Posterior Capsulectomy and Anterior Vitrectomy for the Management of Pediatric Cataracts
Rupal H. Trivedi
M. Edward Wilson
Management of the posterior capsule greatly influences the outcome of pediatric cataract surgery (Figs. 20.1, 20.2, 20.3, 20.4, 20.5, 20.6, 20.7, 20.8, 20.9). Visual axis opacification (VAO) is rapid and virtually inevitable in young children when adult-style cataract surgery, leaving the posterior capsule intact, is performed. The younger the child, the more acute the problem, because VAO is faster and the amblyogenic effect is greater. The anterior vitreous face (AVF) is closely linked to the posterior lens capsule and is more “reactive” in infants and young children (Fig. 20.2A and B). The AVF can also serve as a scaffold, not only for lens epithelial cell proliferation but also for metaplastic pigment epithelial cells, exudates, and cells that result from a break in the blood-aqueous barrier. The inflammatory response in small children may be severe, and fibrous membranes may form on an intact AVF, resulting in VAO. The need for posterior capsulectomy and vitrectomy (PCV) has been well recognized in the literature.1,2,3,4,5,6 With the advent of automated vitrectomy techniques in the late 1970s, many pediatric cataract surgeons began to routinely perform PCV with a vitrector.1,7,8,9,10 As of today, a primary PCV are considered “routine surgical steps,” especially in younger children.
In earlier years, surgeons recommended removing all but the peripheral 2 mm of the posterior capsule to minimize postoperative inflammation and VAO when primary intraocular lens (IOL) is not implanted. There was no consideration given for capsular support of a secondary IOL. However, many of these aphakic children may need secondary IOL implantation later. Thus the modern-day challenge is to leave as much capsule as possible in anticipation for future secondary IOL implantation but not so much that the incidence of VAO is too high. Leaving more capsule remnant at the conclusion of cataract surgery provides a more stable platform for a sulcus IOL implantation later, and it also increases the likelihood that secondary in-the-bag IOL placement can be accomplished. However, a larger capsule remnant in an infant will also increase the risk of posterior synechia. With older techniques, there was very little capsule remnant for the iris to adhere to. Also, smaller anterior and posterior capsulectomies make thorough cleaning of cortex from the lens equator more of a challenge. If cortex is not cleaned thoroughly, VAO incidence may increase. For an infant, we recommend a 4 to 4.5 mm round vitrectorhexis (or manual continuous curvilinear capsulorhexis [CCC]) of the anterior and posterior capsules combined with thorough cortical cleanup and a vitrectomy. Matching the anterior and posterior capsulectomy size and shape promote a sealed bag that traps any Soemmering ring formation and enhances the chances for in-the-bag secondary IOL placement years later.
Modern high-quality vitrectomy machines, and the improved visualization provided by the optics of the operating microscopes, have allowed surgeons to perform PCV more safely. In addition, better understanding of the importance of tight fitting wounds around instruments that enter the eye of a child has helped reduce the anterior chamber instability that can occur during these surgical maneuvers in young eyes. Despite this, various questions for the surgeon remain. When should the posterior capsule be opened and when can it be left intact? When does an anterior vitrectomy need to be added to the posterior capsulectomy and when can manipulation of the vitreous be avoided? Is it best to perform posterior capsulectomy and anterior vitrectomy before or after an IOL is implanted? Is the anterior (limbal) or the posterior (pars plana/pars plicata) approach preferred for PCV? In this chapter we address some of these controversial issues.
