10

Photodynamic Therapy
Lucienne Collet  Gema Ramírez
Gema Ramírez  Rafael Cortez D. Virgil Alfaro III
Rafael Cortez D. Virgil Alfaro III  John B. Kerrison
John B. Kerrison  Monica Rodriguez-Fontal
Monica Rodriguez-Fontal
INTRODUCTION
Age-related macular degeneration (AMD) is the leading cause of legal blindness or severe vision loss in patients older than 60 years in developed countries (1). The management of AMD differs depending on whether it is exudative or nonexudative. The only proven treatment for the nonexudative type, comprising 85% of cases, is an antioxidant/mineral supplement which can slow the progression of the disease by 25% over 5 years (2). For the remaining 15% of the cases, laser treatment, thermal laser photocoagulation, submacular surgery, photodynamic therapy (PDT), and pharmacologic therapy are considered as treatment options.
In 1982, the Macular Photocoagulation Study (MPS) Group demonstrated the effectiveness of laser treatment for choroidal neovascularization (CNV), showing decreased risk of vision loss in these patients (3). Treatment failure occurred in at least 50% of cases resulting from the development of recurrent or CNV on the foveal edge of the laser scar (4). In 1995, the MPS reported that treatment of subfoveal CNV composed of both classic and occult neovascularization was not beneficial with respect to visual acuity and recurrent neovascularization (5).
PDT was first used in ophthalmology in 1994 (6). In 1996, several multicenter randomized clinical trials of PDT with verteporfin were initiated to evaluate its safety and efficacy in treating subfoveal CNV secondary to AMD. Today, the management of exudative AMD is constantly changing with new antiangiogenic therapies.
MECHANISM OF ACTION AND PHARMACOLOGY OF PHOTODYNAMIC THERAPY
PDT uses an intravenously injected photosensitizing drug that reaches the target tissue through the bloodstream. The photosensitizer is activated by low-intensity laser light and causes damage to choroidal neovascular tissue through a photochemical reaction. The maximum absorption spectrum of the photosensitizer determines the wavelength of the radiation. The light-dye interaction elevates the photosensitizer from its electronic ground state to a higher-level excited triplet state. The photosensitizer quickly returns to the ground state and transfers energy to other molecules, such as oxygen. Singlet oxygen and free radicals are formed and react with proteins, nucleic acids, and lipid membranes. The effective penetration depth of PDT is dependent upon the wavelength of the light. At 630 nm the effective penetration depth is 2 to 3 mm and increases to 5 to 7 mm at 700 to 800 nm (7).
The reactions that follow the formation of intravascular free radicals are classified as cellular, vascular, and immunologic (8). At the cellular level, the free radicals develop a cytotoxic effect by interacting with mitochondria, lysosomes, and other intracellular organelles (9), leading to apoptosis. At the vascular level, which is believed to be the main mechanism, the free radicals lead to destruction of the vascular endothelium. When the vascular endothelium is destroyed, the basal membrane is exposed and it interacts with blood and its components, triggering a platelet aggregation (9). After platelet activation, diverse mediators of inflammation such as thromboxane and histamine are released, thus leading to thrombosis of the vascular lumen and a closing of the vessels limited to the CNV with slight effect on the surrounding microcirculation (10–12). The effectiveness and selectivity of PDT depends on the photosensitizer and the laser used. The ideal wavelength must coincide with the peak light absorption of the photosensitizer used (13). The photosensitizer diffuses into the bloodstream and adheres to the plasmatic low-density lipoproteins. These lipoproteins have abundant receptors in the cytoplasmic membranes of tumoral cells and vascular endothelium. After the photosensitizer associates with LDL, this complex is incorporated into the cell by endocytosis, and then it can be activated by a laser with the appropriate wavelength (14).
