(A) Rhinitis
(B) Photic sneeze reflex (ACHOO syndrome)
(C) Physical stimulations of the trigeminal nerve
(D) Central nervous system pathologies
(E) Psychogenic (intractable) sneezing
(F) Snatiation* reflex
(G) Sexual ideation or orgasm
11.3.1 Rhinitis
It is the inflammation of the nasal mucosa causing nasal stuffiness, rhinorrhea, nasal pruritus, and sneezing (Bousquet et al. 2001).
11.3.1.1 Allergic Rhinitis
Allergic rhinitis is the inflammation of the mucosa lining the nasal cavity in the form of IgE-dependant type I hypersensitivity reaction (Bousquet et al. 2001). Allergic rhinitis is a common disorder, which represents a considerable burden both on individual patients and on society (Ozdoganoglu and Songu 2012; Cingi et al. 2010b). Itching and sneezing represent two of the main bothersome symptoms, apart from nasal obstruction and rhinorrhea in allergic rhinitis (Ozdoganoglu et al. 2012). In allergy-related nasal inflammation, it can be demonstrated that especially the neurotransmitter SP is released by C-fibers (Ader et al. 1995; Kim and Baraniuk 2007). SP is significantly increased in the nasal lavage of patients with allergic rhinitis, in contrast to healthy subjects, which is interpreted as a sustained stimulation of the sensory system (Klimek and Schäfer 1996). Exogenically administered SP results in a dose-dependent occurrence of nasal symptoms in asymptomatic patients with allergic rhinitis and controls, without elevation of inflammatory mediators. In addition to SP, other neuropeptides, including calcitonin gene-related peptide (CGRP) and vasoactive intestinal polypeptide (VIP), are increased in nasal lavage fluids after nasal provocation in allergic rhinitis (Mosimann et al. 1993). An important feature of allergic rhinitis is hyper-responsiveness influenced by products of the allergic reaction including eicosanoids; cytokines such as IL-6, Il-1β, and TNF-α; and, most importantly, neurotrophins including nerve growth factor (NGF) and brain-derived neurotrophic factor (BDNF). NGF targets nociceptor fibers, leading to upregulated activity, increased SP content, and dendrite sprouting (Levi-Montalcini 1987). The allergen-induced increased BDNF expression in the nasal mucosa significantly correlated with the maximal increase of total nasal symptom score in allergic rhinitis (Raap et al. 2008) (Fig. 11.1).
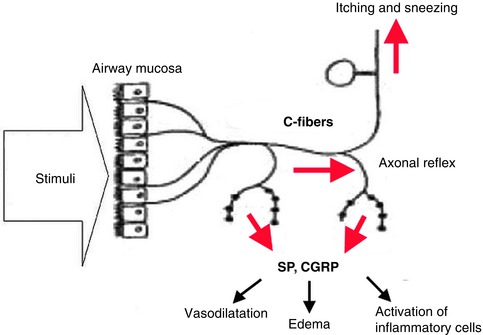
Fig. 11.1
Schematic presentation of the processes involved in “neurogenic inflammation” leading to itching and sneezing. Activation of afferent trigeminal C-fibers by several stimuli including allergen contact may result in an efferent liberation of substance P (SP) and calcitonin gene-related peptide (CGRP) via axonal reflex. This further leads to vasodilatation, edema, and recruitment/migration of inflammatory cells
11.3.1.2 Infectious Rhinitis
In more than 50 % of cases, rhinovirus is the responsible agent for common cold (nasopharyngitis) which is the most common clinical form of viral infections. Inhalation, close contact with the infected person, contact with the objects contaminated with the virus such as door handles, school desks, household goods or phones, are all ways of contracting the virus. The most common prodromal manifestations include high fever, nasal irritation, and sneezing. Nasal symptoms are also present in influenza (flu) caused by influenza virus; however, they are likely to be overshadowed by malaise, fatigue, myalgia, and high fever. Bacteria may infiltrate the tissue and cause infections during the course of viral rhinitis due to impairment of mucosal integrity and ciliary function. Clinical picture of rhinitis may occur during the course of specific bacterial diseases such as diphtheria, rhinoscleroma, lepra, tuberculosis, syphilis, and glanders. Opportunistic fungal infections which develop in AIDS, chemotherapy, prolonged intensive care unit stay, and disorders of neutrophil number and function such as neutropenia and diabetes may cause rhinitis.
