Pregnancy and the Mother’s Eye
David J. Ramsey
Janet S. Sunness
1. Normal physiologic alterations seen in healthy eyes during pregnancy.
2. Ocular disease processes arising in pregnancy, such as preeclampsia.
3. Effects of pregnancy on preexisting eye disease, such as diabetic retinopathy.
4. Guidance on the use of ophthalmic medications and testing in pregnant patients.
Pregnancy is associated with maternal hormonal, metabolic, hematologic, cardiovascular, and immunologic alterations that can affect the ocular tissues. No significant ophthalmic changes occur in most normal pregnancies. However, pregnancy can be associated with the development of new ocular conditions such as serous retinal detachment related to preeclampsia, or with an exacerbation of preexisting disease processes such as diabetic retinopathy. These ocular changes are usually transient, but can cause permanent visual disability. This chapter presents the current state of knowledge about the relationship between pregnancy and maternal ophthalmic disorders. It also includes a brief summary of some considerations regarding diagnostic testing and therapeutic treatments during pregnancy.
EYELIDS
Skin changes are a frequent and polymorphous feature of pregnancy. Chloasma is a blotchy brown discoloration that may occur around the eyelids and usually fades postpartum. Hormonal factors may play a role, either elevated levels of melanocyte stimulating hormone or estrogen and progesterone.1 Spider angiomas are common during pregnancy and can occur on the eyelids, perhaps related to high estrogen levels.1 Ptosis has been reported during and following normal pregnancies, with one patient worsening after each of three pregnancies.2, 3 Most cases are unilateral. The authors suggest that the ptosis is caused by an aponeurosis defect, possibly related to increased fluid retention, hormonal effects, or the effects of labor and delivery. Another study of skin changes in pregnant women reported eyelid edema in 3 cases out of 60.4
CONJUNCTIVA
Changes in conjunctival blood vessels have been described toward the end of normal pregnancies. One study described granularity of the conjunctival venules, mild spasm of conjunctival arterioles, and decreased visualization of conjunctival capillaries.5 Another study reported increased vessel diameter in the second half of pregnancy.6 The conjunctival epithelium has been shown to undergo cytologic changes during pregnancy related to elevated estrogen levels.7 Vomiting during pregnancy can cause eyelid petechiae and subconjunctival hemorrhages. An increase in conjunctival pigmentation can be associated with normal pregnancy.
CORNEA
Corneal sensitivity has been found to be decreased in most pregnant women tested,8, 9 although one study found no change in corneal sensitivity.10 The sensitivity returns to normal by 2 months postpartum.8 The corneal sensitivity change does not appear to be related to the amount of increase of corneal thickness or weight gain.9
Corneal thickness has been reported to increase during pregnancy with resolution a short time after delivery in three studies.8, 11, 12 The amount of increase found varied from 1 µm11 to 16 µm.12 The change appears to be present throughout pregnancy.12 Two studies found no change in corneal thickness.10, 13 Possible causes of increased corneal thickness include fluid retention that is often associated with pregnancy.12
The corneal curvature has been found to increase (steepen) by 1 diopter (D) on average in the second half of pregnancy, with resolution postpartum or after cessation of breastfeeding.10 However, the manifest refraction did not change in this study. A second study showed no change in corneal curvature during pregnancy.13
The changes in corneal thickness and curvature may be factors in pregnant women developing difficulty with previously comfortable contact lenses.8, 10, 14, 15 and 16 Estimates in the literature are that 25% to 30% of contact lens wearers develop problems during pregnancy.10, 16 A woman may develop contact lens intolerance during one pregnancy, but not during another.10 It has not been reported whether the symptoms correlate with the degree of corneal curvature and corneal thickness change. A decrease in tear production was found during the third trimester of pregnancy in about 80% of pregnant women studied.16 Other changes such as conjunctival modification and lid edema also may be factors leading to discomfort with contact lens wear.16 It is preferable to avoid prescribing a new correction for patients until several weeks postpartum if this is possible.
There is some weak evidence suggesting that pregnancy may alter corneal immune function. One case report describes bilateral herpes simplex virus (HSV) keratitis in a pregnant contact lens wearer. The authors suggest that pregnancy-associated immunosuppression and contact lens wear may have an additive effect and increase the possibility of HSV recurrence.17 Corneal perforation has been reported in the setting of rosacea fulminans in pregnancy.18 Retrospective study of 3,608 corneal grafts found that pregnancy was a statistically significant univariate risk factor for graft failure.19 This suggests that pregnancy might be a risk factor for graft rejection in some patients.
