8 See Chapter 3. Before surgery, the surgeon should question the patient about the following: 1. Use of oral medications that are α-1 blockers (e.g., Flomax [tamsulosin]; Cardura [doxazosin]; Hytrin [terazosin]; Uroxatral [alfuzosin]; Minipress [prazosin; Clopixol [zuclopenthixol]) increase the risk of intraoperative floppy iris syndrome (IFIS) (intraoperative miosis, floppy iris, and iris prolapse through wound). 2. Assess dose, duration, and interval since last dose. If patient has used these medications, plan accordingly (see 3d). 3. If patient has an automatic implantable cardiac defibrillator (AICD) or pacemaker, the operating room staff will likely require device information. In general, the AICD should be deactivated as it can inappropriately discharge during surgery. Discussion with patient’s cardiologist or anesthesiologist about the generation of AICD (first, second, third, fourth) and the need for deactivation with a “donut” magnet. 4. Note if patient is taking coumadin, aspirin, or plavix (clopidogrel bisulfate [Bristol-Myers Squibb/Sanofi Pharmaceuticals, Inc.]). Patients usually do not have to stop these medications. Most studies show no increased risk of retrobulbar hemorrhage with peribulbar injections. Topical anesthesia is an option if there is a concern; this essentially rules out hemorrhage. 5. On slit lamp examination, carefully assess for the following: size of maximally dilated pupil; pseudoexfoliation; phacodonesis; narrow angle (gonioscopy is recommended); guttae (Fuchs dystrophy), lens subluxation, zonular dialysis. 6. Check eye dominance if planning refractive cataract surgery. Choice of power depends on intraocular lens (IOL) type (i.e., monofocal versus refractive IOL). Some surgeons consider targeting the nondominant eye for reading vision when using monofocal lenses. 1. Calculate IOL power: Numerous formulas for calculating IOL power have been derived based on theoretical optics and empirical data. Check the literature for continued advances in IOL calculations (e.g., IOL master, Holladay II formula). The Sanders-Retzlaff-Kraff (SRK) formula is one of the most basic and widely used. SRK Formula: Power of IOL = A − 2.5(AL) − 0.9(K), where: K = average keratometry measurement in diopters. AL = axial length of eye in millimeters measured with A-scan ultrasonography. Certain formulas are generally recommended for certain axial lengths and IOLs: a. For short eyes, AL ≤ 22.0 mm, the Hoffer Q or Holladay II formula is recommended. b. For average eyes, AL 22.1–24.4 mm, Hoffer Q, Holladay I or II is recommended. c. For medium to long eyes, AL 24.5 to 25.9 mm AL, the Holladay I or II is recommended. d. For long eyes, AL ≥ 26.0 mm, SRK/T or Holladay II is recommended. e. If using the Crystalens Five-0, the Holladay II is recommended for AL < 22.0; the SRK/T is recommended for AL > 22.0. The Holladay II is recommended for comparison in steep corneas (Table 8.1). 2. Determine target postoperative refraction and select proper IOL. Target postoperative refraction may be in part determined by the status of the other eye (e.g., phakic, pseudophakic) and the type of IOL chosen (e.g., refractive lenses). Nomograms for many refractive lenses are available from the IOL manufacturer. 3. Dilate pupil and preoperative drops: a. Tropicamide 1%, phenylephrine 2.5%, and Cyclogyl 1%, every 15 minutes starting 1 hour before surgery is a typical regimen. Other regimen examples: Phen/Trop 1 gtt q 5 minutes × 3. Coll 3&38 ¼ 1 gtt q 5 minutes × 3. b. Preoperative drop of antibiotic (e.g., moxifloxacin 0.5% [Vigamox, Alcon, Inc., Fort Worth, TX, US], gatifloxacin 0.3% [Zymar, Allergan, Inc., Irvine, CA, US]) 1 drop before surgery. c. Optional: Topical nonsteroidal anti-inflammatory agent one drop every 15 minutes × 3 starting 1 hour before surgery (to minimize intraoperative miosis) (e.g., flurbiprofen 0.03% 1 gtt q 5 minutes × 2). Other topical nonsteroidal anti-inflammatory drugs (NSAIDs) (e.g., nepafenac 0.1% [Nevanac, Alcon, Inc.] 3e times per day, ketorolac tromethamine [Acular, Allergan, Inc.] 4 times daily, or bromfenac