Etiology and Morphology of Pediatric Cataracts
M. Edward Wilson
Rupal H. Trivedi
Suresh K. Pandey
William J. Johnson
Childhood cataracts can be classified as congenital, infantile, or juvenile, depending on the age at onset. Congenital cataracts are present at birth but may go unnoticed until an effect on the child’s visual function is noticed or a white pupil reflex develops. Infantile cataracts develop in the first 2 years of life, and juvenile cataracts have an onset within the first decade of life.1,2 The term presenile cataract is sometimes seen in the literature. This term refers to cataracts with an onset prior to 45 years of age. Age-related or what has historically been called “senile” cataracts occur at or after age 45 years. Childhood cataracts can also be classified according to etiology (e.g., hereditary cataract, traumatic cataract) or morphology.3,4,5,6,7 Childhood cataract and lens-related pathology can have widely different appearance (Figs. 2.1, 2.2, 2.3, 2.4, 2.5, 2.6, 2.7, 2.8, 2.9, 2.10, 2.11, 2.12, 2.13, 2.14, 2.15, 2.16, 2.17, 2.18, 2.19, 2.20, 2.21, 2.22, 2.23, 2.24, 2.25, 2.26, 2.27, 2.28, 2.29, 2.30, 2.31, 2.32, 2.33, 2.34, 2.35, 2.36, 2.37, 2.38, 2.39, 2.40).
ETIOLOGY OF PEDIATRIC CATARACTS
It is important to consider the origin of a cataract. The common teaching for many years has been that roughly one-third of childhood cataracts are inherited, one-third are associated with other diseases or syndromes (Figs. 2.6 and 2.40), and the remaining one-third are idiopathic. However, the rate of idiopathic congenital cataracts has been reported as high as two-thirds.8 The etiology of pediatric cataracts has been reviewed by several authors, and several classifications have been proposed.2,3,9 The etiology of pediatric cataracts can be broadly classified and summarized in the following subgroups.
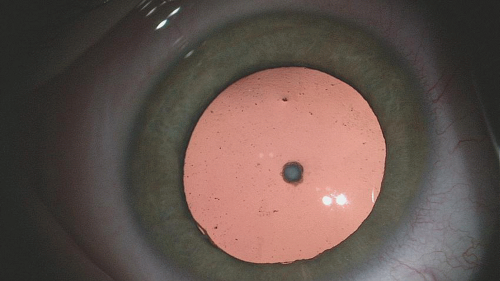 Figure 2.1. Anterior polar cataract in the right eye of a 12-year-old child. |
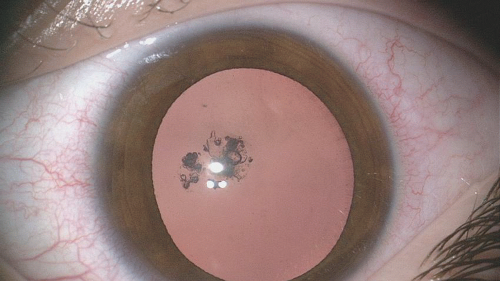 Figure 2.2. Mild posterior capsular cataract in a 9-year-old child. |
Hereditary Cataracts
Hereditary cataracts are passed from one generation to the next. Autosomal dominant transmission is responsible for 75% of congenital hereditary cataracts. Affected individuals are usually otherwise perfectly well and have no associated systemic illness. Less commonly, the inheritance may be autosomal recessive. These cataracts are bilateral but may be asymmetric. Also, marked variability can be seen between affected family members. Some cataracts are so mild that family members do not know they have them.
There are also a number of rare hereditary syndromes in which the affected individual not only has cataracts but also has an associated systemic illness. Cataracts may be associated with renal and cerebral disease as in the X-linked oculocerebrorenal syndrome of Lowe.
An examination by a developmental pediatrician and/or a clinical geneticist is important for children with bilateral cataracts to help detect any associated systemic disorder. Genetic disorders linked to cataracts are Norrie disease, Peters anomaly, etc. (see Chapter 1).
An examination by a developmental pediatrician and/or a clinical geneticist is important for children with bilateral cataracts to help detect any associated systemic disorder. Genetic disorders linked to cataracts are Norrie disease, Peters anomaly, etc. (see Chapter 1).