Pregnancy may prompt hormonal changes, which in turn could affect the biomechanical stability of the cornea. There has been a case report of spontaneous corneal melting in pregnancy.20 Keratoconus has also been reported to progress in pregnancy, prompting its diagnosis21 or progression.21, 22 There is also a case report of a woman with bilateral keratoconus who developed corneal perforation late in pregnancy.23
Krukenberg spindles are found more commonly in pregnant women, unassociated with other evidence of pigmentary dispersion. The spindles become smaller late in pregnancy and postpartum. It has been hypothesized that the development of Krukenberg spindles may be related to hormonal changes and that resolution late in pregnancy relates to increased facility of outflow.24
REFRACTIVE CHANGES IN PREGNANCY
One cross-sectional study compared 38 nonpregnant to 93 pregnant women and found no differences in refractive error, corneal curvature, corneal thickness, accommodative amplitude, AC/A ratio, and fusion break ranges between the two groups.13 Another smaller casecontrol study of 83 pregnant patients matched with sequentially presenting nonpregnant controls found a small subset of 12 patients that reported subjectively decreased vision and had a myopic shift of <1 D; post partum, all patients returned to their prepregnancy refraction.25 Another study found no refractive error, cornea curvature, or visual acuity changes among 72 patients.26
A population-based study in South India that evaluated female reproductive factors, including age at menarche, age at natural menopause, and median number of pregnancies, found no influence on the prevalence of myopia, as well as several age-related ophthalmic disorders.27
Pregnancy may also impact refractive surgery outcomes in the perioperative and postoperative period, in several cases years after the procedure. One report suggested that photorefractive keratectomy (PRK) near or during the time of pregnancy may lead to suboptimal outcomes.28 Another study showed myopic regression in 12/18 (66%) and corneal haze in 10/12 (83%) with a history of PRK eyes during pregnancy. The corneal haze and myopic regression improved in 50% of eyes after delivery29 and in one case report, after a spontaneous abortion.30 A third study failed to demonstrate impaired PRK outcomes after pregnancy.31 Two cases of pregnancy-associated cornea ectasia following laser insitu keratomileusis (LASIK) for nearsightedness have been reported. The first case consisted of a woman who developed bilateral iatrogenic keratectasia during her first pregnancy 26 months after LASIK. Corneal collagen crosslinking (CCL) with riboflavin and ultraviolet-A was performed and arrested the progression; however, keratectasia worsened again during the patient’s second pregnancy.32 Another case was reported to occur 18 months following a myopic LASIK procedure, steadily worsening over the course of pregnancy.33 Unrecognized forme fruste keratoconus is an important risk factor for post-LASIK ectasia and should be routinely screened for in all refractive surgery patients, especially those who are pregnant or likely to become pregnant.
INTRAOCULAR PRESSURE
Studies have found about a 20% decrease in intraocular pressure (IOP) during pregnancy.34, 35, 36, 37, 38, 39 and 40 This ocular hypotensive effect seems to increase until delivery26, 36, 37, 38, 39 and 40 and may persist for several months postpartum.41 A greater reduction of intraocular pressure was noted among pregnant women with baseline ocular hypertension in one study.37 Another investigation showed that the reduction in IOP was greater among multigravida than among primigravida women.35 However, two studies have demonstrated that IOP is higher in the peripartum period for women with third trimester hypertension or preeclampsia than in normotensive pregnant women.39, 42 A third study failed to corroborate this association.34
Several etiologies for pregnancy-related reduction in IOP have been proposed. There is an increased facility of outflow43, 44, 45 and 46 and increased uveoscleral outflow,34 possibly related to hormonal effects. Changes in progesterone levels during pregnancy may correlate with changes in IOP.45 There may be decreased episcleral venous pressure,41, 47 consistent with a general decrease of venous pressure in the upper extremities during pregnancy. Finally, there is also a small change in ocular rigidity during pregnancy.48 Aqueous production appears to remain constant during pregnancy.45, 46
One case of acute angle closure glaucoma during labor has been reported. However, the patient was later believed to have had unrecognized subacute attacks prior to pregnancy.49 There is also a case report of acute angle closure glaucoma in the setting of preterm labor precipitated by ritodrine, a beta-2 adrenergic receptor agonist used as a tocolytic drug by virtue of its ability to cause uterine smooth muscle relaxation.50
One study has examined the impact of labor on IOP.51 Sixty-four pregnant patients without a history of baseline ocular hypertension or glaucoma were evaluated both before and immediately after delivery. The study reported a mean IOP increase of 1.4 mm Hg during active labor followed by a decrease of 3.0 mm Hg immediately after delivery. The IOP returned to baseline in all patients by 72 hours after delivery. Valsalva maneuvers have also been shown to increase IOP and could lead to intermittent increases in IOP during active labor, but are of such a short duration that they are unlikely to cause any glaucomatous progression.52
Transient hypotensive shock associated with large amounts of blood loss during labor may be mistaken for glaucoma-like optic nerve and visual field changes.53, 54 and 55
The Blue Mountains Eye Study (1992 to 1994) examined 2,072 women aged 49 to 97 years and included questions about female reproductive factors such as age at menarche and menopause, parity, and use of hormone replacement therapy.56 A modest increase in OAG risk was found to be associated with later (>13 years) compared with earlier (≤12 years) age of menarche. Although increasing parity was associated with an increased risk of primary open angle glaucoma (POAG) (P = .03), there was a decreased risk of ocular hypertension (P = .03).
Recently, the Nurses’ Health Study, which followed 79,440 women, reported that in multivariable analysis, there were no significant linear trends between age at menarche, reproductive duration defined as time between age at menarche and menopause, or parity and POAG. In contrast, >5 years of oral contraceptive use was associated with a 25% increased risk of POAG; however, ever using oral contraceptives was not associated with POAG risk. These modest associations add further support for a role of circulating estrogen in the pathogenesis of POAG.57
A population-based study in South India that evaluated female reproductive factors, including age at menarche, age at natural menopause, and median number of pregnancies, found no influence on the POAG, age-related cataract, macular degeneration, or myopia.27
The course of glaucoma during pregnancy may be variable, requires close monitoring by an ophthalmologist, and may require medications or even surgery to control IOP and to prevent vision loss during pregnancy.58 Glaucoma laser procedures, such as laser peripheral iridotomy and laser trabeculoplasty, pose no known teratogenic risk or increased side effects in pregnant women.59
LENS
The curvature of the crystalline lens has been reported to increase during pregnancy.16 A transient loss of accommodation has been reported during and after pregnancy.60 However, a more recent study failed to demonstrate any change in accommodative amplitude during pregnancy.13
An increase in lens autofluorescence has been reported in pregnant patients with diabetes compared with nonpregnant diabetic patients.61 This observation suggests the possibility of lenticular metabolic alterations during pregnancy. Another small study, which included 15 healthy pregnant women in their third trimester, showed a significant decrease in lens autofluorescence in pregnant women compared to a normal population.62 Although the nature of this change is not well understood, it has been suggested that there is an increase in the aqueous component of the lens, thereby diluting the fluorescent substances.