VERTEPORFIN
Verteporfin (Visudyne) is a tetrapyrrole derived from the benzoporphyrin, also called benzoporphyrin derivative monoacid ring A (BPD-MA). It is a potent second-generation light-activated drug. It is a chlorin-type molecule and exists as an equal mixture of two regioisomers, each of which consists of an enantiomeric pair that demonstrate similar pharmacologic activity in vitro and in vivo (15, 16). Verteporfin has a molecular formula of C41H42N4O8 and a relative molecular weight of 718.81. Nowadays, it is the only photosensitizer approved by the U.S. Food and Drug Administration (FDA) for the treatment of CNV secondary to AMD and subfoveal CNV secondary to pathologic myopia.
Verteporfin has a long absorption wavelength with a strong absorption peak at 680 to 695 nm (15). It absorbs light efficiently at a wavelength of 689 nm (red light), which can penetrate a thin layer of blood, melanin, or fibrotic tissue. Light at this wavelength is not absorbed strongly by naturally present substances (17). The strongest absorption peak of verteporfin is at approximately 400 nm (blue light), but this wavelength is not clinically useful for treatment of CNV because it is the same as the absorption peak of oxyhemoglobin (17). The most suitable light source for use in Visudyne therapy is a nonthermal diode laser, operating at a wavelength of 689 ± 3 nm (17).
The regimen of Visudyne therapy established by the phase I/II studies and investigated in phase III placebo-controlled studies is as follows:
Visudyne dose: 6 mg/m2 body surface area (BSA)
Infusion rate: 3 mL/min
Duration of infusion: 10 min
Light application interval after start of Visudyne infusion: 15 min
Wavelength: 689 nm
Dose: 50 J/cm2
Intensity: 600 mW/cm2
Resulting duration of light application: 83 seconds
Closure of abnormal, leaking blood vessels occurs for approximately 6 to 12 weeks in most patients. Reperfusion is common and multiple treatments are often required.
INFLUENCE OF TREATMENT PARAMETERS ON SELECTIVITY OF VERTEPORFIN
Studies have been conducted to test the effect of changing dosimetry in order to avoid damage to the surrounding tissue (18). It has been observed that there is a significant photodynamic effect on the choroidal circulation with 50 J/cm2. This parameter was established as a guideline under treatment of age-related macular degeneration with photodynamic therapy (TAP) (19–23). It has been demonstrated by indocyanine green (ICG) angiography that the TAP regimen regularly results in damage to the physiologic choroid, showing early and often persistent nonperfusion of the surrounding choroid (19, 20). Histopathologic studies show a dose-dependent thrombosis of the choriocapillaris (21) and immunostaining reveals a reactive upregulation of vascular endothelial growth factor (VEGF) (22). Modification of treatment parameters with reduced fluence to 25 J/cm2 allows selective closure of the CNV and reduces the impact on the physiologic choroidal vasculature (18).
CLINICOPATHOLOGICAL FINDINGS AFTER PHOTODYNAMIC THERAPY
Histopathological findings of CNV 2 weeks to 3 months after PDT in neovascular AMD have been published (24–26). In these studies, endothelial damage of the CNV was noted. Schnurrbusch, in an electron microscopic study of surgically extracted CNV, showed occluded vessels with thrombotic masses and ultrastructural damage of the neovascular endothelium 3 months after PDT (24). Ghazi also reported endothelial cell degeneration with platelet aggregation and thrombus formation on removed CNV specimens 4 weeks after PDT (25). In a more recent study, the histopathological examination of the excised CNV membranes was done 3 days after PDT (24). It revealed fibrovascular tissue with swollen and disintegrated endothelium. However, neither a red blood cell nor a platelet/fibrin clot was observed (24). Other studies have also reported a uniform occlusion of the healthy choriocapillaris 1 week following PDT in enucleated human eyes (27). The occlusion of the choriocapillaris, perhaps, is the explanation for the nonperfusion of CNV membranes in 3 days following verteporfin PDT.