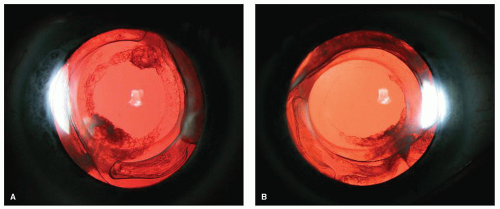 Figure 20.1. Eight-year postoperative picture of a child operated for cataract surgery with vitrectorhexis, posterior capsulectomy/vitrectomy, and SA60AT IOL. A: Right eye. B: left eye. |
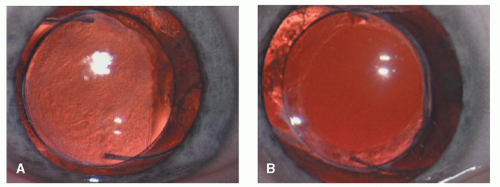 Figure 20.2. A five-and-a-half-year-old child operated for bilateral cataract and IOL implantation. The right eye received posterior capsulectomy (but no vitrectomy), and the left eye received PCV. At 18 months postoperatively, the right eye was noted to have translucent opacification of the visual axis (A) and the left eye was clear (B). |
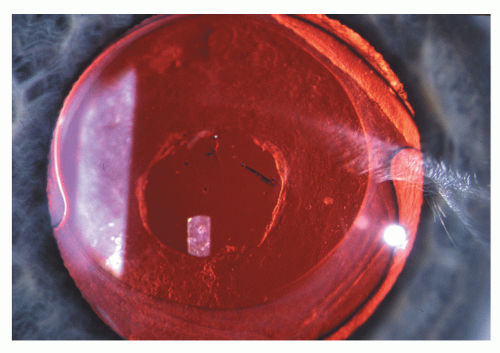 Figure 20.3. Nd:YAG laser has been successfully accomplished in this child’s eye returning the visual acuity to 20/20. |
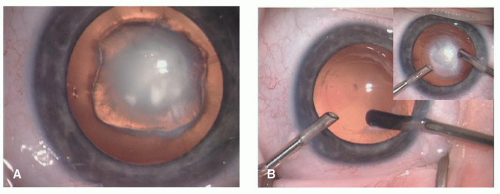 Figure 20.4. A 3-month-old child operated for cataract surgery. A: Preoperative appearance. B: Surgical photos. Note dense plaque on posterior capsule (inset). As IOL implantation was not the intended management for this eye, the limbal approach was used. A large posterior capsulectomy was required to encompass the plaque. If IOL implantation had been intended, we would have used the pars plicata approach in this eye (after IOL implantation). |
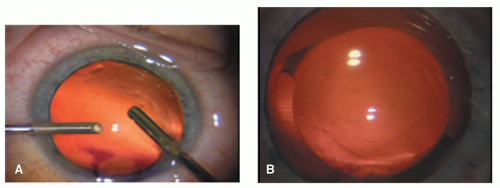 Figure 20.5. Limbal-approach PCV. A: Note smaller opening of posterior capsule (than anterior capsule) and B: well-centered IOL. |
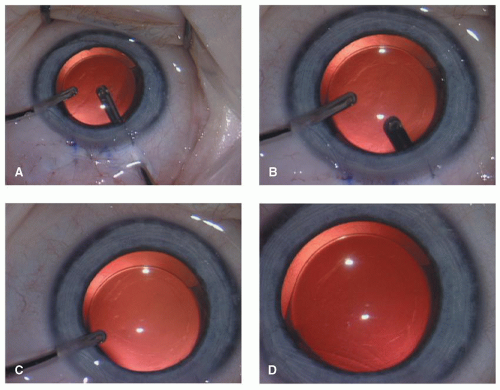 Figure 20.6. Pars plana PCV (after IOL implantation). A: The vitrector has been placed 2.5 mm posterior to the limbus. B: A round posterior capsulectomy is made with cutting port facing anterior. C: Irrigation is from an anterior approach. D: The completed surgery reveals a well-centered posterior capsulectomy and a capsular-fixated IOL. |
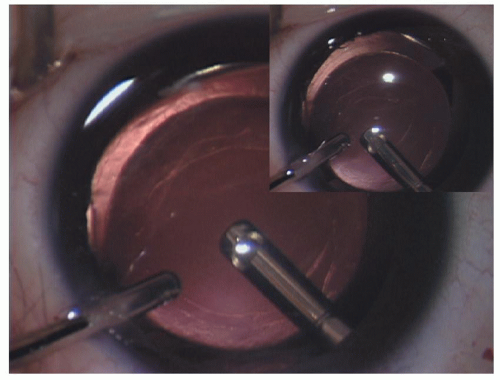 Figure 20.7. Pars plana posterior capsulectomy and anterior vitrectomy after IOL implantation. (Main figure photo shows vitrectomy being performed after completion of posterior capsulectomy) (inset shows capsulectomy being enlarged in a circular fashion by the cutter in the vitrector handpiece). |
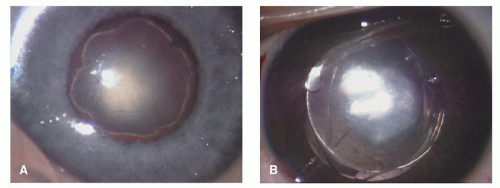 Figure 20.8. In the presence of a dense plaque (A), it is better to perform the PCV after IOL placement (B). |
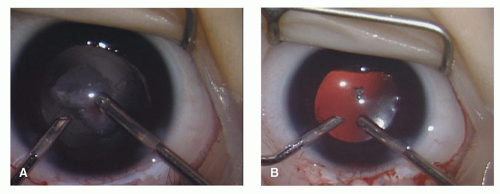 Figure 20.9. Vascularized plaque in an eye with persistent fetal vasculature (A). In this case, the IOL was placed in the ciliary sulcus with the optic captured in the anterior capsulectomy, since most of the posterior capsule had to be removed to clear the plaque. Bleeding from the fetal vessels cleared spontaneously in the first postoperative week (B). |
WHEN SHOULD THE POSTERIOR CAPSULE BE LEFT INTACT?