A case-control study from central India63 showed that having more than three babies doubled the risk of developing bilateral cataracts in the 35- to 45-year age range. The extent to which this is related to nutritional status is not clear. A larger population-based study in south India found no increased prevalence of age-related cataract.27
EXTRAOCULAR MUSCLES
Patients can present with strabismus during pregnancy. A search for preexisting underlying conditions may help to clarify the diagnosis. For example, three otherwise healthy pregnant women developed a superior oblique palsy during pregnancy. On evaluation, they had amblyopia and decreased stereopsis, suggesting that there may have been decompensation of a latent vertical deviation.64 One healthy patient developed a transient sixth nerve palsy during pregnancy, unassociated with other changes (C. Rommel, personal communication, 1991), or patients with hyperemesis gravidarum, pernicious vomiting in pregnancy, can develop thiamine deficiency, leading to Wernicke’s encephalopathy with nystagmus and extraocular muscle palsies.65, 66, 67, 68, 69, 70, 71 and 72
NEURO-OPHTHALMOLOGIC CHANGES
Bell’s Palsy
The most common cranial neuropathy encountered in pregnancy is Bell’s palsy or facial neuropathy. The incidence of Bell’s palsy is more than three times as frequent in pregnant woman than age-matched nonpregnant women, approaching 50 per 100,000 live births, and more than two-thirds of cases are encountered in the third trimester.73, 74 The etiology of cranial neuropathies may be related to an increase in interstitial fluid around the nerve, creating focal compression. A case of simultaneous idiopathic bilateral Bell’s palsy during the third trimester of pregnancy has been reported.75
Visual Field
A number of different studies of visual fields during pregnancy were performed in the first half of this century, motivated by findings of pituitary enlargement during pregnancy.76 Some studies found no change in most pregnant women,77 some found concentric constriction,78 and some found bitemporal constriction.79, 80 and 81 One study among 41 pregnant women in Canada found no field loss and actually reported a small increase in the mean sensitivity of the visual field in the third trimester.26 These early studies found changes most prominently late in the pregnancy that generally resolved by 2 weeks postpartum. Patient fatigue and nonuniform equipment in the era before automated perimetry may have been factors in these findings.77 It is important to note that none of these healthy pregnant women were symptomatic in terms of visual field changes.
No recent studies of visual fields in normal pregnant women have been performed. It is felt that the increase in size of the pituitary gland during pregnancy is not sufficient to cause visual field change except when there is an unusual position of the pituitary relative to the optic chiasm.76
A complaint of visual field change in a pregnant woman should not be dismissed. Rather, it should be considered an indication for evaluation for a possible disease process such as an enlarging pituitary adenoma, meningioma, or lymphocytic hypophysitis (discussed in the following section).
Normal Pituitary
It was reported as early as 1909 that the normal pituitary gland undergoes enlargement during pregnancy. This was confirmed by later work82 and by recent studies using magnetic resonance imaging (MRI).83, 84 Beyond the first week postpartum, the pituitary rapidly returns to normal size regardless of the status of breastfeeding.84 Pregnancy-related pituitary enlargement is associated with an increased number of prolactin-secreting cells present during pregnancy.85 MRI also demonstrates increased intensity of the anterior lobe of the pituitary that is thought to be related to this increase in prolactin-secreting cells and to possible increases in endoplasmic reticulum.86 This enlargement generally does not lead to visual field defects. Therefore, a visual field defect in a pregnant woman should be evaluated for a possible pathologic cause.
CONDITIONS ARISING DURING PREGNANCY
Intracranial Disorders
Acute presentations of pituitary-based pathology during gestation may include previously unrecognized but enlarging tumors, apoplectic hemorrhage and necrosis, and the rare autoimmune condition, lymphocytic hypophysitis, that occurs most frequently in women in the last trimester of pregnancy or the early postpartum period. Pituitary adenomas and meningiomas do appear to become more symptomatic and grow more rapidly during pregnancy, although intracranial tumors overall do not appear to be more frequent than in nonpregnant women.87, 88 Because some of the symptoms of intracranial processes, such as nausea and vomiting, may be related to pregnancy alone, there may be a delay in diagnosing intracranial disorders. Intracranial disorders should be included in the differential diagnosis of pregnant women with visual acuity or visual field loss, persistent headaches, or oculomotor palsies,89, 90 while realizing that other processes may be responsible as well.
Pituitary Adenoma
Asymptomatic pituitary adenomas are common. A metaanalysis estimated the prevalence of pituitary adenomas at 16.7% (14.4% in autopsy studies and 22.5% in radiologic studies).91 Historically, these tumors have been characterized based on size with microadenomas measuring <1 cm and macroadenomas measuring ≥1 cm.
