Preliminary Evaluation
Edward S. Bennett
Ronald K. Watanabe
Carolyn G. Begley
▪ PURPOSE
A comprehensive preliminary evaluation is the essential first step in the contact lens fitting process. It is extremely important for the practitioner to evaluate every potential contact lens wearer to determine whether the patient is suitable for contact lens wear. This will minimize the risk of future failures or problems because of poor patient selection. If the patient is deemed a good candidate, the information obtained during the prefitting examination will help determine the most appropriate lens material, lens design, wearing time, and care regimen. It also serves as baseline data with which changes caused by contact lens wear can be compared.
▪ HISTORY
A good history includes the patient’s reasons for wanting to wear contact lenses, ocular and medical histories, and any previous contact lens history. The history should guide the clinician in determining which tests to perform and the expected results for those tests. It should also contribute to the fitter’s recommendations on contact lens types, care regimens, and wearing schedules.
Reasons for Contact Lens Wear
Cosmesis. Many patients do not like their appearance in glasses.
Inconvenience of glasses. They may be uncomfortable, get misplaced or broken, and have to be cleaned.
Improved vision. Patients with high ametropias, high astigmatism, keratoconus, corneal trauma, corneal distortion, and poor refractive surgery outcomes benefit visually from contact lenses.
Sports and recreation. Most athletes, both professional and recreational, benefit from the wider field of vision provided by contact lenses.
Occupation. In addition to athletes, individuals in the performing arts benefit greatly from contact lens wear. Celebrities, politicians, and others in the public eye may prefer their cosmetic appearance in contact lenses. However, contact lenses are contraindicated for patients who work in dusty, dirty environments (e.g., coal miners, sanitation workers) where debris and particulate matter may become trapped under the lens. In addition, individuals such as laboratory workers and hairdressers who work around noxious fumes are borderline contact lens candidates because of the possibility of a chemical keratitis and lens surface contamination. Some workers such as plumbers and automobile mechanics may experience difficulty cleaning all of the dirt and oils off their hands and therefore may be poor candidates. Other individuals, such as pilots, flight attendants, and video display terminal operators, may work in low-humidity environments and perform tasks during which blinking is inhibited. These individuals are not contraindicated for contact lens wear but should be managed as potential dry-eye patients.
Ocular History
Previous correction. Glasses or contact lenses?
Strabismus and amblyopia. Significantly reduced acuity? Diplopia? Past treatment?
Vision therapy. Binocular vision problems or symptoms?
Eye trauma.
Eye surgery.
Medical History
The following symptoms and conditions may contraindicate or restrict contact lens wear:
Itching, burning, or tearing.
Seasonal or chronic allergies.
Recurrent ocular infection or inflammation.
Sinusitis.
Dryness of mouth, eyes, or mucous membranes.
Nocturnal lagophthalmos.
Convulsions, epilepsy, and/or fainting spells. Such an individual should be identified as a contact lens wearer.
Diabetes. Type 1 diabetics, in particular, may have varying degrees of corneal anesthesia, poor corneal epithelial healing, and the potential to develop neurotrophic keratitis.
Collagen vascular disorders. Patients with rheumatoid arthritis and related collagen vascular disorders may have Sjögren’s syndrome with keratoconjunctivitis sicca and associated tear film abnormalities. In addition, handling difficulties may be present.
Pregnancy. During pregnancy, particularly the third trimester, the tear film and corneal curvature may change significantly. This usually stabilizes shortly after childbirth.
Psychiatric treatment. Patients on medications to control anxiety, depression, or manicdepressive states should be screened but not necessarily discouraged from contact lens wear, especially if contact lenses would benefit them visually.
Thyroid imbalance. Hyperthyroidism, for example, may result in exophthalmos and lack of blinking, which can make contact lens wear difficult because of insufficient tear flow to the cornea.