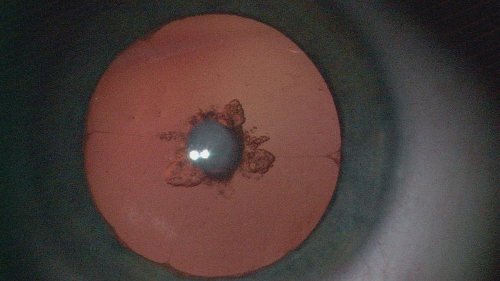 Figure 2.3. Visually significant anterior polar cataract in a 2-year-old child. |
 Figure 2.4. Anterior polar cataract in a 2-year-old child. Cataract had progressed to involve a portion of the surrounding cortex. |
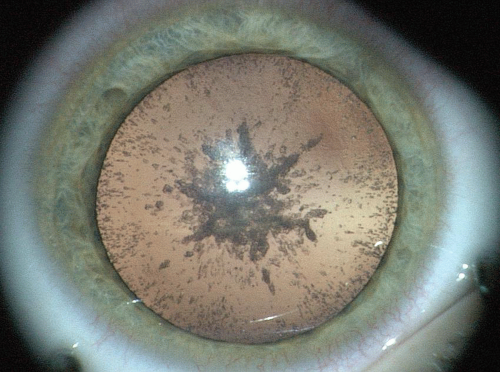 Figure 2.5. Slowly progressing cataract in a 13-year-old child. |
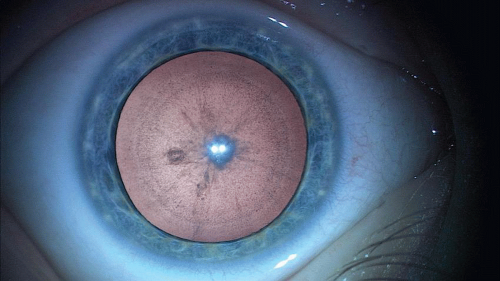 Figure 2.6. Cataract in an 18-year-old child with Down syndrome. |
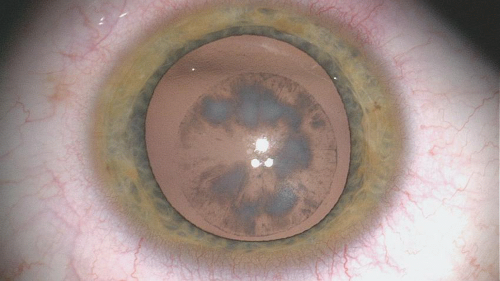 Figure 2.7. Lamellar cataract. |
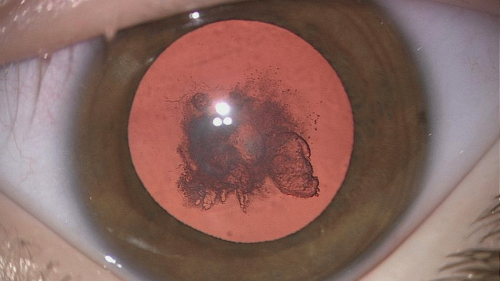 Figure 2.8. Nuclear and cortical cataract. |
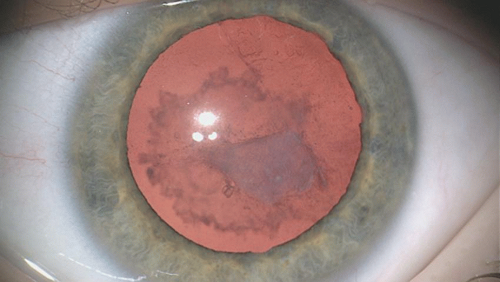 Figure 2.9. Traumatic cataract in a 6-year-old boy. History of blunt trauma 2 months ago. |
 Figure 2.10. An 8-year-old child with cataract and fibrotic posterior capsule. |
 Figure 2.11. Cataract in a 1-month-old child. Posterior capsule plaque was noted at the time of cataract surgery. |
 Figure 2.12. Congenital nuclear cataract associated with posterior capsule plaque in a 4-month-old child. |