11.3.1.3 Nonallergic Noninfectious Rhinitis
Every sneezing paroxysm does not mean an allergic rhinitis or common cold. There are also many rhinitis clinical pictures of unknown etiology that may cause sneezing and are classified as “nonallergic noninfectious rhinitis.” The commonly observed clinical pictures in this group are NARES and vasomotor rhinitis and are usually confused with allergic rhinitis.
11.3.1.3.1 NARES (Nonallergic Rhinitis with Eosinophilia Syndrome)
It is a nasal hyperreactivity syndrome, manifested by sneezing paroxysms and watery discharge followed by nasal stuffiness and hyposmia in which the increased eosinophil count exceeds 20 % of total leukocyte number in the absence of an IgE-dependant allergy (Dykewicz et al. 1998). The suspected etiology is the infiltration of circulating eosinophils into the site of inflammation because of the increased level of substance P as a result of alterations within the nasal mucosa due to irritation, senility, or other factors.
11.3.1.3.2 Idiopathic (Vasomotor/Nonallergic and Non-eosinophilic) Rhinitis
It is a short course hyperreactive nasal mucosal disease of sudden onset manifested by nasal stuffiness, watery nasal discharge or postnasal drip, and sneezing. Eosinophilia is not found in nasal secretions and allergy tests are negative. The most important clinical feature that differentiates vasomotor rhinitis from NARES is the sudden onset of the symptoms which relieve immediately following disappearance of triggering factors. Environmental factors including cold and dry air, high amount of moisture, dyes, chlorine water, perfume, tangs, cigarette smoke, exhaust gas, and other inhaled irritants may initiate the symptoms of vasomotor rhinitis. A typical example is a sudden onset of nasal stuffiness and short-lasting though forceful sneezing paroxysm in the morning time after being exposed to cold and dry air. Individual factors such as fatigue, stress, and sexual activity may develop the clinical picture as well (Fairbanks and Kaliner 1998).
11.3.1.4 Others Causes of Rhinitis
Many other clinical pictures classified as nonallergic and noninfectious rhinitis are also common causes of sneezing. Occupational rhinitis is the most commonly observed one among these clinical pictures and is triggered by dense cigarette smoke, cold air, air fresheners, formaldehyde, and other chemical irritants in the workplace (Stevens 1991; Dykewicz et al. 1998). Hormonal rhinitis may occur in cases of physiologically increased levels of estrogen such as puberty, menstrual cycle, and pregnancy or in case of receiving exogenous estrogen while on oral contraceptives (King and Mabry 1993; Dykewicz et al. 1998). Inhibiting acetylcholinesterase activity, estrogen leads to edema formation in the nasal mucosa while progesterone causes congestion through vasodilatation in capacitance vessels and sneezing occurs (Incaudo 2004). As a result of sympathetic hypoactivity in hypothyroidism, parasympathetic activity relatively increases leading to vasodilatation in the nasal mucosa and an increase in secretions. Drug-induced rhinitis may be manifested in two clinical patterns. In medicamentous rhinitis many drugs affect nasal mucosa through different mechanisms of action and cause sneezing. It is usually observed in treatments with antihypertensive drugs (reserpine, guanethidine, phentolamine, methyldopa, hydralazine, and prazosin), beta blockers (propranolol, nadolol), aspirin, and other NSAIDs (Cingi et al. 2011). Rebound rhinitis, on the other hand, develops as a result of prolonged usage of vasoconstrictor drops or sprays (King and Mabry 1993; Dykewicz et al. 1998; Fairbanks and Kaliner 1998). In geriatric rhinitis, atrophy in submucosal glands due to senility and severe irritation in sensitive nerve endings result in nasal stuffiness and sticky and thick mucus which may cause sneezing. Atrophic rhinitis is a rare pathological condition in etiology of which bacterial infections, deficiency of vitamin A or D, and iron or estrogen deficiencies are suspected. In contrast to clinical conditions concerned, many different factors may develop irritant-induced rhinitis and cause sneezing (Fairbanks and Kaliner 1998). Some of these include dust, smoke, perfume, powder, sharp odor, ammonia, inhalation of corrosive gases or chemicals, mechanical obstruction of the nasal cavity, chymic irritation due to cauterization or silver nitrate application, capsaicin, application of airflow into superior nasal meatus by a catheter, and repetitive nasal electrical stimulation (Imamura and Kambara 1992; Kitajiri et al. 1993; Kira et al. 1997). Capsaicin, the active ingredient obtained from hot chili peppers, stimulates the nasal small unmyelinated C-fiber afferent nerves to release various tachykinins. These nerves, with their somata in the trigeminal ganglion, transmit the information to the central nervous system through the trigeminal dorsal horn in the medulla and lead to sneezing and a sense of pain (Geppetti et al. 1988). Although various peptides and tachykinins may be involved, it appears that the capsaicin-induced release of substance P is the most potent trigger of the sneezing response (Kitajiri et al. 1993; Imamura and Kambara 1992). Capsaicin also precipitates sneezing through a local axon reflex (Canning 2002).
