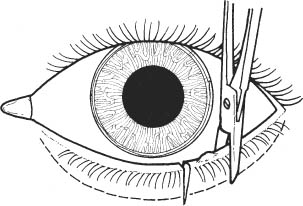
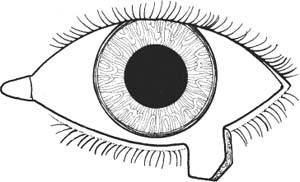
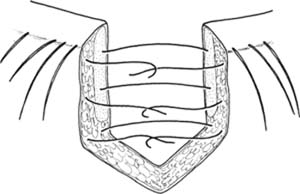
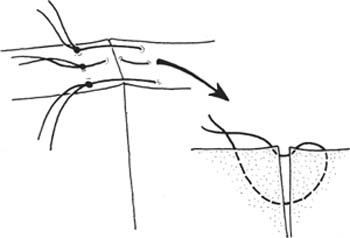
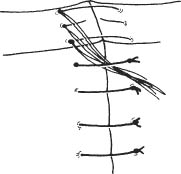
46 The following chapter discusses the general repair of a lid margin defect, whether of surgical or traumatic etiology. Situations in which this technique is used include: See Chapter 3. For traumatic lid lacerations: 1. Rule out injury to the eye. 2. Carefully inspect injury site. a. Rule out involvement of canaliculus and lacrimal system. (If lacerated, see Canalicular Repair with Intubation section later in this chapter). b. Assess levator function to rule out injury to the levator aponeurosis. See Ptosis Repair by External Levator Aponeurosis Advancement section in Chapter 54, p. 279. 3. Administer tetanus prophylaxis as indicated. 4. Administer prophylactic intravenous or oral antibiotics. 1. Apply topical anesthetic. 2. Subcutaneous infiltration with a 50:50 mixture of lido-caine 2% plus 1:100,000 epinephrine and 0.75% bupivacaine. a. Infiltrate area to be manipulated via cutaneous or conjunctival route. 3. Prepare and drape in the usual sterile manner. 4. Place scleral shield. Figure 46.1 5. Incise lid margin perpendicularly at one side of area to be excised (Fig. 46.1). a. Secure lid with forceps or traction suture. b. Use #15 Bard-Parker blade scalpel or scissors to perform incision. c. Extend incision just below edge of tarsus. d. Excise additional several mm if excising neoplasm. 6. Similarly, perform a second vertical incision at other side of lesion, completely encompassing the area of interest (Fig. 46.1). Figure 46.2 7. Excise the lid segment as a pentagon, completing the incisions inferior to the tarsus (scalpel or scissors) (Fig. 46.2). Figure 46.3 8. Approximate tarsus with three interrupted, partial thickness absorbable sutures (e.g., 6–0 Vicryl) (Fig. 46.3). a. Make certain that suture does not protrude posteriorly through conjunctiva. b. Sutures may be left untied until lid margin is approximated. Figure 46.4 9. Approximate lid margin (Fig. 46.4). a. Use nonabsorbable suture (e.g., 6–0 silk). b. Sutures should be ~1–2 mm on each side of wound and 1–2 mm deep. c. Suture 1: Use a vertical mattress suture through the gray line (create wound eversion to prevent lid notching) or use simple interrupted sutures. d. Suture 2: Use an interrupted suture at lash line. e. Suture 3 (optional): Use an interrupted suture through the posterior lid margin. Figure 46.5
Eyelid Lacerations/Eye Defects/Biopsies
 Repair of Full-Thickness Lid Margin Lacerations and Defects
Repair of Full-Thickness Lid Margin Lacerations and Defects
Indications
 Full-thickness marginal lid biopsy and excision of lid margin lesions.
Full-thickness marginal lid biopsy and excision of lid margin lesions.
 Treatment of focal trichiasis.
Treatment of focal trichiasis.
 Repair of full-thickness lacerations involving the lid margin.
Repair of full-thickness lacerations involving the lid margin.
 Treatment of eyelid ectropion or entropion where full-thickness resection of eyelid is desired.
Treatment of eyelid ectropion or entropion where full-thickness resection of eyelid is desired.
Preoperative Procedure
Instrumentation
 Scleral shield
Scleral shield
 Toothed forceps
Toothed forceps
 Scalpel with #15 Bard-Parker blade
Scalpel with #15 Bard-Parker blade
 Scissors
Scissors
 Cautery
Cautery
 Needle holder
Needle holder
 Sutures (6–0 Vicryl on spatulated needle, 6–0 silk)
Sutures (6–0 Vicryl on spatulated needle, 6–0 silk)
Operative Procedure
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