Systemic medications. Certain medications can affect contact lens wear by reducing production of the aqueous phase of the tear film. Patients currently taking any of these medications should either be contraindicated as a contact lens wearer until the medication is discontinued or placed on a limited wearing schedule and carefully monitored. These medications include antihistamines, anticholinergics, some β-adrenergic blockers, tricyclic antidepressants, and oral contraceptives.1
Topical ocular medications. Patients using topical ocular medications may have restricted wearing times during contact lens wear. Soft lenses absorb the medication and alter drug delivery to the cornea, while gas-permeable (GP) lenses may block access to the cornea or increase contact time for any medication that collects under the lens.2 In general, topical medications should be instilled 15 to 20 minutes before application of contact lenses or after they are removed.
Contact Lens History
If the patient is currently wearing lenses or has worn them in the past, it is important to determine why the person desires a refit, since this will likely affect what lens material and design will be used. The following questions should be asked:
What type of contact lens does (or did) the patient wear? Satisfaction? Symptoms?
What is (are) the reason(s) for discontinuing wear or desiring a change?
What is the patient’s current wearing and lens replacement schedule?
What is the patient’s care regimen (if appropriate)? Satisfaction? Symptoms?
Is there a history of a contact lens-related problems or complications in the past?
Is there a frequent history of changing lens materials (i.e., “shopper”)?
▪ ANATOMIC MEASUREMENTS
Ocular and eyelid dimensions influence the selection of lens type, initial lens parameters, and fitting technique to be used (i.e., lid attachment vs. interpalpebral).
Horizontal Visible Iris Diameter
Horizontal visible iris diameter (HVID) provides an approximation of the corneal diameter and ranges from 10 to 13 mm.
HVID is measured with a pupil diameter (PD) ruler tilted inward and read using the horizontal scale (Fig. 1.1).
This measurement will help determine overall diameter of the contact lens.
Pupil Diameter
Measurement of pupil diameter is similar to that for HVID (Fig. 1.2).
Perform this measurement under both normal and dim illumination. The latter will help in determining the optical zone diameter of a GP lens, which should be 1 to 2 mm larger than the pupil to minimize flare with vertical blink movement and pupil dilation in dim lighting conditions (e.g., driving at night).
Pupil sizes (dim illumination) are categorized as follows:
Small pupil: <5 mm.
Medium pupil: 5 to 7 mm.
Large pupil: >7 mm.
For large pupil sizes, select a large optical zone (e.g., >8 mm) or a soft lens with a large optical zone. (Do not assume all soft lenses have large optical zones!)
Palpebral Aperture Height/Lid Position
Palpebral aperture height is equal to the vertical measurement of the opening between the upper and lower lids, with the patient gazing straight ahead.
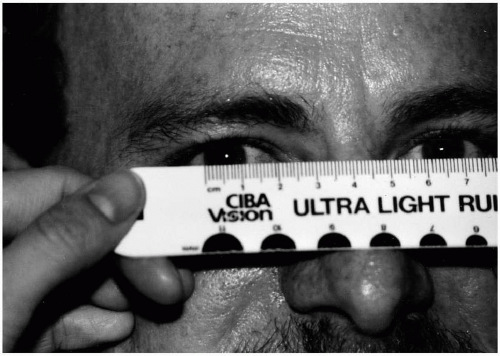
▪ FIGURE 1.1 Proper measurement of corneal diameter.
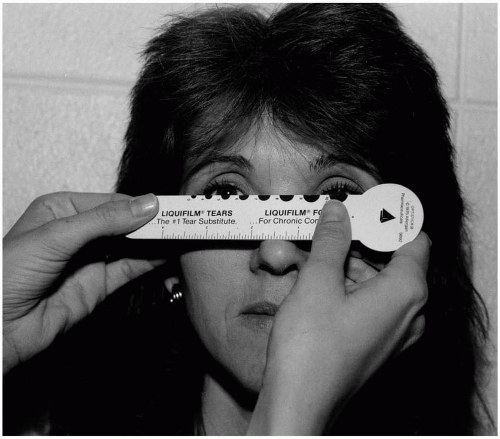
▪ FIGURE 1.2 Measurement of pupil diameter.