Although pituitary adenomas are now further classified according to immunohistochemistry and functional status, the risk of visual changes in pregnant women with pituitary adenomas is related primarily to tumor size.
The availability of drugs such as bromocriptine and cabergoline to induce ovulation in women with amenorrhea allow many women with pituitary adenomas to conceive.92 Pituitary adenomas can enlarge during pregnancy, probably as a result of a combination of the physiologic enlargement seen in normal pregnant women and growth of tumor. The size of the normal pituitary gland increases an average of 65% to 76% during pregnancy and in certain cases has increased as much as 120% to 136% when measured in the immediate postpartum period.83, 93 An MRI study of 17 pregnancies in women with prolactinomas reported no change in size in 45%, increased size in 27%, and decreased size in 27%.94 Another investigation estimated the risk of adenoma growth during pregnancy at 1% for microadenomas and 23% for macroadenomas.95
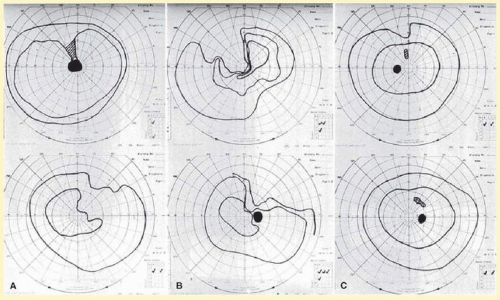 FIG. 32.1 Pituitary adenoma first presenting during pregnancy as a left anterior chiasmal syndrome. A: Goldmann visual fields in the sixth month of pregnancy showing bitemporal superior defects, the left (top) worse than the right (bottom). Visual acuity at this time was 20/30 OD and hand motions OS. B: Goldmann visual fields around the time of delivery show progression of the bitemporal superior defects. For each visit, the upper field is the left eye, and the lower field is the right eye. C: Goldmann visual fields performed 4 months after delivery show resolution of much of the visual field change. Visual acuity at this time was 20/15 in each eye. The patient remained stable thereafter and had a subsequent uncomplicated pregnancy 6 years later. (Courtesy of Neil Miller, MD.) |
The critical clinical issue for the ophthalmologist is whether this enlargement is associated with visual symptoms and signs, which then warrant treatment during pregnancy.
The most common visual findings are bitemporal visual field defects and visual acuity decrease (Fig. 32.1),96 but other visual disturbance, headaches,97 and rarely diplopia also may be seen.98, 99 The risk of a woman developing visual loss during pregnancy is primarily related to tumor size. However, a majority of patients with acromegaly do not experience an increase in tumor size during pregnancy, rarely have metabolic complications, and neonatal outcome is largely unaffected.100
A cohort study of 111 pregnancies in 65 women found that 6 of 8 (75%) with macroadenomas, whereas none of 57 (0%) with microadenomas developed vision loss during pregnancy.101 A smaller study of four women with macroprolactinomas similarly showed irreversible visual field loss in three of four (75%).102 A third study found a rate of visual involvement in 1 of 85 (1.2%) with microadenomas and 14 of 46 (30%) with macroadenomas.103 In contrast, one study reported that only 1 of 14 pregnant women with large prolactinomas developed visual field defects during pregnancy.104 Another study reported that 4 of 18 (22%) with adenomas developed visual loss but tumors were not differentiated according to size.96 A recent retrospective multicenter study of 59 pregnancies in 46 women reported visual field defects diagnosed during pregnancy in only 4 women, 3 of whom were diagnosed with acromegaly during pregnancy.105
Finally, there is often spontaneous regression of the adenoma postpartum (see Fig. 32.1), so that the decision to treat depends on the severity of visual findings during pregnancy, and how early in pregnancy the findings develop.98 Fortunately, the dopamine agonists bromocriptine and cabergoline can cause tumor regression both within and outside of the context of pregnancy. Many studies have demonstrated the efficacy of bromocriptine for pregnancy-associated adenoma progression,106, 107, 108, 109, 110, 111 and 112 and there have not been any reports of adverse pregnancy outcomes related to the drug.100, 101 and 102 Cabergoline also appears to be effective113, 114 and safe114 during pregnancy. One case report describes the successful treatment of a thyrotropin secreting macroadenoma during pregnancy with octreotide resulting in improved visual fields, reduced tumor size, and good pregnancy outcome.92
Surgical therapy of symptomatic adenomas also has been successfully employed during pregnancy,107 but in most cases this can be safely postponed until after delivery.100
Because the risk of symptomatic progression of a microadenoma during pregnancy is small, discontinuation of dopamine agonist therapy should be considered once pregnancy is confirmed. Treatment options for patients with macroadenomas include discontinuation of dopamine agonist therapy when pregnancy is confirmed and reinstituting therapy if the patient develops evidence of vision loss, continuous dopamine agonist therapy throughout pregnancy, and surgical debulking of the tumor prior to pregnancy.115 Decisions regarding management should be guided by an ophthalmologist, endocrinologist, obstetrician, radiologist, and possibly a neurosurgeon.