11.3.2 Photic Sneeze Reflex
It seems that some people really do sneeze when they look at the sun or actually at any bright light (there is nothing special about the sun). Photic sneeze reflex is also called ACHOO (autosomal dominant compelling helio-ophthalmic outburst) syndrome (Collie et al. 1978). This reflex was first described in the medical literature by Sedan in 1954 (Sedan 1954). It was shown to have an autosomal dominant inheritance pattern and is assumed to affect 17–35 % of the world population (Morris 1987). Photic sneeze reflex has been reported to be present in 23 % of medical students (Everett 1964). According to a Swedish study, 24 % of blood donors experienced sneezing on visual exposure to strong light (Beckman and Nordenson 1983).
We do not know exactly why this happens, but it might reflect a “crossing” of pathways in the brain, between pupillary light reflex arc and sneezing reflex arc. The reflex can be triggered only after the first exposure to light, never on repetitive stimulation, and many reports cite a refractory period before the reflex can be elicited suggesting that a polysynaptic pathway is involved. The first theory concerning the pathways mentioned belongs to Eckhardt et al. who suggested that stimulation of the optic nerve triggers the trigeminal nerve (Eckhardt et al. 1943). The afferent impulses of pupillary light reflex are transmitted via the optic nerve while the efferent impulses are transmitted via the oculomotor nerve. According to this theory, an indirect impulse is transmitted to the ophthalmic division of the trigeminal nerve. This impulse generates the nasal stimulation that causes sneezing by affecting the maxillary division of the trigeminal nerve as well. The second theory of crossing pathways belongs to Watson. Light falling on the retina stimulates afferent fibers to the pretectal nuclei, which then send interneurons to the Edinger-Westphal nuclei. The parasympathetic fibers from the Edinger-Westphal nuclei and the trigeminal afferent fibers from the cornea both pass through the ciliary ganglion, where they may participate in transmission (Watson 1875). Parasympathetic generalization may also contribute to photic sneeze. Stimuli which excite primarily one branch of the parasympathetic nervous system tend to activate other branches. Thus, the parasympathetic branches of the oculomotor nerve which are activated to generate pupillary constriction against the bright light cause secretion and congestion in the nasal mucosa by triggering the parasympathetic activation by the pterygopalatine ganglion. This process triggers sneezing (Brubaker 1919).
What is the benefit of photic sneeze reflex? Photic sneezing reflex exists in animals for which the smell sensation is vital to survive and can be used to clean the nasal cavity. Animals such as cats and dogs sneeze largely through their nose while the adults sneeze through their mouth. The reflex arc may also be useful to a limited extent in human beings when it is considered that the nasal respiration is dominant in the neonatal period. Babies have no other way to get rid of the annoying little tickle caused by normal mucus. Young children sometimes have more disgusting ways of dealing with that sensation, but babies just sneeze often with the help of photic sneeze reflex.
In conclusion, photic sneeze reflex, which can lead the drivers to have accidents following a sudden exposure to sunlight at the end of a long tunnel, or can cause a plane crash by inactivating the masks of jet pilots, can be considered to be an annoying “holdover” of evolution (Benbow 1991; Breitenbach et al. 1993).
11.3.3 Physical Stimulants of the Trigeminal Nerve
Physical or mechanical stimulants in the innervation zone of the trigeminal nerve may trigger sneezing reflex. Some of these stimulants include pulling hair, tearing off eyebrows, or orbital injections administered frequently during ocular surgery under local anesthesia (Wallois et al. 1997; Sekizawa et al. 1998).
