Perforations of the Tympanic Membrane
Dennis S. Poe
Perforations of the tympanic membrane are caused by a number of etiologies, most commonly suppurative otitis media. Perforations cause hearing loss and predispose patients to drainage, pain, and complications from otitis media.
The earliest known evidence of a tympanic membrane perforation was described by Benitez (1) in an Egyptian mummy, Pum II. There was an oval-shaped perforation in which the margins demonstrated histologic evidence of inflammation and repair consistent with otitis media. The process of acute suppurative otitis media leading to perforation of the tympanic membrane was described by Shambaugh (2), who noted that toxins from beta-hemolytic Streptococcus were capable of producing rapid necrosis of the tympanic membrane.
Trauma is the second leading cause of tympanic membrane perforations. Injury may be due to direct trauma or to barotrauma. Direct trauma includes self-inflicted injuries with cotton-tipped applicators and other instruments used to clean or scratch the ear canal, iatrogenic injuries from attempts to remove foreign bodies or cerumen, welding slag, waterskiing injuries, temporal bone fractures, and injuries from flying debris. Barotrauma includes aerotitis, waterskiing injuries, slap injuries to the ear, and explosions.
The failure of perforations to heal spontaneously is due to many factors, including size and location of the perforation, severity of tissue injury, approximation of the margins, tendency of epithelial margin to develop squamous ingrowth, presence of infection, and health of the surrounding tympanic membrane. Perforations may persist following the removal or extrusion of tympanostomy tubes and is correlated with the diameter of the tube or duration of the tube in the tympanic membrane (3,4). Spontaneous healing of traumatic perforations occurred in 73% of the cases reported by Kristensen et al. (5).
The severity of the conductive hearing loss due to tympanic membrane perforation appears to be correlated with the size of the defect, with larger perforations generally causing greater hearing loss. The hearing loss is typically worse in the lower frequencies. Perforations overlying the round window are said to have a disproportionately greater hearing loss than a comparably sized perforation located elsewhere on the tympanic membrane due to a lack of phase and amplitude differences between the oval and round windows (6). However, Voss et al. (7) in a cadaveric model have demonstrated that the location of the perforation, at least of those with a diameter of 1 mm or less, had no influence on the size of the conductive hearing loss.
The concept of repairing perforations of the tympanic membrane was revolutionary when it was introduced by Wullstein (8) and Zöllner (9) in 1952 and 1955, respectively. It was realized late in the nineteenth century that manipulation of the ossicles could improve hearing in some cases. The incidence of postoperative deafness and meningitis was sufficiently high that the concept of ear surgery for correction of hearing loss was condemned for decades. The development of fenestration surgery for otosclerosis rejuvenated the concept of hearing restoration by ear surgery, but it remained unthinkable for perforations, because prevention and treatment of infections were the only important goals in chronic otitis media. The very concept of tissue grafting of a tympanic membrane over air seemed to defy the presumed necessity for graft placement on a vascularized base. In 1950 Moritz (10) described the use of pedicle flaps as a staged procedure to close draining perforations and cover the round window before a second-stage fenestration procedure. Zöllner (11) in 1951 adapted the pedicled flap techniques to close simple perforations of the tympanic membrane. Wullstein (8) in 1952 was the first to perform tympanoplasty using a free skin graft placed lateral to the perforation (overlay graft). The success of tympanoplasty gave birth to a new era of reconstructive ear surgery. Skin grafts were complicated by graft eczema, inflammation, perforations, and iatrogenic cholesteatoma. House and Sheehy (12) reported that the skin from the auricular meatus was more suitable than skin from a remote site. Vein graft perichondrium and homograft were employed and offered various benefits (13, 14, 15). In 1961 Storrs (16) reported the use of temporalis fascia, which quickly gained widespread acceptance.
Techniques to place the graft medial to the tympanic membrane (underlay) using fascia and the loose areolar layer of temporoparietal fascia began to emerge and were popularized by Glasscock (17). Overlay procedures had the technical advantage of being easier to place the graft on the lateral surface of the tympanic membrane, which had been denuded of all epithelium. However, the technique requires a wide canalplasty and precision in packing the tympanic membrane graft in position to minimize scarring and blunting of the anterior canal sulcus or lateralization of the graft. The underlay technique minimizes the possibility of blunting or lateralization because the skin of the anterior ear canal and annulus is left in place. However, placement of the graft medial to the tympanic membrane can be more technically challenging. Given the advantages and disadvantages of both techniques, it is ideal to be well trained in the use of either so that the surgeon may select a technique based on the location, size, and character of perforation. The author prefers the underlay technique for most cases because of the reduced complication rate and reduced time required for performance of the procedure. It is a useful technique even for total tympanic membrane replacement.
