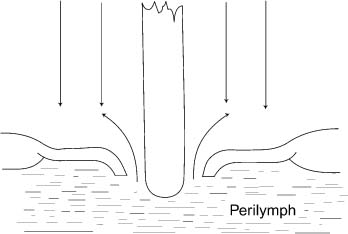
Chapter 12 A perilymph fistula is one of the most common causes of sensorineural hearing loss following stapedectomy. It is thought that perilymph fistulae occur because of inadequate closure of the fenestra in the footplate by the seal, too long a prosthesis, or possibly increased perilymph pressure. The diagnosis and treatment of this condition are vital, because it has the potential to cause irreversible profound sensorineural hearing loss and puts the patient at risk of developing meningitis. Newlands (1976) reported on a patient who developed acute otitis media, labyrinthitis, and meningitis 16 months following stapedectomy. Poststapedectomy carries an increased risk of labyrinthitis and meningitis. Should labyrinthitis occur with or without meningitis, fistula repair must be taken as soon as the infection has been eliminated (Matz et al 1968). Lewis (1961) described perilymph fistula, observing that the polyethylene strut caused perilymph to leak into the middle ear. Perilymph fistulae have been observed with all types of stapes surgeries and with all techniques. The most common symptoms are fluctuating sensorineural hearing loss, roaring tinnitus, and vertigo accompanied by fullness in the ear. These symptoms are also associated with endolymphatic hydrops. The key to making a diagnosis of perilymph fistula, however, is that it occurs following stapedectomy. If it occurs immediately following surgery, the diagnosis of perilymph fistula is obvious. This is termed primary or early perilymph fistula. If instead symptoms occur long after stapedectomy, then establishing a diagnosis of perilymph fistula may not be that easy. This is termed delayed or secondary perilymph fistula. Perilymph fistulae account for 9 to 10% of failures of stapedectomies (Crab-tree et al 1980; Derlacki 1985; Glasscock et al 1987). On the other hand, Feldman and Schuknecht (1970) analyzed 154 revision stapedectomies and reported that perilymph fistulae were found in just 5 cases. The incidence of perilymph fistulae as a cause of failure in stapedectomy is approximately the same for both short- and long-term follow-up (Glasscock et al 1987). Stapedectomy by necessity involves the creation of a fistula for the insertion of the prosthesis. The primary perilymph fistula occurs when the fistula created at the time of surgery persists and fails to seal off the vestibule from the middle ear. This can occur immediately after surgery, and symptoms can persist for days or weeks. The typical symptoms consist of hearing loss, tinnitus, and vertigo. Because these symptoms are also typical of endolymphatic hydrops, an early peri-lymph fistula can be confused with endolymphatic hydrops. The most common symptom in some series is vertigo, whereas in others the most common symptom is a drop or a fluctuation in hearing (Wiet et al 1993). Harrison and colleagues (1967) reviewed 46 cases of poststapedectomy perilymph fistulae and found hearing loss or fluctuating hearing loss to be the most common symptom in 87% of cases. Moon (1970) examined 49 cases of poststapedectomy perilymph fistulae and found that 71% of cases with primary fistulae, and 78% of cases with secondary perilymph fistulae, presented with hearing loss as their chief complaint. Moon also reported that a pure sensorineural hearing loss is the most common type of loss in both primary and secondary fistulae. On occasion, however, mixed hearing losses and pure conductive hearing losses can occur as a symptom of peri-lymph fistula. Goodhill (1967) emphasized that a perilymph fistula may present only as a fluctuating or persistent conductive hearing loss. He postulated that the ratio of the transducer effect of the prosthesis to the peri-lymph spillage effect is less than ideal in such patients, thus accounting for their symptoms. Vertigo may result from semicircular canal disturbances that then result in rotatory vertigo, or it may have a utricular origin, which results in a sense of falling down. Harrison et al (1967) found that 35% of their patients complained of vertigo, and 39% had a sensation of imbalance. Moon (1970) found that 77% of primary fistulae and 61% of secondary fistulae caused disequilibrium. Tinnitus was found in 28% of patients, as reported by Harrison et al (1967). Moon (1970) found tinnitus to be present in 45% of patients who had a perilymph fistula. The signs and symptoms vary with the size of the leak. Large fistulae result in rapid hearing loss, tinnitus, and vertigo. Morrison (1984) noted that such large fistulae accompanied technical difficulties by the operating surgeon at the time of stapedectomy. Fluctuation in hearing loss is unlikely to be a feature in such a situation. In early perilymph fistulae, when the leak is small, the hearing loss may initially appear as a conductive hearing loss; then has a sensorineural component; then progresses to a total sensorineural hearing loss. When such a fistula is repaired late, the hearing does not improve, although vertigo may resolve. When a minute fistula is present, the only evidence of the fistula is failure of a good closure of an air-bone gap, mild fluctuation in hearing, and a small decrease in speech discrimination scores. Figure 12–1 A prosthesis without an adequate oval window seal creates a perilymph fistula. (Adapted from Beales PH. Otosclerosis. Bristol: John Wright and Sons; 1981. Used with permission.) Improperly sealed oval window fenestrae are the most likely cause of such fistulae (Fig. 12–1). Goodhill (1967) stated that if a mucosal seal does not hermetically seal off the vestibule from the middle ear at the time of surgery, then the chances of such a fistula forming are high. Failure to reflect the mucoperiosteal flaps may allow the lacerated edges of tissue to extend down into the vestibule and prevent formation of a new endosteal membrane at the level of the oval window. A prosthesis that is too long will also prevent the fistula from sealing off.
Poststapedectomy Perilymph Fistulae
SIGNS AND SYMPTOMS OF PERILYMPH FISTULA
INCIDENCE
EARLY (PRIMARY) PERILYMPH FISTULA
Signs and Symptoms
Cause of Primary Perilymph Fistula
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