Whether PDT-induced ischemia of the choriocapillaris influences the reactivation of the CNV by increasing the expression of factors contributing to new vessel formation is not known. The absence of thrombosis in the CNV by light microscopic examination, in the presence of fluorescein angiographically proven nonperfusion of the entire treated area, suggests that choroidal ischemia induces the closure of the CNV vessels in the early period following PDT. The disintegration of the endothelium of the CNV vessels may result in thrombosis in the weeks following treatment (28). Additionally, Tatar et al. studied 50 eyes that underwent removal of choroidal neovascular membranes, 20 of them having received PDT prior to removal. The study histologically revealed many collapsed vessels, damaged endothelial cells, and an occluded choriocapillary layer within the spot produced by the laser. There was intense VEGF synthesis especially prominent in retinal pigment epithelium (RPE) cells induced by hypoxia after PDT (29–33). There was prominent inflammatory activity described in post PDT CNV (34). These findings seem to be an important angiogenic stimulus that may lead to increased vascular leakage and development of recurrent CNV (35).
IMMUNOHISTOLOGICAL EVALUATION OF CHOROIDAL NEOVASCULARIZATION POST PHOTODYNAMIC THERAPY
Analysis of vascularization and proliferative activity of surgically extracted CNV following PDT by immunodetection of characteristic markers (CD 34, CD 105, and Ki-67) showed that there is a neoangiogenetic mechanism that leads to the formation of new vessels observed in CNV even after 37 days post PDT (36). However, Schnurrbusch (24) and Moshfeghi (37) reported that new vessel formation does not occur until a minimum of 63 days after such an event.
ANGIOGRAPHIC FINDINGS AFTER PHOTODYNAMIC THERAPY
Fluorescein angiography in animal studies, early after PDT, demonstrated hypofluorescence with perfusion of retinal vessels. Also, ICG angiography demonstrated hypofluorescence in the area treated with PDT, although larger choroidal vessels were perfused. In animal studies, this hypofluorescence on ICG angiography resolved to some extent with follow-up but was still evident at 5 to 8 weeks after PDT. The hypofluorescence may be caused by PDT-induced choriocapillaris occlusion or retinal pigment swelling leading to blocked fluorescence. Follow-up at 2 to 5 weeks after PDT demonstrated staining of the irradiated CNV by ICG angiography and may represent staining of the remaining fibrovascular tissue (29).
OCT AFTER PHOTODYNAMIC THERAPY
Rogers et al. (38) studied the optical coherence tomography (OCT) characteristics following PDT in eyes treated for CNV secondary to AMD. They correlated it to fluorescein angiography findings and proposed an OCT classification system as follows:
In Stage I there is evidence of acute inflammatory response, confirmed at 1 hour and up to 1 week following PDT. Fluorescein angiography revealed hyperfluorescence of both the CNV and treatment area, with later frames of the angiogram demonstrating increased leakage of fluorescein in the treatment zone. The OCT demonstrated increased accumulation of intraretinal fluid in a circular distribution delineating the treatment spot.
In Stage II there is resolution of subretinal fluid with choroidal hypoperfusion. Approximately 1 to 2 weeks following treatment, there is hypoperfusion of the CNV and choriocapillaris with a well-delineated area of hypofluorescence corresponding to the treatment spot on fluorescein angiography (FA). OCT exhibits resolution of subretinal fluid in the treatment area with the reestablishment of a normal appearing foveal contour. Stage II typically lasts up to 4 weeks or whenever choroidal reperfusion occurs.
In Stage III, there is reaccumulation of subretinal fluid with subretinal fibrosis. They observed that after the fourth week of treatment, reperfusion of the CNV is typically present on FA with variable degrees of leakage. The treatment spot is less visible on angiography, as the choriocapillaris is rapidly perfused. Intraretinal and subretinal fluid reaccumulates and early subretinal fibrosis becomes evident on OCT between the retina and underlying RPE. They propose that Stage III is subdivided into two separate stages: stage IIIa and IIIb, depending on the ratio of fluid to fibrosis on OCT. In stage IIIa retinal fluid to fibrosis ratio is higher, representing a more active neovascular process. In stage IIIb, the fibrotic component of the CNV is prominent with minimal intraretinal fluid on OCT. Stage IIIb lesions are relatively inactive due to the predominance of subretinal fibrosis with minimal intraretinal fluid, which still leak on fluorescein angiography.