 Figure 2.13. Four-year-old child with history of bilateral cataract. |
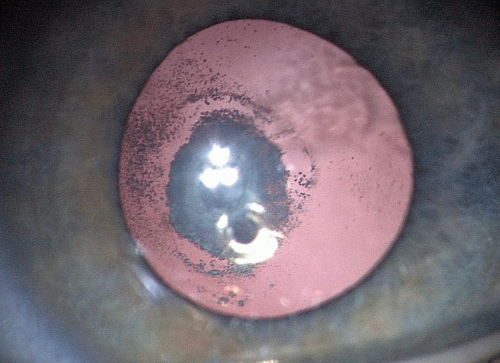 Figure 2.14. Visually significant cataract in the right eye of a 6-year-old girl. Cataract was diagnosed after failed vision screening in the school. The cataract involved at the posterior capsule and that lens material was in the vitreous. |
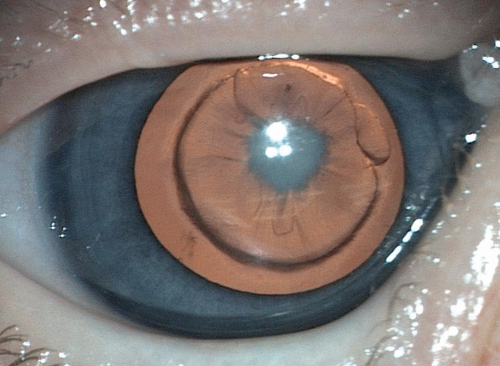 Figure 2.15. Visually significant unilateral cataract in the left eye of a 6-week-old infant. The child was noted to have a posterior cortical opacity with a posterior capsule plaque and an evolving fetal nuclear opacity as well. |
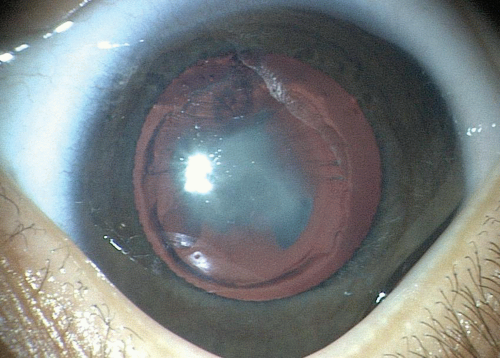 Figure 2.16. Visually significant cataract in a 1-month-old child. The cataract was nuclear and with advancing cortical spread and posterior capsule plaque. |
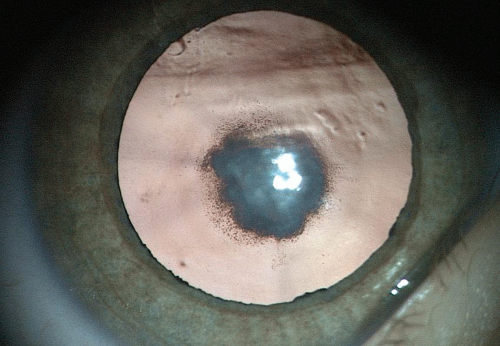 Figure 2.17. Slowly progressive posterior cataract in the left eye of a 3-year-old child. |
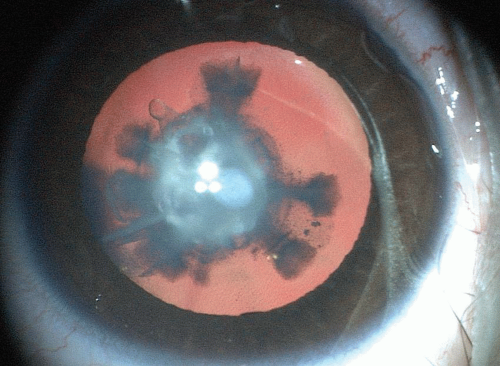 Figure 2.18. Dense nuclear and cortical cataract in a 2-year-old child. |