Perform this measurement with the patient relaxed and looking straight ahead (Fig. 1.3); also note and record the lid-to-cornea relationship.
This procedure will help determine type of lens and lens diameter for optimum patient comfort. A patient with an abnormally large palpebral fissure (e.g., ≥12 mm) will need a large-diameter lens for stability and comfort; likewise, a patient with an abnormally small palpebral fissure (e.g., ≤9 mm) will require a small-diameter lens.
Similarly, the position of the lower and upper lid to the limbus should be determined. A patient with a low upper lid that overlaps a large portion of the superior cornea is more likely to have a superior lid attachment. Likewise, a patient with a high upper lid that does not overlap much of the superior cornea is more likely to have an inferior lens position.3
Lid Tension
Lid tension is determined by lid eversion. Grasping the upper lid between the thumb and forefinger and gently pulling outward will give the practitioner an estimation of the lid tension over the globe.
Tight lids will pull a lens upward or may squeeze it downward (watermelon seed effect). Loose (heavy, fatty) lids will displace a lens downward.
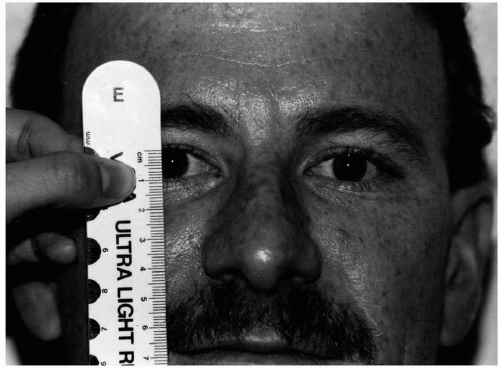 ▪ FIGURE 1.3 Measurement of palpebral aperture height. |
Blink Rate
A normal blink rate is 10 to 15 per minute.
Blink rate should be measured without the patient’s knowledge; note the amplitude, length, and completeness of a typical blink.
If the patient presents with only 10% to 50% completeness of the blink, GP lenses are contraindicated unless a lid attachment or superior fitting relationship exists after the blink.4 If the patient is a very infrequent blinker, soft lenses for social/occasional wear are recommended. On follow-up of patients with incomplete blinks, interpalpebral corneal and conjunctival desiccation should be monitored.
▪ REFRACTIVE INFORMATION
An evaluation of corneal topography and refractive status, with subsequent determination of predicted residual astigmatism, is imperative for proper contact lens design and parameter selection so that the likelihood of future success is maximized.
Corneal Topography
An evaluation of the patient’s corneal topography is important in determining the appropriate lens parameters to be diagnostically fit. The base curve radius (BCR) and diameter for both GP and soft lens materials are selected based on corneal curvature measurements.
Corneal Contour
The cornea is an aspheric surface with greatest curvature at the apex and progressively flatter curvature toward the periphery. It is classically visualized as consisting of an essentially spherical central corneal cap (apical zone/apical cap) and a surrounding peripheral zone that gradually flattens. The corneal cap is defined as the area within which the corneal power does not change more than 1 D and is approximately 4 mm in diameter. A more accurate description of the corneal contour is an ellipsoid centrally with progressively increasing radius of curvature and eccentricity toward the periphery.5 It is important to understand this corneal shape so that a contact lens can be optimally fit. For example, two patients having identical central corneal curvatures but different peripheral corneal curvatures and eccentricities are likely to be optimally fit with different contact lens parameters.
Evaluation
Methods for evaluating corneal topography include keratometry, autokeratometry, photokeratoscopy, and videokeratography (computer-assisted corneal topographic modeling).
Keratometer:
The most common instrument for measuring corneal topography, the keratometer averages the curvature values of a few points on the cornea separated by approximately 3 mm in both the vertical and horizontal meridians. This instrument has the advantages of both ease of use and low cost. However, there are disadvantages:
Only the central 3 mm of the cornea (approximately 8% of the corneal area) is evaluated.
The apex is not directly measured.
The central 3 mm of the cornea is assumed to be spherical, which may not be true. The magnitude of error is related to the rate of peripheral corneal flattening.