In Stage IV, there is subretinal fibrosis with cystoid macular edema (CME). On FA, the borders of the lesion remain relatively fixed with staining of the fibrotic CNV. However, a component of active leakage in FA is present, which is defined on OCT as CME. The cysts are represented by hyporeflective black circular spaces in the retina. The involuting CNV is represented on the OCT as a highly reflective band merging with RPE/choriocapillaris layer (38).
ELECTRO-OCULOGRAPHY AFTER PHOTODYNAMIC THERAPY
Osner et al. found that the Arden ratio of the electro-oculogram (EOG) decreased 1 week after PDT and the differences were statistically significant. The decrease in Arden ratio persisted at the first month, as assessed by EOG recordings. PDT may affect the interaction between RPE and photoreceptors (39).
CLINICAL TRIALS
There are numerous controlled studies that employ PDT. They can be divided into Phase I/II dose-finding studies, where the dose parameters are established, and Phase III placebo-controlled studies that include TAP, verteporfin in photodynamic therapy (VIP), and verteporfin in the ocular histoplasmosis (VOH).
In order to determine an effective treatment regimen as well as the safety and efficacy of Visudyne therapy, a total of 1236 patients were included: 142 in the phase I/II dose-finding study, 609 in the TAP investigation, 459 in the VIP trial, and 26 in the VOH syndrome study.
DOSE-FINDING STUDY (PHASE I/II)
Dose Determination
Some experiments with thermal laser-induced neovascularization in primate eyes were conducted in order to determine the optimal parameters for effective closure of CNV with Visudyne therapy (14, 23, 30, 40–57). Maximal closure of CNV was achieved using Visudyne 0.375 mg/kg with light application 20 to 50 minutes after Visudyne injection at a light dose of 150 J/cm2 (light intensity 600 mW/cm2) (56). Lower doses of Visudyne were more selective for CNV, reduced damage to surrounding tissues, and permitted a shorter time interval between Visudyne infusion and light application (56). Light intensities of 300 or 600 mW/cm2 enabled shorter, more practical treatment times and were not accompanied by any apparent adverse effects (57). Light doses of 50 to 600 J/cm2 stopped fluorescein leakage from CNV, but doses of ≥400 J/cm2 were associated with unacceptable toxicity in normal retinal tissues (52). These parameters formed the basis for phase I/II dose-finding studies in patients with CNV.
Phase I/II dose-finding study was carried out in patients with subfoveal CNV (30–32). It was a nonrandomized, dose-finding study that was conducted at a total of four centers in Europe and North America. It included 142 patients with subfoveal CNV secondary to AMD (n ∇ 128), pathologic myopia (n ∇ 10), ocular histoplasmosis syndrome (OHS) (n ∇ 1), angioid streaks (n ∇ 1), and idiopathic causes (n ∇ 1). All of them had evidence of classic CNV and were not eligible for laser photocoagulation.
All patients received one of five treatment regimens and were monitored for 12 weeks. Within each regimen, light at 689 nm (intensity 600 mW/cm2) was increased up to a maximum of 150 J/cm2; each light dose was tested on three patients, and the dose was only increased if these patients did not experience adverse events. The maximum tolerated light dose was below 150 J/cm2 and the minimum effective light dose was greater than 25 J/cm2 (30). At 150 J/cm2, nonselective effects on the retinal vasculature and loss of visual acuity were observed, and little evidence of effect on neovascular tissue was seen at light doses of 25 J/cm2 (30).
PLACEBO-CONTROLLED STUDIES (PHASE III)
In order to study the efficacy of Visudyne therapy in terms of visual function and angiographic outcomes, in patients with CNV, the following phase III clinical trials in patients with CNV were conducted:
– Treatment of AMD with Photodynamic therapy (TAP) Investigation (23, 40)
– Verteporfin in Photodynamic therapy (VIP) Trial (41, 42)
TREATMENT OF AGE-RELATED MACULAR DEGENERATION WITH PHOTODYNAMIC THERAPY INVESTIGATION (PHASE III)
The TAP Investigation (23, 40) included two clinical trials, designed to determine if PDT with Visudyne significantly reduced the risk of vision loss compared with placebo in patients with subfoveal CNV secondary to AMD. It was a 2-year study that was conducted in 22 centers in North America and Europe, and the enrollment was completed in 1997. Patients were randomized in a ratio of 2:1 to receive either Visudyne (n ∇ 402) or placebo (dextrose in water) (n ∇ 207) in a double-masked fashion.