This is perhaps one of the most common questions. The answer depends mainly on the age at cataract surgery but also on the condition of the posterior capsule and the child’s presumed cooperation for YAG laser capsulotomy in the future. Proponents of primary PCV argue that performance of these steps is a necessity in all children within the amblyopic ages to prevent VAO and worsening amblyopia. However, opponents argue that it is not a safe choice. The posterior capsule is a physiologic barrier between the anterior and the posterior segment of the eye and should not be removed. It prevents the vitreous from entering the anterior chamber, and theoretically preserves the ocular anatomic relationship and the blood-aqueous barrier after cataract surgery. Despite this controversy, PCV are viewed by most pediatric surgeons as necessary steps for the best outcome from cataract surgery in young children. Using currently available IOLs, visually significant posterior capsule opacification (PCO) develops most commonly about 18 months to 2 years after surgery when the posterior capsule is left intact in children older than 5 years of age. Therefore the posterior capsule can be left unopened if it is anticipated that the child is cooperative for slit-lamp examination before cataract surgery, which may be an indication that the child would be cooperative for a YAG laser capsulotomy 18 months to 2 years after surgery. One-third or more YAG laser capsulotomies close spontaneously when performed in young children (<6 years of age or so). The practice of leaving the posterior capsule intact in all children at the time of surgery and bringing them back to the operating room 6 weeks later for a YAG laser capsulotomy has also been described, but did not find widespread acceptance because of the recurrence of VAO. Vertically mounted YAG lasers designed for use in the operating room are now difficult to find because of their infrequent use.
Generally speaking, the posterior capsule can be left intact when children present for cataract surgery at age 8 years or older. A primary PCV should be performed even for older children if YAG laser availability is in question, a posterior capsule anomaly (plaque, defect, etc.) is present, or the child is developmentally delayed or uncooperative for YAG laser capsulotomy.
DO I NEED TO PERFORM AN ANTERIOR VITRECTOMY WHENEVER I PERFORM A POSTERIOR CAPSULECTOMY?
In general, in patients up to 5 years of age, this is an essential step, since vitreous face opacification is likely to occur if an anterior vitrectomy is not performed. However, in children between 5 and 8 years of age, it is an optional step since the chances are better that a posterior capsulotomy (posterior capsulorhexis) alone may result in a long-term clear visual axis. Nonetheless, surgical or YAG laser may be needed secondary to vitreous face opacification.