A decentered corneal apex may cause inaccuracy.
Examiner error is possible.
Keratometric change may not correspond with refractive change.
Despite its drawbacks, most practitioners still use keratometry for the initial selection of lens parameters because of its accessibility and ease of use. In fact, for initial base curve selection and prediction of residual cylinder, it has proven to be quite reliable. However, fluorescein pattern evaluation is still the most important assessment in GP contact lens fitting, while centration and lens lag are most important for soft lens fit assessments.
Autokeratometer:
Currently available automated keratometers provide accurate and consistent measurements of the central corneal curvature. The Humphrey Autokeratometer also assesses a larger area of the cornea (6.4 mm in the vertical meridian; 2.6 mm in the horizontal meridian), calculates the corneal curvature at the apex, provides the location of the apex, and calculates the shape factor. The disadvantages of automated keratometers include a much higher cost to the practitioner and a limited area of evaluation.
Photokeratoscope:
A photokeratoscope presents a hemispherical, lighted Placido disk image to the cornea. The observer focuses on a virtual image (plus sign) reflected from the corneal apex. A Polaroid photo is taken and analyzed to determine corneal curvature. Since the camera magnification is fixed and known, the amount of separation between rings can be used to determine curvature.6 The advantages of these instruments are their ability to provide a topographic analysis of at least 55% of the corneal surface, their ability to detect subtle topographic shifts, and the availability of data. The disadvantages include the more complicated data analysis and presentation, the limited availability of the instrument (it is no longer in production), and the expense.
Videokeratograph:
The videokeratograph (computer-assisted corneal topography system) is a state-of-the-art instrument that measures and analyzes thousands of points on the corneal surface to provide information on corneal curvature and contour. It produces a color-coded corneal topographic map that provides the examiner with an easy-to-read representation of the curvature of virtually the entire corneal surface. Most systems use a combination of computer technology and a photokeratoscopic (Placido disk) image (Fig. 1.4) to produce a comprehensive topographic map of the cornea. Alternative methods utilizing projected grids (raster photogrammetry),7 pachymetry,8 and Fourier analysis of sine waves9 have also been developed.
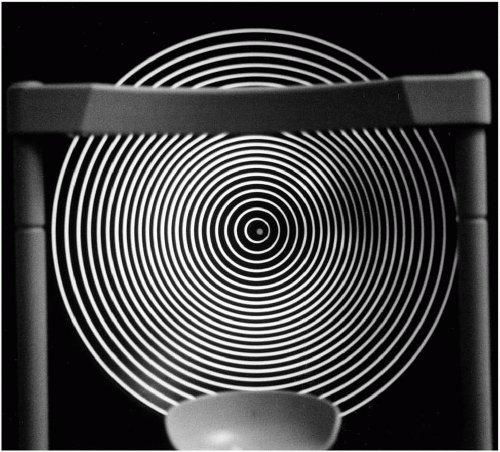 ▪ FIGURE 1.4 Photokeratoscopic cone used in Placido disk-based videokeratographers. |
In addition to calculating corneal curvature, videokeratography software is able to determine corneal eccentricity, surface regularity, and elevation. With this information, the practitioner can detect corneal irregularities that may be causing reduced visual acuity and more effectively manage corneal distortion induced by contact lens wear, trauma, or surgery. Also, all videokeratographers have software that can design GP contact lenses based on the topographic information it has obtained. These software programs can design GP contact lenses successfully, but for most normal corneas, it may still be more efficient and just as accurate for the practitioner to use keratometry values for initial lens selection.10,11 For irregular corneas, videokeratography more extensively describes the corneal contour, which may allow the practitioner to make contact lens-fitting decisions with greater confidence.12
The advantages of videokeratography include the availability of significantly more information, ease of use and analysis, and the most accurate method of monitoring topographic changes over time. The primary disadvantage is cost, although most systems are becoming very affordable for most practitioners.