The inclusion criteria were as follows: patients over 50 years of age with new or recurrent subfoveal CNV secondary to AMD; the lesion had to have classic CNV (although the presence of occult CNV was permitted) with evidence that either classic or occult CNV involved the geometric center of the foveal avascular zone; the combined area of classic CNV had to occupy at least 50% of the total CNV; the greatest linear dimension could not exceed the diameter of a circle measuring 9 MPS disc areas (approximately 5400 μm); and the treatment eye had to have a best-corrected visual acuity score of at least 34 and not more than 73 letters (Snellen equivalent: 20/200 – 20/40). The characteristics of the treatment groups were balanced, except that there were more women assigned to placebo than Visudyne (p ∇ 0.025) and more lesions with blood assigned to placebo (p ∇ 0.028). The follow-up examinations were scheduled every 3 months. The treating physician considered retreatment if there was leakage from CNV on the fluorescein angiogram. All randomized patients received treatment at the baseline visit, and the final treatment was given at month 21, with follow-up at month 24. From month 6 through month 21, re-treatments were required by 12% to 20% fewer patients treated with Visudyne than placebo (40). The mean number of treatments administered per patient through the 2 years of the TAP Investigation was 5.6 in the Visudyne group and 6.5 in the placebo group. In the second year, fewer treatments were required (mean 2.1) than in the first year (mean 3.4) in the group treated with Visudyne (40).
TAP Report 5 (42) is an open label extension of selected patients from TAP trial where patients were followed beyond 2 years. The purpose was to describe the visual outcomes between the month 24 and month 36 for verteporfin-treated patients who had a predominantly classic lesion at baseline. The results show little change from the two-year findings for patients with lesions that were composed of predominantly classic CNV and assigned to verteporfin therapy at baseline. The results provide evidence that the benefits of this therapy continued through 3 years in patients with subfoveal CNV caused by AMD (42).
VERTEPORFIN IN PHOTODYNAMIC THERAPY TRIAL (PHASE IIIB)
The VIP Trial (41) was designed to investigate the efficacy of PDT with Visudyne in a wider range of patients compared to the TAP trial. The study included patients with AMD with better visual acuity (70 letters or better, approximate Snellen equivalent better than 20/40), patients with occult CNV with no classic CNV, and patients with CNV secondary to pathologic myopia. It was a 2-year study involving 28 centers in North America and Europe. The enrollment was completed in 1998. Patients were stratified according to the cause of CNV and randomized in the ratio of 2:1 to either Visudyne (n ∇ 306) or placebo (n ∇ 153).
The inclusion criteria were as follows: patients with new or recurrent subfoveal CNV secondary to AMD or pathologic myopia; patients at least 50 years of age whose CNV was secondary to AMD; the area of classic CNV plus occult CNV had to occupy at least 50% of the total lesion; the greatest linear dimension of the lesion could not exceed the diameter of a circle measuring 9 MPS disc areas (approximately 5400 μm); and the treatment eye had to have a best-corrected visual acuity score of at least 50 letters (20/100 or better), except for eyes with lesions containing classic CNV secondary to AMD, which had to have a best-corrected visual acuity score or better than 70 letters (20/40 or better). Lesions with occult CNV and no classic CNV either had to contain blood or show progression of disease within the 3 months preceding randomization to treatment (defined as either a loss of at least six letters of visual acuity or growth of at least 10% of the lesion’s greatest linear dimension within 3 months). If the subfoveal CNV was secondary to pathologic myopia, the spherical equivalent had to be equal to or more negative than –6 diopters, or the axial length had to be at least 26.5 mm. Only 22% of eyes had classic CNV at the baseline examination; 68% had occult CNV with no evidence of classic CNV (41). The majority of lesions were predominantly classic (83%), and only 14% of eyes had evidence of occult CNV at the baseline examination (43). In patients with AMD, the mean treatment rate was 3.1 in the Visudyne group and 3.6 in the placebo group (43). In patients with pathologic myopia, the mean treatment rate was 3.4 in the Visudyne group and 3.2 in the placebo group.
