lesion in the eyelid area, or a part of the organoid nevus syndrome. The neurologic aspects of the organoid nevus syndrome include seizures and mental retardation secondary to arachnoid cysts and cerebral atrophy. The best known ocular finding is the epibulbar complex choristoma (discussed in the section on conjunctival choristomas). The most frequent cutaneous feature of the organoid nevus syndrome is the sebaceous nevus of Jadassohn. This congenital cutaneous lesion can frequently give rise later in life to BCC and other benign and malignant cutaneous neoplasms.
Clinical Features
Sebaceous nevus can occur on the eyelid or eyebrow as a solitary lesion or as a component of a larger geographic lesion that affects the skin of the face, retroauricular area, and scalp, with contiguous involvement of the eyebrow and eyelid. It usually has a pink to brown color and well-defined irregular margins. The component that involves the scalp is usually associated with localized alopecia. The lesions are initially flat but become more elevated about the time of puberty, perhaps owing to sebaceous gland hyperplasia (1,2,3,4,5,6,7,8,9,10,11,12,13).
Diagnostic Approaches
The diagnosis can be easily made based on the typical clinical features mentioned. The patient should have a thorough ocular, dermatologic, and neurologic survey to exclude some of the mentioned systemic findings.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