Final Analysis
Despite the vast amount of information that videokeratography provides, most still consider keratometry the method of choice for diagnostic lens selection; however, it is important to remember that it represents only a starting point. As more accurate and accessible contact lensfitting software becomes available for videokeratography, it may replace keratometry. Currently, it is more valuable for qualitative evaluations of the overall shape of the cornea, particularly for distorted and highly astigmatic corneas, for which both initial fitting and long-term management are enhanced.
Refraction
It is important to perform a careful binocular refraction to help calculate the contact lens power and expected residual astigmatism. Residual astigmatism for spherical soft lenses is simply equal to the refractive astigmatism. For GP contact lenses, calculated residual astigmatism is determined by the following formula:
CRA (calculated residual astigmatism) | = | Refractive astigmatism | − | Keratometric astigmatism |
Example: Keratometry = 42.00 @ 180; 42.25 @ 090
Refraction = − 2.00 − 1.00 × 180
CRA = (− 1.00 × 180) − (−0.25 × 180) = − 0.75 × 180
Typically, if the actual residual astigmatism (ARA) measured by refracting over a GP contact lens is >0.75 D, a spherical GP lens is not recommended because of reduced vision. Depending on the amount of keratometric (corneal) astigmatism, either a soft or GP toric lens would be a better option. In the above case, if the ARA equals the CRA, the best option may be a soft toric lens since the ARA with a spherical soft lens will equal the refractive astigmatism, or −1.00 D.
▪ BINOCULAR VISION STATUS
Contact lenses may alter the binocular status of patients with high refractive errors or significant binocular anomalies. It is therefore important to test binocular function prior to lens fitting and make the necessary recommendations for lens wear.
Accommodation and Convergence
Pre-presbyopic moderate to high myopes may experience accommodative problems when switching from spectacles to contact lenses. In addition, they should be advised that a bifocal correction will probably be required at an earlier age. Convergence is similarly affected. A spectacle-corrected myope has a base-in prism effect when viewing at near, while a spectaclecorrected hyperope has a base-out prism effect. When contact lenses are worn, the myope loses the base-in prism effect at near and must converge more. Likewise, the contact lens-corrected hyperope loses the base-out prism effect at near and must converge less. Exophoric myopes and esophoric hyperopes may therefore experience more nearpoint symptoms with contact lenses than with spectacles.
Prismatic Correction
If base-in or base-out prism is necessary to provide binocularity and relieve asthenopic stress, it must be prescribed in spectacles. Although contact lenses can be worn together with spectacles, most patients would not appreciate the benefits of contact lens wear if glasses must be worn also. A small amount of base-down prism can be corrected in a contact lens, but base-up prism must be placed in spectacles.
▪ SLIT-LAMP EVALUATION
A comprehensive slit-lamp examination plays a vital role in determining whether the patient is a good contact lens candidate. The following should be evaluated on all prospective contact lens wearers:
External Observation
It is important to evaluate the eyelashes and external eyelids for the following conditions:
Blepharitis
Swollen inflamed lid margins reduce prognosis for successful contact lens wear. Debris from the lids may act as an irritant, and abnormal meibomian gland secretions will create an oily film on the lens surface. Staphylococcal blepharitis is also a potential cause of corneal infiltrates and may predispose the wearer to peripheral corneal ulcers. Acute and chronic forms of blepharitis should be treated before the patient is fit with contact lenses.
Entropion/Trichiasis
In-turned or disorganized lash patterns are not a contraindication for contact lens wear. In fact, a soft lens would protect the cornea from irritation caused by in-turned lashes.
Conjunctiva
The bulbar and tarsal conjunctiva should be evaluated biomicroscopically with white light. Rose bengal and lissamine green dye can be used to stain damaged or dead conjunctival cells, thus visualizing defects. Upper eyelid eversion is also required.