ophthalmic solution 0.009% [Xibrom, ISTA, Inc., Alpharetta, GA, US] 2 times per day), can be used for 5–7 days before surgery in patients with a history of diabetes, uveitis, previous cystoid macular edema, epiretinal membrane, or vein occlusion, and then for approximately 3 months after surgery to help prevent cystoid macular edema. Some surgeons use preoperative and postoperative NSAIDs on all patients. Check literature for updated efficacy studies among topical NSAIDs and current practices as indicated. d. If pupil dilates poorly or the patient has a history of using α 1A adrenergic antagonists (e.g., tamsulosin hydrochloride [Flomax]), be prepared to use iris hooks (4–0 polypropylene hooks or 6–0 nylon) or alternative method for addressing small pupil for potential IFIS (e.g., Healon 5, intracameral preservative-free epinephrine, preservative-free phenylephrine), Silicone Pupillary Expansion Ring (Graether Pupil Expander [Eagle Vision, Memphis, TN]), Perfect Pupil Injectable (PPI; Milvella, Ltd, Sydney, Australia). Low-flow parameters and lowering the balanced salt solution (BSS) bottle also helps in patients with Flomax. In addition, preoperative atropine 1% drops bid for 4–10 days before surgery may be used, if patient can tolerate potential anticholinergic effects. A preoperative gonioscopy should be considered in potential cases for angle closure (i.e., from anticholinergic effects of atropine). 4. Optional for complicated cases: For stable uveitis patients with no inflammation for 3 months before surgery, use topical NSAID 4 times daily for 7 days before surgery, then 3 months after surgery to help prevent cystoid macular edema. In case of active uveitis, consider admitting patient the day before surgery for intravenous corticosteroid management. Many surgeons recommend the use of nonsilicone lenses (e.g., polymethal methacrylate [PMMA] or acrylic) for patients with uveitis to minimize postoperative inflammation and posterior capsular opacification. If there is a poor red reflex or concern about being able to make a continuous capsulorhexis, consider using a capsular dye to allow easier visualization of the anterior capsule (see Capsular Stains section later in this chapter). 5. Preoperative and intraoperative antibiotic use. Preoperative and intraoperative antibiotic use (diluted in BSS bottle) is controversial, and there are broad variations in their use. Check the literature for updated information.
Phacoemulsification/Posterior Chamber Intraocular Lens Implantation
Indications
 Small incision phacoemulsification is the standard technique for cataract surgery today.
Small incision phacoemulsification is the standard technique for cataract surgery today.
 Advantages of phacoemulsification over extracapsular cataract extraction:
Advantages of phacoemulsification over extracapsular cataract extraction:
 Smaller wound minimizes astigmatism and wound-related postoperative complications.
Smaller wound minimizes astigmatism and wound-related postoperative complications.
 Surgery accomplished within a relatively closed system, allows for greater control over intraocular structures during surgery.
Surgery accomplished within a relatively closed system, allows for greater control over intraocular structures during surgery.
 May be done under topical anesthesia.
May be done under topical anesthesia.
 Less postoperative discomfort and inflammation.
Less postoperative discomfort and inflammation.
 Shorter recovery period.
Shorter recovery period.
 Innovations in the methods of phacoemulsification continue (e.g., ultrasound, torsional, laser). Review literature for latest outcomes reports.
Innovations in the methods of phacoemulsification continue (e.g., ultrasound, torsional, laser). Review literature for latest outcomes reports.
 Phacoemulsification generates heat by transforming electrical energy to mechanical energy with the subsequent generation of emulsifying shock waves.
Phacoemulsification generates heat by transforming electrical energy to mechanical energy with the subsequent generation of emulsifying shock waves.