Techniques to place the graft medial to the tympanic membrane (underlay) using fascia and the loose areolar layer of temporoparietal fascia began to emerge and were popularized by Glasscock (17). Overlay procedures had the technical advantage of being easier to place the graft on the lateral surface of the tympanic membrane, which had been denuded of all epithelium. However, the technique requires a wide canalplasty and precision in packing the tympanic membrane graft in position to minimize scarring and blunting of the anterior canal sulcus or lateralization of the graft. The underlay technique minimizes the possibility of blunting or lateralization because the skin of the anterior ear canal and annulus is left in place. However, placement of the graft medial to the tympanic membrane can be more technically challenging. Given the advantages and disadvantages of both techniques, it is ideal to be well trained in the use of either so that the surgeon may select a technique based on the location, size, and character of perforation. The author prefers the underlay technique for most cases because of the reduced complication rate and reduced time required for performance of the procedure. It is a useful technique even for total tympanic membrane replacement.
OFFICE MANAGEMENT OF TYMPANIC MEMBRANE PERFORATIONS
Tympanic membrane perforations may be symptomatic with hearing loss or otorrhea or present as incidental findings on a routine examination with no symptoms. Pain with infection is unusual because drainage through the perforation will normally prevent the accumulation of pus under pressure. If pain is present with suppurative otitis media, it should be regarded as a potentially ominous symptom of a possible underlying complication (Chapter 18).
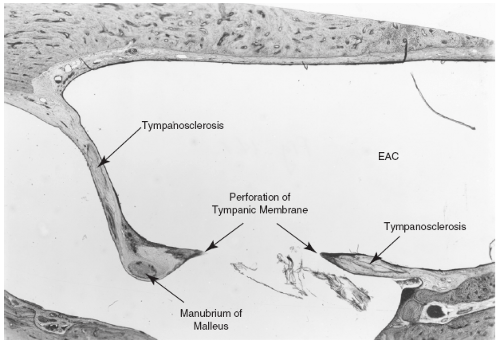 FIG. 14.1 Photomicrograph of chronic perforation of the tympanic membrane with tympanosclerosis. EAC, external auditory canal. |
Perforations are generally classified as central or marginal. Central perforations occur in the pars tensa and have a rim of tympanic membrane circumferentially. Size is variable, and the shape is typically round, oval, or kidneylike. The edges of long-standing perforations are rounded, with keratinized stratified squamous epithelium of the external surface approximating the middle ear mucosa at the margin of the perforation.
Marginal perforations include defects of the pars tensa that extend to the tympanic annulus and any perforation located in the pars flaccida. Marginal perforations may be preceded by retraction of the tympanic membrane, typically in the posterosuperior portion of the pars tensa or in the pars flaccida.
Chronic perforations may be associated with tympanosclerosis, hyalined plaques embedded in the tympanic membrane (Fig. 14.1). Histologically, there is hyalinization of the subepithelial connective tissue with dystrophic calcification, usually involving the middle fibrous layer of the tympanic membrane and in some cases the middle ear mucosa. Hearing loss usually occurs only when the ossicles become involved and fixed (4,5).
PATIENT SELECTION FOR SURGERY
The principal indications for surgery are hearing loss or infection that may be intermittent or chronic or evidence of early formation of cholesteatoma. Repair of a chronic, stable,
asymptomatic perforation may be done to obviate the need for water precautions. Complicating factors such as allergic rhinitis, sinusitis, other nasal pathology, or immunocompromised state should be managed to the best extent reasonable preoperatively. A comprehensive medical history and physical examination should be completed.
asymptomatic perforation may be done to obviate the need for water precautions. Complicating factors such as allergic rhinitis, sinusitis, other nasal pathology, or immunocompromised state should be managed to the best extent reasonable preoperatively. A comprehensive medical history and physical examination should be completed.