Lymphocytic Hypophysitis
Lymphocytic hypophysitis (LH) or adenohypophysitis is a rare autoimmune condition that occurs most frequently in women in the last trimester of pregnancy or the early postpartum period. The most common presenting symptoms are visual field defects and headache. Most patients show signs of isolated or multiple pituitary hormone deficiencies manifesting polyuria, polydipsia, hypernatremia, and diabetes insipidus. Adrenocorticotropin hormone (ACTH) secretion is most frequently impaired, followed by thyroid stimulating hormone (TSH), gonadotropins, growth hormone (GH), and prolactin (PRL).116 One-third of the cases involve hyperprolactinemia.117
One study of 16 patients found that 63% had anterior pituitary hypofunction, 56% had symptoms consistent with an expanding pituitary mass, 38% had hyperprolactinemia, 25% had associated autoimmune thyroiditis, and 19% had diabetes insipidus. Computed tomography (CT) and MRI scanning demonstrated a pituitary mass mimicking an adenoma in 83% of cases.118
Because LH can present with headache, visual field defects, hyperprolactinemia, and a pituitary mass by imaging, this disorder can be difficult to distinguish clinically from a prolactinoma. However, this differentiation is critical because a failure to recognize LH can lead to untreated pituitary insufficiency and death,119 and an incorrect diagnosis of pituitary adenoma may lead to unnecessary transsphenoidal surgery. A study of 45 patients with lymphocytic hypophysitis and 806 with pituitary adenoma during pregnancy found that history and endocrinologic evaluation will usually differentiate these disorders. The spontaneous pregnancy rate was 100% in LH, whereas only 2.4% in patients with pituitary adenoma. Prolactin levels averaged 34.6 µg/L in LH compared with 393 µg/L for pituitary adenomas. Hypothyroidism and hypocortisolism were present in 57.5% of LH cases, but only 2.5% of patients with pituitary adenomas. There were no distinguishing features on radiographic studies,120 and LH may be confused with apoplexy.121
The authors recommend that patients presenting to an ophthalmologist during pregnancy with signs and symptoms consistent with a pituitary disorder be co-managed with an endocrinologist, obstetrician, radiologist, and possibly a neurosurgeon.
There is strong anecdotal evidence in the form of case reports that treatment with steroids can lead to marked improvement in vision loss from LH and possibly avoid permanent pituitary insufficiency in some cases.122, 123, 124, 125 and 126 Most cases lead to varying degrees of irreversible visual field loss or pituitary insufficiency. However, there are six reported cases of complete recovery,121, 126, 127, 128, 129 and 130 and only two of those cases were treated with steroids.121, 126
Little was known about the etiology of LH until recently. Serum autoantibodies directed against a 49-kDa cytosolic protein have been detected by immunoblotting in 70% of patients with biopsy proven LH.130a In 2002, the target pituitary autoantigen was identified as alpha-enolase,131 and similar autoantigen targeting of the gamma-enolase isoform found in placental tissue was soon found.132 This established a direct link between pituitary and placental autoantigens and provides a theoretical basis for the strong predilection for LH to occur during or shortly after pregnancy. Two documented cases of a ruptured Rathke’s cleft cyst have been reported, suggesting that disruption of cyst integrity may be a trigger for LH.133, 134 The authors are not aware of any evidence suggesting increased perinatal morbidity or mortality associated with LH.
Intracranial Meningioma
Sixty-five percent of all intracranial meningiomas occur in women.135 The age-adjusted incidence of meningioma is 4.52 per 100,000.136 The incidence in pregnant women is comparable to nonpregnant women of the same age.137 Growth of these tumors is typically slow, producing insidious visual disturbances. In contrast, during pregnancy some meningiomas rapidly enlarge, producing dramatic and relatively acute vision loss.90, 138 The diagnosis can be delayed because nausea, vomiting, and other symptoms caused by the tumor may be attributed to pregnancy.90, 139 The tumors present more commonly during the second half of pregnancy.88 The predominance of meningiomas in women, their accelerated growth during pregnancy and the luteal phase of menstruation, and an association with breast cancer led to studies examining the potential role of hormones on meningioma growth.140 Subsequent studies have supported this association by demonstrating that about 70% of meningiomas express progesterone receptors and approximately 30% express estrogen receptors.141
Ocular findings can include decreased visual acuity, visual field defects that depend on the location of the tumor, oculomotor palsies, papilledema, and late optic atrophy.142, 143, 144, 145, 146, 147 and 148 Rarely, extension may cause proptosis or other orbital signs.149 Symptoms may abate spontaneously after delivery and can recur during subsequent pregnancies.90,150 Hormone-responsive intracranial meningiomas should be considered in the differential diagnosis of visual disturbances during pregnancy.90 Close cooperation among ophthalmologist, neurosurgeon, obstetrician, and neonatologist are essential for an optimal outcome.
If there are no neurological impairments, pregnancy may be carried to full-term delivery. Management with steroids and anticonvulsants may delay surgical excision, which is usually the treatment of choice during pregnancy.90, 137 In the early post-operative setting, adjuvant external beam radiation therapy or brachytherapy may be considered, but should be withheld until after delivery.151 Antiprogesterone therapy may be effective in receptor positive cases, but is unlikely to have a role during pregnancy.