Bulbar Conjunctiva
Moderate injection of the bulbar conjunctiva, especially if persistent, may be caused by infection, dry eye, blepharitis, an allergic reaction, or other inflammatory process, and may contraindicate contact lens wear. Interpalpebral conjunctival staining is also suggestive of dry eye and should be investigated further with a tear film evaluation prior to contact lens fitting. Dense
or coalesced rose bengal or lissamine green staining of the interpalpebral conjunctiva is often associated with the symptoms of dry eye. The presence of a pinguecula could necessitate GP lens wear if the edge of a soft lens irritates this condition. The presence of a pterygium should contraindicate contact lens wear; however, if only a small region of the peripheral cornea is affected, contact lenses can be considered.
or coalesced rose bengal or lissamine green staining of the interpalpebral conjunctiva is often associated with the symptoms of dry eye. The presence of a pinguecula could necessitate GP lens wear if the edge of a soft lens irritates this condition. The presence of a pterygium should contraindicate contact lens wear; however, if only a small region of the peripheral cornea is affected, contact lenses can be considered.
Tarsal Conjunctiva
After upper eyelid eversion, the superior tarsal conjunctiva should be evaluated with and without fluorescein using the following scale13:
0 = satin. No papillae are observable.
1 = mildly elevated papillae, 0.1 to 0.2 mm in diameter, with uniform distribution (several papillae per millimeter of lid area).
2 = papillae are 0.5 to 1.0 mm in diameter, with nonuniform distribution.
3 = papillae 1 mm in diameter or greater are present on all regions of the upper lid.
Seasonal allergies result in mild papillary hypertrophy of the upper lid, usually of grade 1. A patient with giant papillary conjunctivitis (GPC, also known as contact lens papillary conjunctivitis [CLPC]) will exhibit large, irregularly sized papillae of grade 2 or 3 on the superior tarsal plate, which may be flattened and scarred if the condition is chronic (Fig. 1.5). GPC improves when a new contact lens is worn or with cessation of contact lenses. Thus, a new patient with GPC may be fitted in a daily disposable soft lens or a 2-week disposable lens, in combination with a decreased lens wearing time until the condition resolves. A mast cell inhibitor and/or corticosteroid may be used initially to decrease the inflammation.
Cornea
It is critical to carefully evaluate all aspects of the cornea prior to fitting. The presence of any significant corneal defect or disease process contraindicates contact lens wear until the condition has resolved. Many corneal defects are best visualized using the technique of indirect illumination. Chronic conditions, such as corneal dystrophies, may alter the type of contact lens, wearing schedule, and care regimen prescribed.
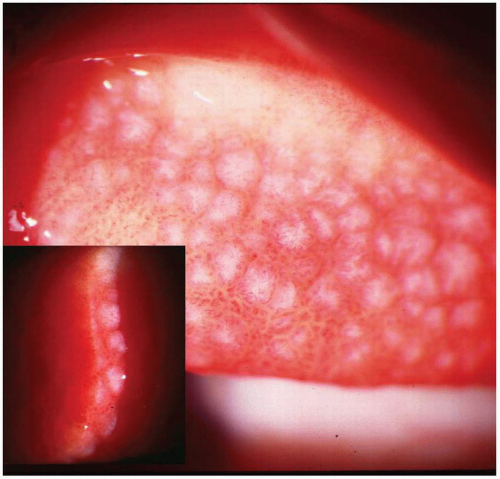 ▪ FIGURE 1.5 An everted upper lid from a patient with giant papillary conjunctivitis (GPC), showing grade 3 papillae on the upper tarsal plate |
Limbal Vasculature
A 360-degree evaluation of the limbal vessels should be performed. Documentation of limbal vessel encroachment onto the cornea should be made. It is important to differentiate normal limbal vasculature from contact lens-induced vascularization. Encroachment of 1 to 2 mm suggests chronic hypoxia and may indicate the need for refitting with a silicone hydrogel, even on a daily wear basis, or refitting with GP lenses. Encroachment of >2 mm requires refitting to increase oxygen to the cornea, a decreased wearing time, and careful monitoring to prevent further advance of the neovascularization.