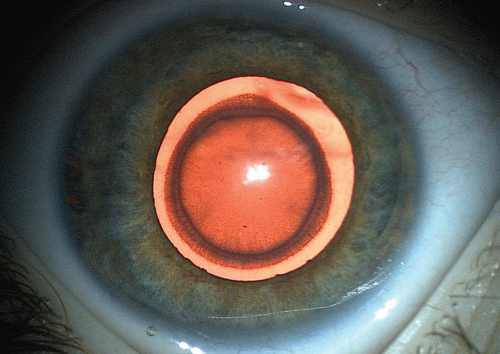 Figure 2.19. Lamellar cataract in a 3-year-old child with ocular albinism. |
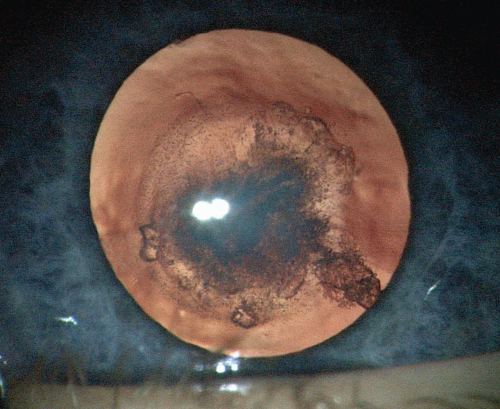 Figure 2.20. Congenital capsular and subcapsular cortical cataract in right eye of a 14-month-old child. |
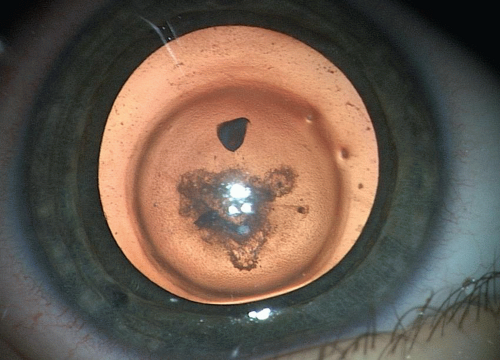 Figure 2.21. Cataract in the left eye of a 10-month-old child. |
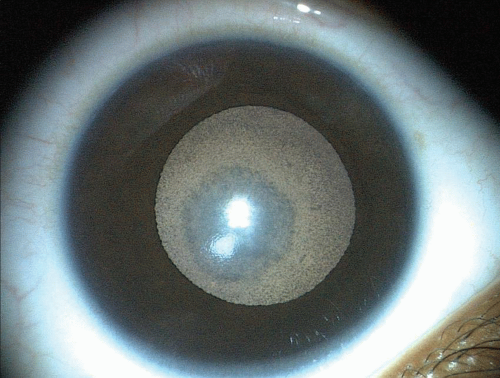 Figure 2.22. Cataract in an eye with semidilated pupil. |
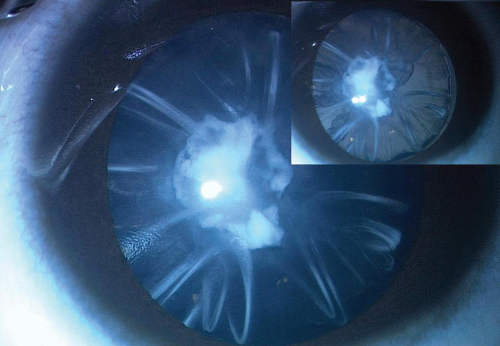 Figure 2.23. Dense cataract in a 23-month-old child. |
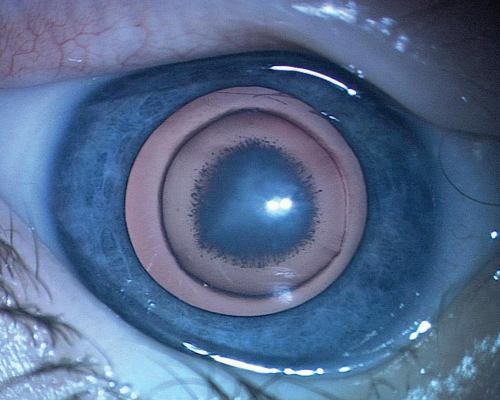 Figure 2.24. Central nuclear cataract in a 6-week-old child. |
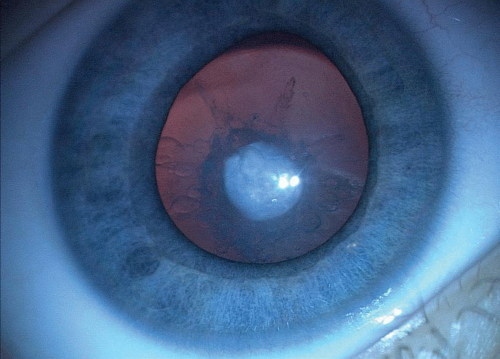 Figure 2.25. Cataract in 1 year in a 10-month-old child. The child had anterior polar cataract in both eyes; however, in this left eye, cataract has grown and spread throughout the cortex. |
 Figure 2.26. Cataract in a 6-month-old child. Cataract was posteriorly located with spread in the cortex. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