The success of tympanoplasty surgery depends to a large degree on the patient having adequate eustachian tube function. Attempts to objectively evaluate eustachian tube function have not been able to reliably predict which patients will fail tympanoplasty surgery. Many tests use sophisticated means for recording tubal opening pressures in response to varying gradients of applied pressure, but the conditions are actually nonphysiologic and correlate only poorly with clinical success or failure. Bluestone and Cantekin (18) have shown that the simple ability to equalize middle ear pressure by swallowing while the pressure is varied with a tympanometry bridge does correlate well with tympanoplasty success. Failures of equalization tests, however, have not accurately predicted tympanoplasty failures. Other methods of eustachian tube evaluation have shown similar correlations for predicting success when function is good but are poorly correlated with tympanoplasty failures (19, 20, 21, 22, 23, 24). Normal tubal function on the contralateral ear does not adequately predict normal tubal function in the perforated ear. Magnuson and Falk (25) observed that variation of tubal function over time is one reason for poor predictive value. It is well known that patients may have successful closure of the perforation for many months, or even years, and suddenly fail after an acute episode of eustachian tube dysfunction.
There is controversy concerning timing of repair of perforations in children. The incidence of otitis media declines sharply after age 6, and the eustachian tube has reached adult length generally by age 7 (26). Symptomatic perforations with infection or hearing loss may be closed at any age. Closure of asymptomatic perforations must be individualized. Generally it is postponed until age 7 when the incidence of upper respiratory infections and dysfunction of the eustachian tube decreases.
The risks and benefits of tympanoplasty should be carefully weighed in all cases. When the perforation involves the better or only hearing ear, repair should be undertaken only when circumstances are compelling, such as with intractable otorrhea, which itself risks inner ear injury.
Examination of the tympanic membrane preoperatively is optimally done with a binocular microscope. Inspection of the perforation edge is done to evaluate the quality of the surrounding tympanic membrane (atrophic or healthy) and to look for additional disease such as migration of skin onto the medial surface of the tympanic membrane, scarring, tympanosclerosis, or myringitis. Examination of the middle ear through the perforation may demonstrate mucosal disease or complications such as cholesteatoma or granulation. The status of the ossicles should be assessed as to their presence, health, and position. Ossicular mobility can be judged by gentle palpation when necessary.
Otorrhea should be treated preoperatively to improve the success rate of tympanoplasty and to reduce postoperative infection. Two weeks of topical antibiotic drops are usually sufficient in those ears that will respond to this treatment. Otic topical drops often contain a corticosteroid to minimize pruritus, inflammation, and edema but are not necessary for successful treatment. A wide range of otic and ophthalmic drops may be used successfully. Drops that contain ototoxic antibiotics are routinely used in inflamed ears, but their use is discouraged in noninflamed ears, in which absorption of the ototoxic medications via the round window may occur more readily. Persistent drainage after adequate topical therapy is an indication for culture. Cultures should include routine and fungal organisms. Tuberculosis should always be considered in endemic areas. If a fungal culture is positive, appropriate treatment may be added to or used to replace the antimicrobial otic drops. When all efforts to dry up the ear fail, mastoidectomy should be considered, but tympanoplasty alone is often successful in cases of uncomplicated chronic otitis media without cholesteatoma (27,28). Ears that persistently drain clear mucoid secretions in the absence of middle ear infection are thought to be of inflammatory or allergic response to airborne allergens and may respond to appropriate allergy therapy (29). Ears that chronically drain clear, watery fluid should always be evaluated for a possible cerebrospinal fluid leak.
Comprehensive audiometry with air-bone and speech evaluations should be done in all patients preoperatively.
MYRINGOPLASTY PROCEDURES
Paper Patch Myringoplasty
Paper patches were widely used in the 1940s and 1950s prior to the advent of formal tympanoplasty. The technique usually required multiple treatments in efforts to induce healing. The technique is most successful in traumatic perforations, in which the paper may help to align the injured portions of the tympanic membrane. Chronic perforations require some freshening of the margin of the perforation to deepithelialize it, gently removing the edge of the margin with a sharp pick or by cauterizing the edge by applying a 50% solution of trichloroacetic acid. The acid may be applied using a tiny cotton-tipped applicator or by dipping a 20-gauge suction into the solution, wicking away the excess drops, and applying the residual to the perforation edge. The cauterized edge takes on a white appearance.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