Idiopathic Intracranial Hypertension (Benign Intracranial Hypertension or Pseudotumor Cerebri)
Idiopathic intracranial hypertension (IIH) is a syndrome of increased intracranial pressure characterized by normal brain imaging, normal cerebrospinal fluid (CSF) composition, and elevated CSF pressure. IIH occurs at the same rate in pregnant and nonpregnant women,152, 153, 154 and 155 but one study showed worsening of symptoms among nine of 11 patients with preexisting IIH who became pregnant.156
The most common symptoms of IIH in pregnancy are headaches and visual changes. One study found that among 240 normal pregnant women, 12 developed IIH during one or more pregnancies. Ten had headaches, five had transient visual obscuration, four had reduced visual acuity, four had visual field loss, and three developed diplopia. All 12 women developed bilateral papilledema of varying severity.157
Visual outcome does not appear to differ between pregnant and nonpregnant women with IIH.152, 153, 157 A study of 13 pregnant IIH patients found that vision loss occurred at the same rate as age- and parity-matched controls.153 In addition, pregnancy outcomes are not adversely affected by IIH.152, 158, 159
The management of IIH during pregnancy includes weight control, nonketotic diet, steroids, and certain analgesics. Diuretics have been used in some cases. When medical management fails, serial lumbar punctures, optic nerve sheath fenestration, or lumboperitoneal shunt can be considered.152, 160 Treatment decisions should be made in coordination with an obstetrician and possibly a neurosurgeon. Therapeutic abortion to limit progression of the disease generally is not indicated.152, 160 The risk of recurrent IIH in subsequent pregnancies does not appear to be increased.158 Women who have developed IIH during pregnancy should not be advised against future pregnancies.161
Intracranial Aneurysms and Arteriovenous Malformations
Hemorrhagic cerebrovascular accidents (CVAs) are the most common neurosurgical diagnosis made in pregnancy.162 Intracranial hemorrhages are responsible for 4% to 12% of all maternal deaths163, 164 and can be caused by arterial aneurysms, arteriovenous malformations (AVMs), metastatic choriocarcinoma, and disseminated intravascular coagulation (DIC).165, 166 One retrospective study of 50,700 pregnancy-related admissions identified 13 hemorrhagic CVAs. Seven hemorrhages were subarachnoid and six were intracerebral. Five were caused by AVMs, three by arterial aneurysms, two by DIC, and three were idiopathic.166 Another retrospective meta-analysis study found that among 152 intracranial hemorrhages, 77% were caused by aneurysms and 23% by AVMs.164
Fifty percent of ruptured arterial aneurysms in women under the age of 40 are pregnancy-related.167 The hemodynamic and endocrinologic changes of pregnancy appear to be the cause of arterial alterations that can lead to new aneurysm formation or enlargement or rupture of a preexisting aneurysm.162, 167, 168 and 169 Aneurysm rupture occurs more often in primiparous women162 and in the third trimester of pregnancy.162, 166, 170 In one study, 92% of intracranial hemorrhages occurred antepartum and 8% postpartum.164 In contrast, women with AVMs do not appear to be at a significantly increased risk of hemorrhage during pregnancy. Seven studies have reported no elevated risk of hemorrhage from AVMs during pregnancy.170, 171, 172, 173, 174, 175 and 176
The most common presentation of a ruptured aneurysm or AVM is severe headache, seizure, or other neurologic signs from subarachnoid hemorrhage (SAH). However, enlarging aneurysms or AVMs can cause mass effects leading to cranial nerve palsies,177 optic nerve compression,178 or papilledema. One study reported that the possibility of focal neurologic deficit was higher among patients with intracranial AVMs than aneurysms.174 Patients with SAH can also develop subhyaloid or vitreous hemorrhage (Terson’s syndrome).179 Secondary intraocular hemorrhage usually is managed conservatively,179 but vitrectomy may be indicated in bilateral or nonclearing cases.
The early diagnosis and management of a ruptured arterial aneurysm or AVM are critical in order to optimize the chances of maternal and fetal survival.167 The clinical challenge is that differentiating eclampsia from SAH can be difficult and may lead to a delay in diagnosis.164, 165, 166 and 167, 169, 180, 181 and 182 The diagnosis is further complicated by the fact that preeclampsia and eclampsia are independent risk factors for aneurysm rupture183 so that these entities may coexist. Clinicians should maintain a high level of suspicion for intracranial aneurysm when pregnant women present with headache, seizure, altered consciousness, focal neurologic signs, visual changes, or diplopia. Urgent MRI and magnetic resonance angiography (MRA) scanning is the current diagnostic modality of choice because there is no radiation risk or side effects of contrast media.184
The management of intracranial aneurysms generally is the same for pregnant as for nonpregnant patients,168, 169 and neurosurgical considerations take precedence over obstetric considerations.168, 171, 185, 186 When SAH occurs, endovascular obliteration,187, 188 and 189 neurosurgical clipping,190 or stereotactic radiosurgery189 of the aneurysm or AVM may be carried out in order to avoid recurrent hemorrhage and secondary ischemia.162 One study of AVMs recommended that patients at high operative risk be managed conservatively until after delivery.189 Another study reported that surgical management of aneurysms was associated with improved maternal and fetal survival. Taken together, these studies suggest that the threshold for neurosurgical intervention might be lower for aneurysms than AVMs, although this decision should be made by the neurosurgeon. The risk of rebleeding in the same pregnancy was 27% among AVMs in one study.191 Visual field and optic nerve changes can resolve over time following surgery.178, 192
Once an aneurysm or AVM has been treated successfully, pregnancy can be allowed to progress to term. Most obstetricians prefer vaginal delivery in these cases,169, 187 although one study reported a bias toward caesarian section among patients with AVM.189 Fetal mortality is not increased among mothers with intracranial aneurysms provided that the mother survives.193 Women with arterial aneurysms or AVMs are not advised against future pregnancy in most cases.170
Cerebral Venous and Sinus Thrombosis
Cerebral venous and sinus thrombosis (CVST) in the pregnant and puerperal state occurs with an incidence of 10 to 20 per 100,000 deliveries and accounts for 5% to 20% of all cerebral venous thrombosis.194 The signs and symptoms are nonspecific, which can lead to a potentially fatal delay in diagnosis.195, 196 A retrospective study of 138 cases found that 74 (54%) presented in the first 7 days of the postpartum period.197 The most common signs and symptoms were fever (62%), headache (48%), seizure (46%), hemiplegia (43%), altered consciousness (41%), and papilledema (35%).197 Another retrospective study of 25 cases reported similar presenting clinical signs, which included headache (96%), focal neurologic deficits (60%), papilledema (43%), and seizure (40%).195 Magnetic resonance venography (MRV) is the preferred diagnostic modality, and treatment is with heparin anticoagulation.