Epithelial Staining
Fluorescein application using a fluorescein strip moistened with preservative-free saline is essential when evaluating a new patient. Any areas of punctate epithelial staining should be noted. Sequential staining with liquid fluorescein is also recommended.14 The presence of dense, coalesced staining may contraindicate fitting at that time and require treatment. It is important to always perform this procedure even if it is likely that the patient desires soft lenses. The eye can be thoroughly irrigated to rinse out the dye before lens application. Tear breakup time (TBUT) can be performed at this time as well.
Edema
The presence of deep stromal striae or folds, epithelial microcysts and vacuoles, or epithelial and stromal clouding indicate corneal edema and may contraindicate contact lens wear. The cause of the edema should be determined and treated, if possible. Occasionally, corneal dystrophies may cause edema; contact lenses are sometimes used in the management of these conditions. Epithelial microcysts are commonly found in extended-wear patients, and indicate that a period of oxygen deprivation has occurred.
Opacities: Scars versus Infiltrates
Carefully scan the cornea to differentiate an active from an inactive condition. Any active corneal infection or inflammation (e.g., corneal infiltrates, microbial keratitis) contraindicates contact lens wear at that time and requires the appropriate treatment.15 Corneal scars and other inactive opacities are not contraindications to contact lens wear.
Endothelium
Evaluate the endothelial layer for the presence of guttata and polymegethism. The presence of an endothelial dystrophy may contraindicate contact lens wear.
▪ TEAR FILM EVALUATION
The preocular tear film plays an important role in contact lens wear. It maintains hydration of soft contact lenses, determines lens surface wettability, acts as the primary anterior refracting surface, and deposits protein, lipids, and mucin onto the lens surface. Poor tear quality or quantity will reduce the patient’s prognosis for successful contact lens wear. There are several tear evaluations that should be performed to determine whether a patient is a good contact lens candidate.
Tear Meniscus Evaluation
The height and quality of the lower tear prism (lacrimal lake) are evaluated during the slit-lamp examination. This is a good test for detecting the borderline dry-eye patient. If the tear prism is not sufficient, an aqueous deficiency is present. The anterior border of the tear meniscus is
just behind the meibomian gland orifices. Where the meniscus meets the cornea, a black line exists that represents localized thinning. To evaluate the tear meniscus, fluorescein should be applied over the inferior bulbar conjunctiva about 1 to 2 minutes before evaluation4 and then observed with cobalt blue and Wratten no. 12 filters. When the meniscus is so thin that it appears as a fine line, it is a significantly insufficient tear meniscus (Fig. 1.6).
just behind the meibomian gland orifices. Where the meniscus meets the cornea, a black line exists that represents localized thinning. To evaluate the tear meniscus, fluorescein should be applied over the inferior bulbar conjunctiva about 1 to 2 minutes before evaluation4 and then observed with cobalt blue and Wratten no. 12 filters. When the meniscus is so thin that it appears as a fine line, it is a significantly insufficient tear meniscus (Fig. 1.6).
Tear Breakup Time
TBUT is the most widely used test of tear film quality and a good predictor of contact lens success. It is equal to the postblink time for dry spots to form in the tear film and it is theoretically caused by contamination of the mucin layer by lipids. Fluorescein is instilled, and the cornea is evaluated with a wide slit-lamp beam (i.e., 2 to 4 mm) under low magnification (i.e., 10× to 20×) with the cobalt blue filter. When wetting the fluorescein strip with saline, it is important to use unpreserved saline and shake excess moisture from the strip to avoid artificially destabilizing the tear film. The number of seconds until a dry spot forms is recorded. These dry spots appear as dark regions in the green-dyed tear film (Fig. 1.7). The patient is instructed to refrain from blinking during this period. An average normal value is 15 to 20 seconds. Less than 10 seconds indicates the patient may have dry eye, although many asymptomatic patients show tear breakup times in this range.16 However, a low tear breakup time indicates that the patient is best suited for daily wear, may suffer from end-of-the-day dryness,
and may not be able to obtain a comfortable all-day wearing schedule. Several important considerations could affect results:
and may not be able to obtain a comfortable all-day wearing schedule. Several important considerations could affect results:
Do not manipulate the lids immediately prior to testing.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