11.3.4 Central Nervous System Pathologies
The lateral medullary syndrome (LMS), or Wallenberg’s syndrome, often results from occlusion or dissection of the vertebral artery. Vertebral artery dissection has been blamed on many different life events, such as sneezing (Schievink 2001). Paroxysmal sneezing at the onset of LMS is usually interpreted as a cause, since a violent sneeze could potentially result in a vertebral artery dissection causing LMS. Due to inactivation of sneezing center in LMS, sneezing cannot occur although the sensation of sneezing is present (Martin et al. 1991; Hersch 2000; Bernat and Suranyi 2000). Localization of the human sneeze center was described in a patient with right LMS, initially presenting with violent sneezes and followed by brief loss of the sneeze reflex with eventual recovery (Seijo-Martinez et al. 2006).
Sneezing may commonly accompany temporal lobe and grand mal epilepsy. It may be observed during the aura prior to an epileptic seizure or it may develop as an autonomic reflexive response during the seizure as well (Penfield and Kristiansen 1951; Penfield and Jasper 1954). Beverwyck commented upon the analogy of the epileptic seizure with hiccups and sneezing and noted that the physiological and anatomical basis for such a hypothesis remained to be unexplained (Temkin 1945). In the mid-nineteenth century, Jackson used the term epilepsy “as the name for occasional, sudden, excessive, rapid and local discharges of grey matter” (Jackson 1958). Jackson further commented upon the healthy and yet random discharge and concluded that “a sneeze is a sort of healthy epilepsy.”
11.3.5 Psychogenic (Intractable) Sneezing
Intractable sneezing, first described by Shilkrel in 1949, is a rare pathological condition that has been detected in more than 50 cases in literature up to present (Shilkrel 1949; Bhatia et al. 2004; Sulemanji et al. 2011). Kanner referred to a 13-year-old girl who had incessant sneezing for over 2 months and whose progress was followed by a daily newspaper communique (Kanner 1957). A diagnosis of hysteria was made and subsequent psychotherapy eliminated the sneezing. Yater referred to similar explosive repetitious episodes and considered them to be a sort of imitation of the true act of sneezing (Yater and Barton 1942).
Psychogenic intractable sneezing occurs mainly in adolescent girls for which a cause may not be found. Organic lesions or causes should always be carefully excluded (Sulemanji et al. 2011). Patients are usually refractory to various medications and have an otherwise unremarkable extensive workup (Bergman 1984; Lin et al. 2003). Inspiratory phase is quite short and the amount of nasal mucosal secretion expelled very low. Eyes may remain open during sneezing. It usually develops due to psychogenic factors and is refractory to medical treatment (Gopalan and Browning 2002). Approximately 25 % of the reported cases resolve without any form of treatment, except counseling of the patient and family (Sulemanji et al. 2011). Psychogenic sneezing responds well to psychological measures such as psychotherapy, biofeedback, relaxation exercises, supportive psychotherapy (i.e., explanation of nature of illness, suggestion to overcome symptoms), and behavior therapy (reward when there is symptom reduction, aversion therapy, hypnosis, and relaxation). The role of anxiolytic drugs lies in reducing underlying anxiety and making the patient more amenable to psychotherapy (Guner et al. 2010).
Medically unexplained physical symptoms usually carry diagnostic difficulties for the physicians (Sulemanji et al. 2011). The most important factors that increase these diagnostic difficulties are the possibility of an underlying physical illness and the uncertainty encountered as to how far the investigations for physical causes should go. It was determined that in some somatization patients, organic pathologies were revealed during follow-up. Paradoxically, it is known that repetitive and advanced investigations for any organic etiology in conversion disorder may increase the anxiety and doubts in the family and thus prolong the duration of the illness. In conclusion, one must not assume that every case of paroxysmal sneezing is of psychogenic origin. Due to the nature of such a disorder, these patients should undergo medical evaluations before a psychogenic cause is even considered.
11.3.6 Snatiation* Reflex
An uncontrollable sneezing attack developing as a result of stretching of the stomach following an excessive nutrition is first described by Teebi et al. as a reflex with autosomal dominant inheritance pattern (Teebi and Al-Saleh 1989). The mechanism of development is unknown. Snatiation* is a combination of the words “sneeze” and “satiation.” Snatiation also stands for “Sneezing Noncontrollably At a Tune of Indulgence of the Appetite-a Trait Inherited and Ordained to be Named” (Hall 1990). This abbreviation was supposed to facilitate the future cases to be evaluated in the same class. Recently, two patients have been reported, who state that several members of their family sneeze on a full stomach (Bhutta and Maxwell 2009). This report doubles the number of families with snatiation reflex in the medical literature.