OTHER STUDIES
Japanese Age-Related Macular Degeneration Trial Study Group
Japanese Age-Related Macular Degeneration Trial (JAT) reported 1-year results of PDT with verteporfin in Japanese patients with subfoveal CNV secondary to AMD (44). After 1 year of follow-up, 50% and 77% of verteporfin-treated patients demonstrated no leakage from classic or occult CNV, respectively.
VOH STUDY (PHASE I/II) (45, 46)
The VOH Study is an open-label, three-center, 1-year study of 26 patients with OHS (45). The patients included in this study had OHS with subfoveal CNV lesions no larger than 5400 μm in greatest linear dimension with classic or occult CNV extending under the geometric center of the foveal avascular zone and best-corrected visual acuity letter score of 73 to 34 (approximate Snellen equivalent 20/40 to 20/200). The patients received verteporfin (6 mg/m2) with the same regimen of Visudyne therapy used in the TAP and VIP Trial. At 3-month follow-up examinations, retreatment with the same regimen was given if angiography showed fluorescein leakage.
By month 12, patients had received an average of 2.9 treatments of a maximum of four possible treatments. The month 12 median improvement from baseline in visual acuity of the remaining 25 patients was seven letters, and median contrast sensitivity improved by two letters. At the month 12 examination, 14 (56%) patients gained seven or more letters of visual acuity from baseline, whereas four (16%) patients lost eight or more letters, of which two (8%) lost 15 or more letters. No serious systemic or ocular adverse events were reported. They concluded that the median visual acuity improved after verteporfin therapy for at least 1 year (45).
The VOH Study published 2-year results (46) of an open-label, 3-center, uncontrolled clinical study. At 24-month examination, which was completed in 84% of the participants, median improvement from baseline in visual acuity was six letters; median contrast sensitivity improved by 3.5 letters. Ten patients (45%) gained seven or more letters of visual acuity from baseline, whereas four patients (18%) lost eight or more letters. There was absence of fluorescein angiographic leakage from classic CNV in 17 of the 20 evaluable lesions (85%). They concluded that the median visual acuity improved and fluorescein angiographic leakage decreased after verteporfin therapy in OHS patients (46).
SAFETY OF PHOTODYNAMIC THERAPY WITH VERTEPORFIN
The systemic and ocular safety of Visudyne therapy has been evaluated in three studies in patients with CNV secondary to AMD, pathologic myopia, and OHS. A total of 1094 patients were included in the TAP, VIP Trial, and the VOH Study (23, 41, 45). Systemic adverse events and ocular adverse events affecting the treated eye were recorded during each study. Other evaluations included measurement of vital signs, physical examinations, electrocardiograms, and laboratory assessments of hematology, serum chemistry, and urinalysis. Visudyne therapy is considered well tolerated. In fact, the withdrawal rate due to adverse events is low (3.8%). Serious adverse events related to treatment occurred in 3.5% of patients treated with verteporfin and 1.4% of placebo patients. In fact, photosensitivity reactions occurred in fewer than 3% of Visudyne-treated patients; injection-site adverse events occurred more frequently with Visudyne therapy (11.2%) than placebo (4.4%). The only reports of infusion-related back pain (2.0%) were in AMD patients treated with Visudyne therapy. All the cases were transient and resolved by the end of the infusion.
SERIOUS ADVERSE EVENTS
In the first year of TAP (23), the incidence of injection-site events was 11.9% in Visudyne treated patients and 1.9% in those who received placebo. In the second year of TAP (40), it increased to 14.4% and 4.8%, respectively. The total incidence of treatment-related serious adverse events was 3.5% for Visudyne-treated patients compared with 1.4% for patients who received placebo. No treatment-related deaths occurred in any of the ocular studies. The total rate of withdrawal from the ocular studies due to adverse events was low: 3.8% for Visudyne-treated patients compared with 0.3% for patients who received placebo.
