Role of Intraocular Lens Optic Capture in Pediatric Cataract Surgery
Abhay R. Vasavada
Rupal H. Trivedi
Sajani K. Shah
Vaishali A. Vasavada
Improvements in surgical techniques and technologies have helped us to provide better surgical outcomes for cataract surgery in children. However, visual axis obscuration (VAO) remains one of the major hurdles that impede successful visual rehabilitation following pediatric cataract surgery. Posterior capsulorhexis and anterior vitrectomy are considered standard surgical steps for infants and young children undergoing cataract surgery to prevent VAO. In 1994, Gimbel and DeBroff described a posterior “optic capture” technique for pediatric cataract surgery that they proposed would maintain a clear visual axis and eliminate the need for vitrectomy.1
The concept of capturing an intraocular lens (IOL) optic through an anterior capsulorhexis was first suggested in a case of posterior capsule tear in an adult eye. The IOL haptics were placed in the ciliary sulcus, and the IOL optic was placed through the anterior capsulorhexis to “capture” the optic and ensure stable optic fixation. The concept was subsequently described as “optic capture,”1,2,3,4,5,6,7,8,9,10,11,12,13,14,15 “optic entrapment,”15 or “optic buttonholing.”16,17,18,19,20,21,22,23
Optic capture fuses the anterior and posterior leaflets of the capsular bag almost completely in a 360-degree position, except at the haptic-optic junction. Theoretically, capsular fusion anterior to the IOL optic reduces central lens epithelial cell migration or at least directs the cell movement anteriorly over the lens optic, which is presumably an unsuitable substrate for lens survival. Thus, capsular fusion may help in decreasing VAO. Another advantage of performing optic capture is its ability to achieve a well-centered IOL.1,7
There are several possible sites for optic capture (Fig. 26.1). Conventional (or posterior) optic capture techniques utilize the posterior capture technique. Here, the optic is captured through the anterior capsulorhexis (haptics in the ciliary sulcus, optic in the bag), through the posterior capsulorhexis (haptics in the bag, optic in the vitreous), or through both the rhexes (haptics in the ciliary sulcus, optic in the vitreous). Optic capture can be helpful for both primary and secondary IOL implantation.7,24
CAPTURE THROUGH POSTERIOR CAPSULORHEXIS (HAPTICS IN THE BAG, OPTICS BEHIND THE POSTERIOR CAPSULE)
Before moving forward, it is worth noting that IOL power may need to be adjusted 0.5 to 1 diopter higher than for bag-fixated IOLs. The success of optic capture technique may depend on the IOL haptic-optic junction design.13 For example, a haptic with a right angle at the haptic-optic junction is preferred for optic capture as it helps in achieving complete capsule closure.
Technique
Following manual anterior continuous curvilinear capsulorhexis and irrigation/aspiration of lens material, a continuous manual posterior continuous curvilinear capsulorhexis (PCCC) is performed (Fig. 26.2). Under a high-viscosity ophthalmic viscosurgical device (OVD), the IOL is implanted in the capsular bag. Thereafter, the IOL optic is gently pressed backward and is captured through the posterior capsulorhexis using a spatula/Leister hook (Fig. 26.3). The haptics are placed in the capsular bag fornix. If the round opening is stretched into an elliptical one, it indicates complete capture (Fig. 26.4).
Optic capture is a technically challenging procedure. The key point is to achieve a “capturable” PCCC. Although there are several options for performing PCCC, a manual PCCC is a prerequisite for optic capture of the IOL through the PCCC. The opening in the posterior capsule should be not only continuous
but also well centered and of an optimum size. If the opening is too small, it is difficult to capture the optic, and there is the possibility of tearing the posterior capsule due to excessive stress to the PCCC edge. On the other hand, if it is too large, the optic may not remain captured. Thus, creating an opening of an optimum size is a prerequisite for successful optic capture. The diameter of the PCCC opening should be approximately 1.0 mm smaller than the IOL optic. The principle behind the use of this technique is to avoid the need for vitrectomy. However, occasionally, the vitreous face is disturbed while performing primary PCCC or capturing the IOL optic, and an unplanned vitrectomy may be required.
but also well centered and of an optimum size. If the opening is too small, it is difficult to capture the optic, and there is the possibility of tearing the posterior capsule due to excessive stress to the PCCC edge. On the other hand, if it is too large, the optic may not remain captured. Thus, creating an opening of an optimum size is a prerequisite for successful optic capture. The diameter of the PCCC opening should be approximately 1.0 mm smaller than the IOL optic. The principle behind the use of this technique is to avoid the need for vitrectomy. However, occasionally, the vitreous face is disturbed while performing primary PCCC or capturing the IOL optic, and an unplanned vitrectomy may be required.
