Pediatric Ophthalmology
Edited by P. F. Gallin
Thieme Medical Publishers, Inc.
New York ©2000

3

Practical Pediatric Refraction
Determining refractive errors in children nearly always requires an objective method of measurement. Subjective refractions prior to 10 years of age are unreliable. Although autorefractors are widely available and are commonly used for adult refractions, children have difficulty maintaining consistent central fixation in these instruments, and the measurements are therefore variable. Retinoscopy has been and remains the standard technique for pediatric refractions. It not only provides the desired information about the focus of the eyes but at the same time it allows the examiner to assess the clarity of the cornea and the lens and the quality of the fundus light reflex.
 Central Role of Retinoscopy
Central Role of Retinoscopy
An important advantage of the retinoscope is that the light of the retinoscope can be directed toward the child’s eye and can follow it when the child moves. Fortunately, most children, especially young infants, will look at the retinoscopic light without much prompting. Central fixation is critical for accurate retinoscopy.1 This fact can quickly be appreciated by noting the change in the character of the retinoscopic reflex when the child looks away from the light. With central fixation the corneal reflex is centered in the pupil, except for small displacement due to variations in the anatomic and visual axis, and the fovea is aligned with the retinoscopic beam. In cases of unsteady or eccentric retinal fixation in one eye, this eye can be more accurately refracted by allowing the preferred fellow eye to fix on a distant animated target (e.g., toy or video screen) while the examiner moves to a position from which the corneal reflex of the eccentrically fixing eye is centered in the pupil. In other cases of strabismus, with central and steady fixation in each eye, the eye not being refracted can be occluded by the examiner’s hand or by an occluder in the trial frame while the fellow eye looks directly at the retinoscope (Fig. 3-1). Not only is it critical that retinoscopy be performed in the visual axis but it is also important to read the central portion of the retinoscopic reflex rather than the peripheral reflex, especially when the pupil has been dilated for refraction. The periphery of the reflex may be less hyperopic than the center, exhibiting an “against” movement while the central reflex is still a “with” movement. The central reflex is the more accurate indicator of the true refractive error.2
 Cycloplegia
Cycloplegia
Because the accommodative state of the eye can vary with any change of fixation or attention, cycloplegia is required for pediatric refractions.
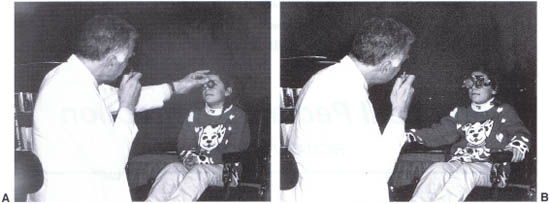
FIGURE 3-1. (A) Retinoscopy being performed on the left eye of a patient while the crossing right eye is occluded by the examiner’s hand. (B) A trial frame with an occluder over one eye can also be used to assure central fixation of the fellow eye on the retinoscope.
Cycloplegia is also required for any refraction under anesthesia because anesthetic agents induce changes in the state of contraction of the pupil and ciliary body at various planes of anesthesia.3 Cyclopentolate is an effective cycloplegic agent for most refractions.4 Two drops of 1% solution in each eye is the usual dose. Stronger concentrations or more frequent applications have been associated with psychic effects, including convulsions. The drug requires approximately 30 minutes to achieve maximum cycloplegia. It is more rapidly effective in blue-rather than brown-eyed patients. One percent atropine ointment is an alternative agent and the standard by which other cycloplegics are measured. It is reliably effective in eyes of any pigmentation and will uncover from one third to one half diopter more hyperopia <than cyclopentolate in hyperopic patients.5 The major disadvantage of atropine is that it has a duration of action of up to 1 week. Tropicamide is effective as a mydriatic agent, but its cycloplegic action is weaker and shorter in duration than that of cyclopentolate.6 All pediatric patients who have an ophthalmic examination should have a cycloplegic examination with retinoscopy and indirect ophthalmoscopy. Anisometropes with attendant amblyopia are often diagnosed in this way, especially in preverbal children in whom a formal visual acuity cannot be obtained. Furthermore, the retina must be inspected for tumors and other anomalies. Partial lens opacities can also be uncovered by this technique.
 Advantage of Trial Frame and Hand-Held Lenses
Advantage of Trial Frame and Hand-Held Lenses
Retinoscopic refractions of young children are best done with hand-held lenses. The spherical and cylindrical lenses can be directly superimposed, making it easy to compare meridians and to refine the axis of astigmatism and to standardize the distance between the vertex of the cornea and the posterior surface of the trial lens. Variations in this distance can significantly alter the spherical power required for neutralization when the ametropia is greater than plus or minus 4 diopters.7 Retinoscopy can, of course, be performed with a phoropter, but positioning the very young pediatric patient behind a phoropter and maintaining this position is difficult. It is not surprising that most pediatric ophthalmology examining lanes do not include a phoropter as standard equipment.
 Hyperopic Corrections
Hyperopic Corrections
Straight-Eyed Hyperopes
When hyperopia is found in a patient whose eyes are straight and binocular, the decision to prescribe glasses depends on the amount of hyperopia and the age of the child. Infants under 1 year of age with 3 or 4 diopters of hyperopia are not generally enthusiastic about wearing glasses, whereas at 4 years they may find correction with glasses quite helpful. Hyperopia of 5 diopters or more is usually corrected whenever it is found, even if the patient is apparently asymptomatic.
Symptoms of reduced visual acuity or blurring in the near range are found only in older children, but when present they should prompt the prescription of a hyperopic correction. It is often theorized that an early glass correction for hyperopia will prevent the development of accommodative strabismus and amblyopia, but controlled trials have failed to show a clear difference in groups of patients managed without spectacles.8 Rather large hyperopic errors found in the early months may diminish or disappear by 1 year of age, so watchful waiting and repeat refraction are appropriate management in this situation.9
On the other hand, hyperopia present after age 1 year may increase with age until approximately the end of the 7th year.10 Beyond age 7 years, hyperopia usually stabilizes or begins to diminish. In the latter case, glass prescriptions must be reduced to avoid blurring at a distance. Straight-eyed hyperopes are usually corrected with something less than their full cycloplegic measurement. This is certainly true if atropine has been used for cycloplegia, but, even if cyclopentolate has been used, one half to one diopter of plus power can be cut when writing a prescription. The same reduction should be made for both eyes.
Hyperopia Associated with Partly or Fully Accommodative Esotropia
When hyperopia is associated with overt esotropia or even large esophoria, a full cycloplegic correction should be prescribed. There is no need to subtract power from a refraction done with cyclopentolate. This is a common error. Because, as mentioned previously, atropine cycloplegia uncovers on average one half diopter more hyperopia than cyclopentolate, one may choose to subtract this amount from the atropine refraction, but in many cases even the full atropine refraction can be given without a postcycloplegic overcorrection.
Esotropia may be caused by a wide range of hyperopic refractive errors.11
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