The increased incidence of intracranial venous thrombosis is attributed to the hypercoagulable state of pregnancy,198, 199 and 200 inherited protein C198, 201, 202 and S deficiencies,198, 203, 204 and eclampsia.205 A prospective study found that 78% of patients with venous thrombosis during pregnancy and the puerperium demonstrated activated protein C resistance (factor 5 Leiden).201 Three case reports have found associated protein S deficiency.198, 203, 204 There is one case report of transverse sinus thrombosis associated with eclampsia.205 The authors suggest a causative mechanism but this association may be incidental. It is recommended that causes of inherited hypercoagulability be investigated in all women who develop CVST during pregnancy or puerperium.
Mortality from CVST is <20%.196, 206 The visual prognosis generally is good with blindness occurring because of late optic atrophy in 2 of 77 (3%) patients in one retrospective study.207 Women with pregnancyrelated CVST should not be discouraged from future pregnancies.196, 208 In one retrospective study, among 39 women with a history of CVST during pregnancy, 14 had 22 subsequent pregnancies resulting in 19 births and 1 elective and 2 spontaneous abortions; five patients were prophylactically treated with low-dose heparin.208 In another study, among 77 women with pregnancy-related CVST there was no recurrence of CVST during subsequent pregnancies, and only one postpartum deep venous thrombosis occurred.207
Metastatic Choriocarcinoma
Gestational choriocarcinoma is a malignant tumor that frequently undergoes hematogenous metastasis to highly vascularized organs such as the lung, brain, and liver. The incidence of choriocarcinoma is 1 in 50,000 live births and 1 in 30 molar pregnancies.209 Intracranial choriocarcinoma metastases can present as intracerebral,210, 211, 212, 213, 214 and 215 subarachnoid,215, 216 and 217 or subdural hemorrhages.218, 219 These tumors can bleed primarily or cause arterial aneurysms210, 216, 218, 220 or arteriovenous fistulae217 with secondary bleeding. In a retrospective analysis of 10 cases, the most common presenting symptoms were features consistent with elevated intracranial pressure and hemiparesis.221 Ophthalmic signs and symptoms may be present and can include visual acuity or visual field loss, transient visual obscuration, papilledema, and retinal hemorrhages.216, 221 It is important to consider this rare tumor in cases of young women presenting with stroke symptoms because it is potentially curable.211
Amniotic Fluid or Air Embolism
Amniotic fluid embolism is a rare but serious complication of pregnancy resulting in death in the majority of patients.222, 223 Particulate matter of amniotic origin has been identified at autopsy in the brain, lungs, and kidneys.222 Focal neurologic deficits are rare,194, 224 but can affect the optic nerve, visual pathways, or occipital cortex. One case report describes a branch retinal artery occlusion attributed to an amniotic fluid embolism.223 There is also one isolated case of cortical blindness from air embolism that occurred following induced abortion and improved following treatment with hyperbaric oxygen.225
Carotid-Cavernous Fistulae
There are reports of five carotid-cavernous fistulas developing or worsening during pregnancy.220, 226, 227 and 228 One spontaneous fistula improved without intervention after the mother aborted the pregnancy in the 12th week.226 A second spontaneous fistula worsened 3 weeks after a normal delivery before improving without intervention.226 Two carotid-cavernous fistulas were caused by metastatic choriocarcinoma.220, 229 A traumatic fistula that had resolved 4 years prior to pregnancy recurred, causing two antepartum and one postpartum hemorrhages. The authors propose that pregnancy-related hormonal and hemodynamic changes caused the recurrence and hemorrhage.228 However, the paucity of reports about carotidcavernous fistulae during pregnancy suggests that this association may be incidental. In familial cerebral cavernous malformations, visual deterioration during pregnancy or breastfeeding may occur in genetically predisposed tissue, including the optic nerve, which may present with signs confused for optic neuritis.230
Optic Nerve
Multiple Sclerosis and Optic Neuritis
Multiple sclerosis (MS) is a common cause of optic neuritis and is the most common chronic disabling neurologic disease affecting women of childbearing age.231 Pregnancy has a protective effect on MS with fewer and less severe relapses, especially during the third trimester.231, 232, 233, 234 and 235 However, the relapse rate increases in the first 3 months following delivery before returning to prepregnancy rates.231, 232, 233, 234, 235 and 236 Breastfeeding and epidural analgesia have no deleterious effect on relapse rates.231, 233, 234 The Pregnancy and Multiple Sclerosis study prospectively followed 254 women with MS through 269 pregnancies. Compared to the year prior to pregnancy, there was a reduction in the relapse rate during pregnancy, which was most marked in the third trimester. There was a striking increase in the relapse rate in the first 3 months after delivery, although 72% of the women did not experience a relapse during these 3 months. After this, the rates returned to prepregnancy levels.233, 234 Relapse rates remained at prepregnancy rates at the 2-year follow-up.234 A recent retrospective review of 351 women with MS confirmed the finding that the MS relapse rate decreases throughout pregnancy and increases during the puerperium.235
Overall, pregnancy has no long-term effect on MS-related disability or disease course.231, 232, 233 and 234, 237 Apart from methotrexate and cyclophosphamide, most drugs used routinely in the treatment of MS, including steroids, can be used safely by pregnant women.237 A study of 14 pregnant women with relapsing-remitting MS, who were treated with postpartum intravenous immunoglobulin (IVIG) in an attempt to avoid postdelivery recurrences, found that none of the patients who received postpartum IVIG relapsed238 compared with the expected relapse rate of about 28%.234 Further study is needed to confirm this apparent protective effect.
