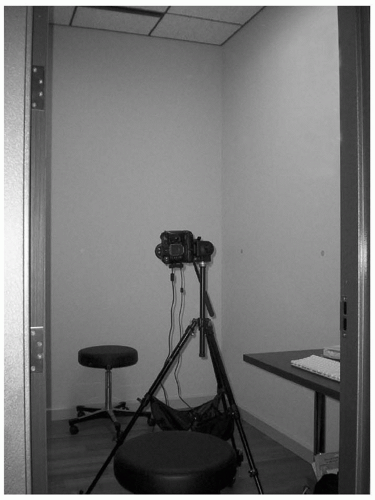
 Figure 171.1 Standardized photography requires a dedicated photography room where all pre- and postoperative photographs are taken. A rotating stool with a low or no back is used to rotate the patient’s entire body to the prescribed angle for each view. The digital camera is mounted on a tripod with a quick-release head that can easily adjust from a vertical to a horizontal frame position. In turn, the tripod rests on a rolling dolly to facilitate maneuverability. Markers have been placed on the wall to guide the patient how far to rotate the body in the oblique and lateral positions. In this setup, the back leg of the patient’s stool contacts the wall, and the tripod’s center frame is aligned with the edge of the computer table in order to maintain a standardized camera-to-subject distance. (If flash photography were used, the patient should not be so close to the wall to avoid harsh background shadows.) The back wall is painted a light blue color as a neutral background color. |
addition to distortion of the neck, over- or underrotation of the neck can cause the nose to appear erroneously rotated or derotated, respectively, and would compromise any photography for rhinoplasty (Fig. 171.3). Patients may also reflexively attempt to lift their brow if they have significant brow ptosis, making the pre- and postoperative result for browlift or upper blepharoplasty less meaningful. If the patient exhibits this behavior, the photographer should ask that the patient close his or her eyes forcefully and slowly open them until they appear fully open. This maneuver will help break the unwitting contribution of the frontalis muscle. The patient may also instinctively smile when posing for a photograph, so the photographer should gently remind the patient that no facial expression should be displayed.
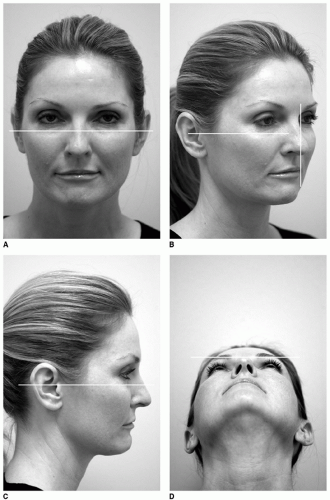 Figure 171.2 Standardized photographic views that show (A) frontal, (B) right oblique, (C) right lateral, and (D) basal of the patient. The horizontal line drawn in A-C indicates the Frankfort Horizontal Plane that runs through the supratragal point and the inferior orbital rim, which should be respected. The horizontal line in D shows the alignment of the nasal tip with the infrabrow line. The vertical line in B shows the alignment of the nasal tip with the malar eminence. |
 Figure 171.3 Poor patient positioning is shown with the neck overrotated and extended that leads to distortion of the neck as well as for the nose, as seen from the frontal view (A) and from the profile view (B). |
45 degrees in front on both sides of the patient can be further softened by aiming the lights away toward reflective umbrellas. A “kicker” light placed behind the patient can fill in any remaining shadows cast by the two forward placed 45-degree lamps and slaved to go off when the camera’s shutter is depressed (Fig. 171.4). Placing the patient an appropriate distance away (˜2 feet) from the rear wall can also minimize unwanted shadows. Generally, an oncamera flash tends to cause excessive highlights and shadows and a “washed-out” appearance to skin tones, but experimentation will determine the best balance of lighting for a particular room and camera. Rather than use fill lights or strobes, the ambient lighting and the camera’s aperture/exposure can be adjusted to achieve the desired lighting objective. Furthermore, the ambient room lighting can be altered to match the color spectrum (e.g., daylight balanced) of the film used or the settings of the camera so that, for example, a green cast from fluorescent lights may be avoided. If shadows and highlights are desired in order to accentuate a scar or other contour irregularity, for example, prominent nasolabial lines for correction with a soft tissue filler, then the balanced fill lights (if used) should be turned off. In addition, the exposure value can be reduced in order to draw out the intended feature. Obviously, the same settings should be used for the postoperative views.
TABLE 171.1 RECOMMENDED, STANDARDIZED PHOTOGRAPHIC VIEWS FOR SPECIFIC FACIAL PROCEDURES | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|