In the TAP trial, three Visudyne-treated patients were withdrawn because of serious verteporfin-related adverse events, such as gastrointestinal bleeding, right-sided body pain with shortness of breath, high blood pressure, and suprachoroidal hemorrhage. An additional three patients were withdrawn due to nonserious treatment-related events, such as severe injection-site pain, skin rash, and infusion-related back pain. Additionally, in the AMD arm of the VIP trial, six verteporfin-treated patients were withdrawn because of adverse events, such as decrease in vision. Seven verteporfin patients (3.1%) had adverse events but were not withdrawn from the trial; their adverse events were central scotoma, vitreous hemorrhage, subretinal hemorrhage, vision loss in two cases, anemia, and knee infection. Four placebo patients had serious adverse events that were considered to be related to therapy (subretinal hemorrhage, vitreous hemorrhage, submacular hemorrhage, and hyponatremia).
In the myopia arm of the VIP trial, the treatment was discontinued in one Visudyne-treated patient who complained of dyspnea and flushing during the second minute of the first infusion. The infusion was discontinued and the dyspnea resolved within 15 minutes of treatment with intravenous (IV) steroids. Treatment was not discontinued in the VOH Study.
OCULAR ADVERSE EVENTS
Clinically significant ocular events were defined in the study protocols of TAP and VIP as serious adverse events including severe vision decrease, defined as vision decrease of at least four lines occurring within 7 days of treatment, arteriolar or venular nonperfusion, retinal capillary nonperfusion of at least 1 MPS disc area, or vitreous hemorrhage.
These ocular events occurred in a total of 24 (3.3%) verteporfin-treated patients and six (1.7%) patients who received placebo. They occurred in patients with AMD and in patients with minimally classic or no classic lesions at baseline (21 of 24 Visudyne patients and four of six placebo patients). There were no clinically significant ocular events in patients with pathologic myopia or OHS. In the three trials, 13 patients there were reported to have an acute severe decrease in vision (1.8%) treated with verteporfin. Four episodes of severe vision decrease were reported in three (0.7%) verteporfin-treated patients within 9 days of treatment in the TAP trial. Two of these patients improved their vision (>5 letters) at the next 3-month visit. Ten patients in the AMD arm of the VIP Trial experienced a severe decrease in vision. No clinically significant ocular adverse events occurred in either treatment group in patients with pathologic myopia.
PHOTOSENSITIVITY REACTIONS
In the TAP trial of 2 years (23) and VIP 1-year trial (43), the photosensitivity reactions reported were 2.2%, seen in patients treated with Visudyne therapy. The photosensitivity reactions were transient and mild to moderate secondary to direct exposure to sunlight within 3 days of treatment and resolved within 1 week. Such reactions can be prevented, and patients should take precautions such as avoiding exposure to direct sunlight or bright indoor lighting, wearing dark sunglasses outdoors during the first 48 hours, and avoiding exposure to powerful operating lights.
ABSORPTION AND BIODISTRIBUTION OF VERTEPORFIN
The pharmacokinetics of verteporfin have been studied in animal models. The apparent volume of distribution at steady state (VSS) in mice, rats, and dogs ranged from 0.26 to 0.94 L/kg depending on the dose and animal studied (47). Dose-dependent variables, such as area under the plasma concentration–time curve and maximum measured plasma concentration (Cmax) demonstrated dose proportionality and were similar under single and multiple dosing, suggesting that there was no accumulation of verteporfin with multiple dosing (47). Verteporfin rapidly distributes in the liver, spleen, and kidneys. Maximal concentrations were observed in all tissues within 3 hours of administration but decreased within 24 hours. Verteporfin reached higher levels in tumors than in normal tissues other than liver, spleen, and kidney, and elimination from tumor tissue was slower than from other tissues, resulting in a higher tumor-to-tissue concentration ratio 24 hours after administration.