Preoperative Procedure
Preoperative Surgical Considerations
| Length | Recommended Formulas |
|---|---|
| Short eyes (≤ 22.0 mm) | Hoffer Q or Holladay II |
| Average eyes (22.1–24.4 mm) | Hoffer Q or Holladay I or II |
| Medium-long eyes (24.5–25.9 mm) | Holladay I or II |
| Long eyes (≥ 26.0 mm) | SRK/T or Holladay II |
Instrumentation
 Honan balloon (optional)
Honan balloon (optional)
 Lid (phaco) speculum
Lid (phaco) speculum
 Castroviejo calipers
Castroviejo calipers
 Fine-toothed forceps (e.g., 0. 12 mm straight Castroviejo and/or Colibri)
Fine-toothed forceps (e.g., 0. 12 mm straight Castroviejo and/or Colibri)
 Westcott scissors
Westcott scissors
 Cellulose sponges
Cellulose sponges
 Cautery (underwater eraser or disposable)
Cautery (underwater eraser or disposable)
 Scleral incision blade (e.g., Beaver #64, #69)
Scleral incision blade (e.g., Beaver #64, #69)
 Crescent/tunnel incision blade (e.g., Beaver #38, #48)
Crescent/tunnel incision blade (e.g., Beaver #38, #48)
 Microsurgical knife (e.g., Beaver #75, MVR, MicroSharp, Superblade)
Microsurgical knife (e.g., Beaver #75, MVR, MicroSharp, Superblade)
 Viscoelastic substance (e.g., Healon, Amvisc, Viscoat)
Viscoelastic substance (e.g., Healon, Amvisc, Viscoat)
 Fine-Thorton 13-mm fixation ring
Fine-Thorton 13-mm fixation ring
 Keratome (e.g., Beaver #55, diamond or steel, 2.7 mm to 3.2 mm)
Keratome (e.g., Beaver #55, diamond or steel, 2.7 mm to 3.2 mm)
 Cystotome
Cystotome
 Utrata forceps
Utrata forceps
 Cyclodialysis spatula or vitreous sweep
Cyclodialysis spatula or vitreous sweep
 Kuglen hook
Kuglen hook
 Iris hooks (e.g., Grieshaber)
Iris hooks (e.g., Grieshaber)
 Drysdale Nucleus Manipulator (to rotate lens)
Drysdale Nucleus Manipulator (to rotate lens)
 Pre-chopper
Pre-chopper
 Chopper
Chopper
 Straight and angled McPherson tying forceps
Straight and angled McPherson tying forceps
 Needle holder
Needle holder
 Phacoemulsification unit
Phacoemulsification unit
 Capsule polisher
Capsule polisher
 Implant blade (e.g., Beaver #47)
Implant blade (e.g., Beaver #47)
 IOL folder or injector system
IOL folder or injector system
 IOL forceps
IOL forceps
 Sinskey hook
Sinskey hook
 Vannas scissors
Vannas scissors
 Sutures: 10–0 nylon, 10–0 Vicryl, 8–0 Vicryl
Sutures: 10–0 nylon, 10–0 Vicryl, 8–0 Vicryl
 Acetylcholine solution (e.g., Miochol)
Acetylcholine solution (e.g., Miochol)
Operative Procedure
1. Anesthesia: Topical, peribulbar, or retrobulbar plus lid block, or general. (See Chapter 4.)
Topical: Apply one drop of 0.5% tetracaine 15 minutes before surgery and 1 drop before the start of surgery. Optional: 2% Xylocaine gel in inferior fornix 5 minutes before surgery.
2. Optional: Apply Honan balloon for ~10–15 minutes to decompress eye and orbit, minimizing positive vitreous pressure.
Note: Honan balloons are not used for topical anesthetic cases.
3. Prep and drape. Use Steri-Strips or a brow tape cut in half to fully cover eyelashes.
4. Place lid (phaco) speculum.
5. Ensure adequate pupillary dilation (prefer pupil diameter of 7 mm or more).
6. Optional: Measure “white-to-white” (limbus-to-limbus) with calipers in case an anterior chamber IOL is needed.
Incision Techniques
Scleral Tunnel Technique
1. Prepare a fornix-based conjunctival peritomy at the limbus using Westcott scissors, tissue forceps; ~9 mm for one-piece lens; ~5 mm if a foldable lens is being used. The peritomy is usually centered around 11:00 or 1:00 o’clock on the side of the surgeon’s dominant hand.
2. Secure hemostasis with wet-field cautery.
3. Create self-sealing scleral tunnel:
a. Use a rounded blade (e.g., #64 or #69 Beaver blade) and 0.12 mm forceps to make a partial (50%) thickness, linear incision vertical and perpendicular to sclera, 2 to 3 mm from limbus (Fig. 8.1).
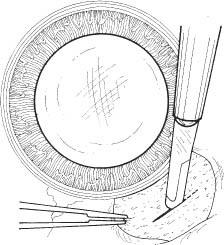
Figure 8.1
b. Extend partial thickness groove incision 2.7 mm to 3.5 mm if a foldable lens is planned and 6.0 mm if a PMMA lens is planned.
c. Use crescent or tunnel incision blade (e.g., Beaver #38, #48) to construct a scleral tunnel of same depth into clear cornea. Maintain a surgical plane parallel to the globe by holding the blade flat against the sclera (e.g., keep blade heel down) (Fig. 8.2).