11.3.7 Sexual Ideation or Orgasm
An association between sexual excitement and sneezing was first described in the nineteenth century (Watson 1875; Mackenzie 1884) followed by a young German otolaryngologist who developed a theory of “nasal reflex neurosis” due to the finding of erectile tissue in both nasal mucous membranes and genital areas (Young 2002; Jones 1974). The first report of this phenomenon in the literature describes a 69-year-old man who complains of severe sneezing immediately following orgasm, with no associated psychiatric morbidity (Anonymous 1972). Stromberg in 1975 and Korpas in 1979 described male orgasm as a precipitant for the sneeze reflex (Stromberg 1975; Korpas and Tomori 1979). Recently, Bhutta described a middle-aged man with uncontrollable fits of sneezing with sexual thought. The patient had no other rhinological symptoms and psychiatric morbidity (Bhutta and Maxwell 2008). Bhutta et al. performed a search of Internet “chat rooms” and found 17 people of both sexes reporting sneezing immediately upon sexual ideation and three people after orgasm. Although Internet reports do not give an accurate incidence, their findings do suggest that it is much more common than recognized.
11.4 Diagnosis, Differential Diagnosis, and Management of Rhinitis
The evaluation of a patient with sneezing should be individualized according to the duration and severity of the symptom. Laboratory tests are not necessary in the majority of patients, since the diagnosis is usually obvious from the history and physical examination.
It should be remembered that the history of the patient is the most important and determining stage for the diagnosis (Kramer 2006). The patient should be asked what his/her main complaint is; the duration and frequency of the symptoms like nasal discharge, stuffiness, and pruritus if present; whether the nasal discharge or stuffiness is present on one side or both, perennial or seasonal; whether he/she has allergic complaints, past trauma, past nasal surgery history, known diseases, and drugs used; and also how these symptoms effect the quality of life. In female patients it is also important to ask whether she is pregnant or on oral contraceptives (Incaudo 2004). One of the most common signs of allergic rhinitis in children is a horizontal creasing over the nasal tip. This physical examination sign develops as a result of habitual rubbing, which is also called allergic salute, after a duration of at least 2 years, a repeated action in order to relieve pruritus and improve respiration. This habit may turn into facial grimacing in adulthood for social reasons. Allergic shiner, on the other hand, is permanent pigmentation on the skin of lower eyelid which present as dark circles at the beginning stage. It develops due to subcutaneous hemosiderin through a capillary leak during periorbital venous stasis as a result of nasal mucosal congestion. Dennie-Morgan folds are short semilunar lines or folds found below the inferior eyelid. These lines develop due to venous blood retention cause by continuous spasm of Müller’s muscle under the inferior eyelid. Silky long eyelashes are another outstanding concomitant sign of allergy. Clinical examination including anterior rhinoscopy and nasal endoscopy provides large information about pathologies related to septum and lateral nasal wall. Allergy is prediagnosed with medical history and physical examination. If the patient has a medical history and complaints that are compatible with allergy, in vivo (prick test, SET, scratch test) and/or in vitro (serum-specific IgE) allergy tests should be performed (Settipane and Klein 1985). The skin prick test is the most common epidermal test. A positive allergen skin test that is compatible with the medical history and findings of physical examination should be assumed to be significant (Skoner 2001). RAST (radioallergosorbent test) and ELISA (enzyme-linked immunosorbent assay) tests measure the amount of allergen-specific IgE antibodies. Since there is no risk of systemic reactions during the application of these tests, they can safely be performed on pregnant women, on patients with a past history of systemic reaction, during measuring the sensitivity to antigens with a high risk of systemic reaction, on patients with skin diseases, on people who use drugs that may affect the prick skin test results, and in medicolegal cases where objective data are needed and also on children. The changes that develop due to gradually increasing doses of the allergen are followed by nasal provocation test. This test is performed when objective data are needed for occupational rhinitis, and it is rather used for scientific studies. Nasal cytology is not a diagnostic method performed for routine clinical practice and considered as an evaluation that does not provide a sufficient support alone (Scadding 2001). The use of acoustic rhinometry and rhinomanometry, which are the most common objective nasal airway tests, is confined because they have high costs and is time demanding in terms of application and interpretation (Galen 1997). Mucociliary function may be evaluated for differential diagnosis in patients with rhinitis (Shaari et al. 2006). Radiological examination is not necessary in a patient prediagnosed with rhinitis as long as an additional pathology is not suspected.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