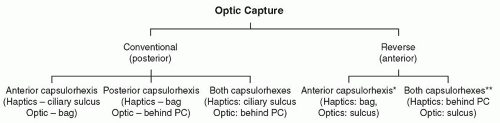 Figure 26.1. Schematic diagram showing different sites for capturing the IOL optic. *In the case of a large posterior capsule tear noticed after IOL implantation and in-the-bag fixation; not considered stable. **In the case of posterior dislocation (pars plana repositioning of an IOL). |
Removal of the OVD may sometimes cause the optic to vault forward. This vaulting can undo the optic capture.
IOL CAPTURE THROUGH BOTH CAPSULORHEXIS (HAPTICS IN THE CILIARY SULCUS, OPTIC BEHIND THE POSTERIOR CAPSULE)
The surgeon may consider this technique as an alternative to sulcus IOL placement in those cases in which the anterior capsulorhexis has more than one large tear to the equator of the capsule that compromises the secure placement of the haptics in the capsular bag. In addition, an intact PCCC must be present. In such a situation, the surgeon may position the IOL in the ciliary sulcus and capture the optic posteriorly through the anterior and posterior capsulorhexis openings. This approach maintains IOL centration and prevents Elschnig pearl formation posterior to the IOL. IOL decentration is the most common complication in eyes with secondary IOL implantation. Optic capture through fused anterior and posterior capsulorhexis (haptics in the ciliary sulcus) may help to avoid IOL decentration postoperatively.24
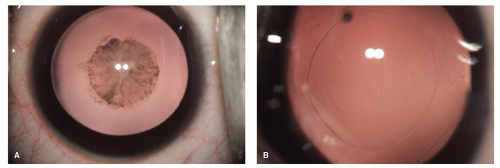 Figure 26.2. A: Lamellar cataract. B: Optimum-sized anterior continuous curvilinear capsulorhexis and PCCC. |
REVERSE OPTIC CAPTURE (HAPTICS IN THE BAG, OPTICS IN THE SULCUS)
Bringing the optic of the IOL anteriorly through the anterior capsulorhexis opening effectively achieves a reverse capsulorhexis fixation. This technique is useful when a radial tear of the PCCC occurs that renders the IOL unstable within the capsular bag. The surgeon may then bring the optic of the IOL forward and capture it through the anterior continuous curvilinear capsulorhexis, thus creating IOL stability and ensuring lens
centration. This technique is reported to be useful to resolve pseudophakic negative dysphotopsia in the adult population.25 This technique can also be useful for piggyback IOL implantation. In this technique, haptics of both piggyback IOLs remain in the bag. The anterior IOL optic is pulled out of the bag for reverse optic capture (the posterior IOL optic remains in the bag). This approach may reduce the accumulation of pearls in the interface between the two IOLs (interlenticular opacification), while maintaining bag fixation of the second IOL.
centration. This technique is reported to be useful to resolve pseudophakic negative dysphotopsia in the adult population.25 This technique can also be useful for piggyback IOL implantation. In this technique, haptics of both piggyback IOLs remain in the bag. The anterior IOL optic is pulled out of the bag for reverse optic capture (the posterior IOL optic remains in the bag). This approach may reduce the accumulation of pearls in the interface between the two IOLs (interlenticular opacification), while maintaining bag fixation of the second IOL.
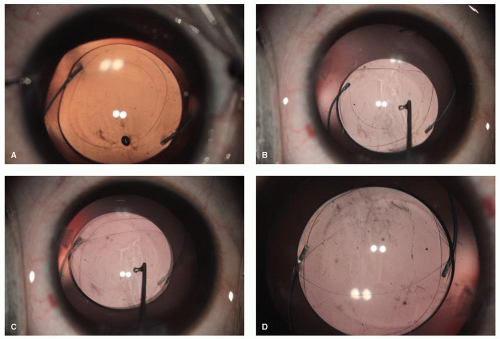 Figure 26.3. A: A three-piece hydrophobic acrylic IOL placed in the capsular bag. B and C: Using Leister hook, the IOL is pressed backward and captured through the PCCC. D: Optic capture of IOL through the PCCC. |
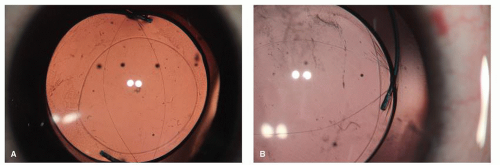 Figure 26.4. A: Successful optic capture of IOL indicated by elliptical shape of the PCCC. B: Striations at the optic-haptic junction. |
PERIOPERATIVE OUTCOMES OF OPTIC CAPTURE OF THE IOL
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