Biodistribution studies show that verteporfin accumulates within 5 minutes in vascular structures in the eye, such as the choroid and ciliary body (48). Verteporfin accumulates less in avascular structures such as the cornea, lens, and vitreous. However, it accumulates within 5 minutes in RPE cells. Two hours after administration, it is no longer detectable in the choroid or photoreceptors and reduced in the RPE. Verteporfin is selectively taken up and retained more by malignant, rapidly dividing cells than by normal or resting cells (49). Verteporfin selectively accumulates in neovasculature such as the proliferating vasculature within tumors (50). Also, in vivo studies have indicated that verteporfin is taken up rapidly and selectively by ocular neovascular endothelial cells (14). After verteporfin is administered intravenously it associates almost exclusively with plasma lipoproteins (47).
Studies of human plasma have shown that 6% of verteporfin is associated with albumin, and 91% is distributed equally among the high-density, low-density, and very low-density lipoprotein fractions (51); thus, it makes verteporfin available to rapidly dividing endothelial cells of the neovasculature through LDL receptor-mediated pathway and possibly via direct diffusion (47). This enhanced delivery is due to high levels of expression of LDL receptors on endothelial cells of the neovasculature.
METABOLISM AND ELIMINATION
Verteporfin is metabolized primarily in the liver, and in the plasma, by esterases (52). The main metabolite is a less active diacid form of verteporfin, but this accounts for only 5% to 10% of the total exposure and is also rapidly eliminated. This biotransformation of verteporfin to a nonphotosensitive product could account for the rapid disappearance of photosensitivity in tissues such as the skin (53). Verteporfin is eliminated rapidly from plasma and exhibits multicomponent kinetics consisting of an initial rapid phase during the first 30 minutes after administration, a second slightly slower elimination rate lasting 8 hours, and a third more prolonged phase (52). Elimination is through the biliary route and less than 0.01% is recovered in urine. The mean plasma half-life of verteporfin is 2 to 5 hours after intravenous doses of 0.5 to 2.0 mg/kg (52).
CLINICAL PHARMACOKINETICS
After a 10-minute infusion of Visudyne 6 mg/m2 BSA the following variables were determined (54):
 Maximum plasma concentration (Cmax) of 1.1 to 1.3 μg/mL
Maximum plasma concentration (Cmax) of 1.1 to 1.3 μg/mL
 Area under the plasma concentration–time curve (AUC0-t) of 1.5 to 1.7 μg∙h/mL
Area under the plasma concentration–time curve (AUC0-t) of 1.5 to 1.7 μg∙h/mL
 Apparent volume of distribution (vss) of 0.45 to 0.6 L/kg
Apparent volume of distribution (vss) of 0.45 to 0.6 L/kg
 Plasma elimination half-life (t1/2) of 5 to 6 h
Plasma elimination half-life (t1/2) of 5 to 6 h
 Total body clearance (CL) of 90 to 110 mL/h/kg
Total body clearance (CL) of 90 to 110 mL/h/kg
Less than 0.01% of the dose is excreted in the urine (54). Dose alterations are therefore unnecessary in patients with renal impairment. The pharmacokinetics of verteporfin are altered in patients with mild hepatic dysfunction (54). The effect is a reduction in plasma clearance, which is predictable because biliary clearance is the main route of verteporfin elimination, and this decreased clearance is not associated with increased skin photosensitivity. Dosage adjustments are therefore not necessary in patients with mild hepatic impairment (Fig. 10-1).
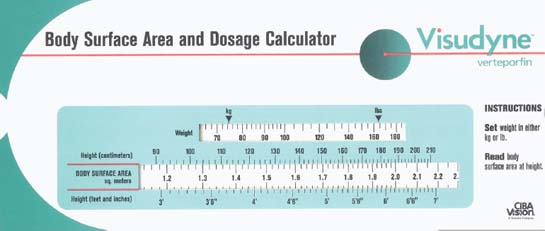
Figure 10-1. Dose meter for Visudyne (vertporfin).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