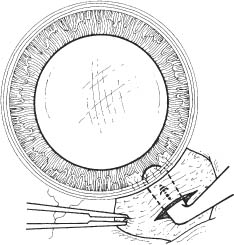
Figure 8.2
d. Continue tunnel construction just past anterior limbal vessels.
4. Perform a paracentesis through clear cornea adjacent to limbus (see Fig. 7.1, p. 23). Place at 10 or 2 o’clock on side of nondominant hand, using a microsurgical knife (e.g., Beaver #75, MVR) (Fig. 8.3).
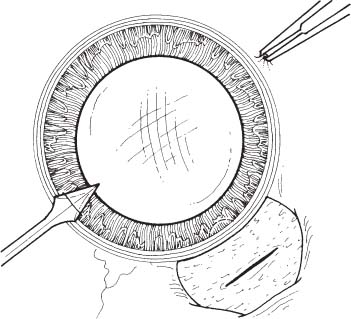
Figure 8.3
5. Optional: Inject 1 ml of 1% nonpreserved intracameral lidocaine (may also use 1:100,000 unpreserved epinephrine to aid in pupil dilation).
6. Inject viscoelastic into anterior chamber through paracentesis port.
7. Use keratome (2.7 mm to 3.2 mm) to slowly enter anterior chamber at the anterior edge of the scleral tunnel, 0.5 mm anterior to the anterior edge of the vascular arcade, on the side of the dominant hand (Fig. 8.4).
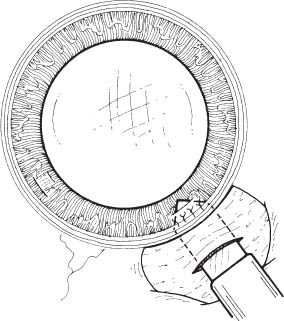
Figure 8.4
Clear Cornea Technique
1. Stabilize and fixate the globe using 0.12 forceps, Fine-Thorton 13-mm fixation ring, or cut end of Wexcel.
2. Perform a paracentesis through clear cornea adjacent to limbus using a microsurgical knife (e.g., Beaver #75, MVR) (see Fig. 7.1, p. 23, and Fig. 8.3).
a. Place at 10 or 2 o’clock on side of nondominant hand if a superior wound is used.
b. Note: If working from temporal side, place paracentesis site at 7 or 11 o’clock for right eye, or 1 or 5 o’clock for left eye, on side of nondominant hand.
3. Optional: Inject 1 ml of 1% nonpreserved intracameral lidocaine for topical cases.
4. Inject viscoelastic into anterior chamber through paracentesis port.
5. Using a keratome, create a clear cornea incision at the desired location (superior or temporal). A triplanar or biplanar incision can be made.
6. Techniques may vary depending on the blade manufacturer’s specifications.
a. For a triplanar incision (Fig. 8.5):
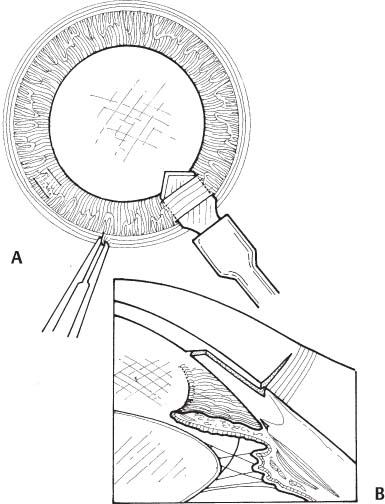
Figure 8.5
i. Make first incision in clear cornea and perpendicular to the cornea plane. Place incision in front of the limbal vessels at a depth of ~250 um using a keratome. Optional: An initial 3.0 mm groove may be placed at the anterior edge of the vascular arcade. If an initial groove is made, make the next incision by depressing on the posterior edge of the groove with the diamond or steel blade of choice.
ii. Flatten the blade against the surface of the eye.
b. For a biplanar incision: Use a straight or angled bi-beveled clear cornea blade.
i. Place tip of blade just in front of the anterior limbal vessels.
ii. Gently press down against the globe, along the heel of the blade so as to engage clear cornea to approximately one half depth with the tip.
iii. Push forward, as the eye is stabilized with a cannula safely placed in the paracentesis (or by holding the conjunctiva/sclera with a 0.12). A wiggle motion is usually not necessary.
7. Construct the second plane of the incision in the corneal stroma parallel to the corneal plane (Fig. 8.5A).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