HOW SHOULD I TREAT THE POSTERIOR CAPSULE? SO MANY OPTIONS: WHICH TO CHOOSE?
Various options are available for PCV in children. Selection among the various technical alternatives is probably best left to the individual surgeon’s preference based on the individual case, available facilities, individual circumstances, and personal experience.
Primary Capsulectomy Versus Secondary Capsulectomy
Posterior capsulectomy may be performed at the time of cataract removal or secondarily. As mentioned previously, most pediatric cataract surgeons now prefer to manage the posterior capsule at the time of cataract surgery. Parks1,10 was an early proponent of primary PCV. He stated, “It should be abundantly clear that the best visual acuity in patients with intractable amblyopia is usually far worse than the best acuity in recovered clinically significant cystoid macular oedema (CME).” He further asked, “How can invasion of the vitreous during a secondary procedure to open the translucent membraneous posterior lens capsule be less likely to cause CME than opening the posterior capsule during the primary lens surgery?” CME turned out to occur much less frequently in children after PCV than originally feared. Remarkably, retinal detachment rates have also been very low after this procedure, owing in part to the formed vitreous of the child’s eye. With the advent of higher-quality vitrectomy machines and sharp, high-speed cutting handpieces, the procedure is even safer than when Parks and others popularized it. We recommend continuing to treat the posterior capsule as a primary procedure in young children until a method is developed to predictably kill residual lens epithelial cells and reduce the likelihood of postoperative VAO.
Surgical Capsulectomy Versus YAG Laser Capsulotomy
Nd:YAG laser capsulotomy can be used as a primary or secondary posterior capsulotomy (Fig. 20.3). Although YAG lasers were most commonly used to perform secondary capsulotomy, it became possible to perform primary capsulectomy with the advent of YAG lasers mounted vertically and used with patients in the supine position. These instruments are rarely used today and are manufactured in small numbers if at all. Table 20.1 lists the pros and cons of both techniques.
In 1985 Maltzman et al.11 described the outcome of YAG laser capsulotomy for secondary membranes in the
pediatric population by using a standard office-based laser delivery system. However, this approach cannot be used for young or uncooperative children. A headrest was designed by Kaufman (cited in Ref.11) for patients placed in the lateral decubitus position. This headrest allowed for treatment of anesthetized children, but it has not come into wide use. The Microruptor III laser system allows for controlled laser procedures in supine anesthetized patients and offers the advantage of being familiar to most surgeons.
pediatric population by using a standard office-based laser delivery system. However, this approach cannot be used for young or uncooperative children. A headrest was designed by Kaufman (cited in Ref.11) for patients placed in the lateral decubitus position. This headrest allowed for treatment of anesthetized children, but it has not come into wide use. The Microruptor III laser system allows for controlled laser procedures in supine anesthetized patients and offers the advantage of being familiar to most surgeons.
Table 20.1 SURGICAL VERSUS Nd:YAG LASER POSTERIOR CAPSULOTOMY | ||||||||
|---|---|---|---|---|---|---|---|---|
|
Atkinson and Hiles,12 in 1994, reported leaving the posterior capsule intact and performing Nd:YAG capsulotomy under a second general anesthesia in the early postoperative period. Hutcheson et al.13 examined the clarity of the visual axis after Nd:YAG laser capsulotomy following cataract extraction and primary IOL implantation in a pediatric population. One eye (3%) in primary surgical PCV experienced postoperative VAO. Thirteen (57%) of 23 eyes in Nd:YAG laser capsulotomy group experienced reopacification, requiring retreatment. Four eyes (17%) treated with Nd:YAG laser required a third treatment. Stager et al.14 reported rates of PCO following foldable acrylic IOL implantation. The authors noted that 60% of the eyes developed recurrent opacification following Nd:YAG laser treatment in the younger age group (<4 years), which suggested that surgical PCV, rather than YAG laser capsulotomy, may be needed in these young children to keep the visual axis clear.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