Women with MS who desire children can be reassured that their infants are not at increased risk of malformations, preterm delivery, low birth weight, or infant death.231, 233, 234, 237 Because a woman’s past history of relapses may be the best indicator of future clinical course and long-term disability,232, 233 and 234 women with more severe disease may wish to complete their families as soon as possible.237
A condition called “lactation optic neuritis” has been described in the first 12 months following delivery unassociated with known MS.239, 240 The clinical course is similar to classic optic neuritis that occurs without lactation. It is possible that decreased immunosuppressive activity during the postpartum period induces the initial clinical manifestation of a previously unrecognized demyelinating disorder such as MS.239 The paucity of cases reported in the literature also suggests that this also could be an incidental association.
Additional Pregnancy-Related Optic Neuropathies
Devic’s syndrome (neuromyelitis optica) is characterized by optic neuritis with transverse myelitis and may present during pregnancy.241, 242 and 243 Severe vomiting in pregnancy (hyperemesis gravidarum) can lead to optic neuritis.244 One case of ischemic optic neuropathy has been reported in association with severe preeclampsia.245 A case of bilateral idiopathic optic neuritis with permanent visual loss recently was reported in association with pregnancy.246 One case of pregnancy-related papillophlebitis in a woman with no identifiable coagulation defect has been reported.247 A case of optic disc drusen related visual loss has also been reported.248
Other Neuro-Ophthalmologic Disorders
Cortical Vision Loss in Preeclampsia and Eclampsia
Preeclampsia typically develops after midgestation and is characterized by hypertension and proteinuria. Eclampsia is preeclampsia with convulsions that usually occurs late in pregnancy, complicating 1% to 2% of severe preeclampsia.249 The HELLP syndrome consists of hemolysis, elevated liver enzymes, and low platelets, and it is generally associated with severe preeclampsia or eclampsia; it significantly increases the risk of preterm labor, maternal and fetal complications, and perinatal mortality. In healthy women, preeclampsia is generally seen in first pregnancies with an incidence estimated at 5%. Risk factors for preeclampsia include very young or advanced maternal age, multifetal pregnancy, hemolytic disease of the newborn, diabetes mellitus, chronic systemic hypertension, and renal disease. Preeclampsia and eclampsia place the fetus at risk because of placental vascular insufficiency. Delivery remains the only cure for preeclampsia/HELLP syndrome combined with blood pressure control and seizure prophylaxis, as well as monitoring of fetal well-being.249
Preeclampsia and eclampsia are the most common causes of pregnancy-related focal neurologic deficits250 and pregnancy-related ischemic strokes.251 These deficits are characteristically of sudden onset and usually resolve over time. The precise pathogenesis of these stroke-like focal deficits remains poorly understood.194, 224
Transient visual changes occur in up to 25% of patients with preeclampsia252 and up to 45% of eclampsia.253 Most patients recover normal vision within hours to several weeks. Cortical blindness is a rare but dramatic finding usually related to the occurrence of the posterior reversible encephalopathy syndrome (PRES)254, 255 and more rarely Balint’s syndrome, a rare condition usually associated with cerebral infarction (or neurodegenerative diseases).256
A prospective study of 15 women who developed preeclampsia/eclampsia-related cortical blindness reported complete resolution over 4 hours to 8 days.257 Another retrospective analysis of 19 cases of eclampsia reported transient cortical blindness in 2 patients that completely recovered in both.258 Preeclampsia usually resolves with delivery; however, in rare cases it may worsen within 48 hours after delivery,259 and transient cortical vision loss may also occur in the postpartum period.260
PRES is a clinical-neuroradiological syndrome characterized by headache, seizures, altered mental status, and vision loss in the setting of neuro-imaging findings consistent with vasogenic edema. The syndrome is thought to be due to loss of cerebral autoregulation in the context of endothelial dysfunction. In the setting of hypertension, this can lead to subsequent hyperperfusion resulting in vasogenic edema.261, 262
It has been proposed that the occipital lobes are more susceptible because the vertebrobasilar arterial system is less well supplied by sympathetic nerves than the anterior cerebral circulation that is provided by the internal carotid arteries.263 The etiology of cortical vision loss remains controversial, however. Various mechanisms have been proposed, including cerebral vasospasm with ischemic injury257, 264, 265 and 266 and increased capillary permeability leading to hydrostatic edema.267, 268 and 269 Loss of autoregulation may be related to extracellular hypercalcemia,270 antiphospholipid antibody related vascular occlusion,271 vasogenic edema269, 272, 273, 274, 275 and 276 perhaps related to inflammatory cytokines of placental origin,277 petechial257 or larger hemorrhages,276 hypertensive encephalopathy,278, 279 ischemia from hypotension during delivery,280 or as part of a postictal state.281
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


