Pediatric Vitreoretinal Surgery
Kimberly A. Drenser
Michael T. Trese
Philip J. Ferrone
The pediatric patient presents many challenges to the vitreoretinal surgeon that require special consideration relative to surgical circumstances.
Examination and Patient Presentation
Pediatric vitreoretinal surgical patients are often unable to verbalize their visual complaint. Therefore the examiner must often rely on physical examination techniques. The patient is often referred for one of the following diagnoses: no red reflex, suspected retinal detachment, unexplained strabismus, leukocoria, history of trauma, a change in visual function, or unexplained irritability.
Like adult patients, pediatric patients require a good clinical examination. Unlike adult patients, however, pediatric patients are often uncooperative during the examination. In pediatric patients (especially those 1 to 4 years of age, who are often unable to understand the need for examination but are strong enough to effectively resist examination), the examination must be very directed and complete, yet brief enough so as not to lose the cooperation of the child, family, or other caretaker. Because children often have a very short attention span, it is necessary for you to begin gathering information as soon as you enter the examining room: Your initial observations of the child interacting with his or her environment may be the most important piece of information you get from the child.
The physical part of the examination consists of visual acuity assessment. Assessment of vision in preverbal infants is difficult and subjective. Even the Teller and Archer-Droste acuity tests have a subjective component, because the observer must decide whether the infant sees the target.1,2 Given the subjective nature of the testing, it is still necessary to try to judge the presence or absence of light perception. This seems to be most easily assessed by either attraction or aversion to light. As the child gets older, assessment of visual acuity as measured by fixing and following behaviors, followed later by recognition behaviors, becomes possible.
After visual acuity assessment, a history of the child and family are necessary. The purpose of the history is to determine whether an examination under anesthesia, other tests (e.g., electrophysiology, blood workup for genetic markers), or surgical intervention is required. Certainly, one of the greatest risks a systemically compromised child can face is anesthesia; therefore, the surgeon must appreciate the child’s systemic condition as well as the level of risk associated with general anesthesia. Often the vitreoretinal surgeon is not one who makes that decision. We prefer to leave that to the neonatologist/pediatrician and anesthesiologist.
The birth history should include the birth weight, conceptual age (i.e., weeks from conception to the present), gestational age (i.e., weeks from conception to birth), the mother’s due date, pregnancy data (e.g., illness, trauma, drug use, HIV status), and familial ocular and systemic diseases. The mother’s due date is a useful landmark because it gives a reference point as to retinal vascular maturity and foveal formation. Retinal vascular maturity occurs at around the due date to several weeks (rarely even up to 8 weeks) after the due date. Foveal maturation occurs approximately 3 months after the due date. In addition, if retinal detachment occurs as a result of acute retinopathy of prematurity (ROP), it usually occurs 1 or 2 weeks on either side of the due date (see ahead to the Retinopathy of Prematurity section).
Examination Technique
The examination technique varies depending on the child’s age. A premature newborn may be quite tolerant of being wrapped and undergoing scleral depression. Caution must be used when performing scleral depression in an infant with extraretinal vascularization, since it is possible to cause retinal hemorrhage during the examination.3 For examination, we use an indirect ophthalmoscope and a 20-diopter lens to assess the anterior segment and a 28- or 40-diopter lens to examine the retina. We prefer to use a small-pupil, spectacle-mounted, or wireless indirect ophthalmoscope because it gives us greater freedom to move around the child during the examination. We generally have the child lie on his back on an adult’s lap with the child’s head at the adult’s knees. This allows the adult “holder” to control the child’s arms and feet while the examiner controls the top of the head and eyelids. We prefer not to use a lid speculum, but some children are unable to be examined without one. In the circumstance that a speculum is needed, a topical anesthetic is often used, and one must be aware of the potential of a corneal abrasion.
Once the examiner is aware of the information that needs to be obtained from the examination and the child is appropriately positioned, the examination can begin. The examiner must realize that the examination that the child will allow will consist of a randomly organized look at the back of the eye. It is the examiner’s job to piece together the sum of these views into a useful montage. As a general rule, the more struggling that is necessary for the examination, the more frustrated the child, examiner, and family will become, and the less information will be derived from the examination. It may be necessary to examine such a child under anesthesia or to have the child return another day so that a more complete examination can be performed.
Examination Under Anesthesia
Examination under anesthesia should be reserved for the child whose office examination did not answer the clinical questions. This hopefully is a small number of children, but postponement of diagnosis of treatable retinal pathology in children not only makes repair of the retina more difficult but also may lead to amblyopia, the need for retinal reattachment, and a poor visual result. Therefore, the decision to perform examination under anesthesia should be made as one would with any other clinical test associated with some risk. Examination under anesthesia should be performed if information can be gained that can help with the child’s management.
Pediatric Retinal Detachment
General Considerations
All aspects of management of pediatric retinal detachment must be viewed with the realization that all the issues associated with adult retinal detachment are present in the child, but that these circumstances are occurring in an eye that is part of a visual system in the process of learning how to see.
Because of the difficulty of examining the signs as well as recognizing the symptoms of retinal detachment in children, the timing of retinal detachment repair is often unavoidably delayed despite appropriate referral. After retinal detachment or detachment repair, the vigor with which reparative tissue grows may lead to severe stages of proliferative vitreoretinopathy. Our clinical impression, which is in agreement with that of other experienced vitreoretinal surgeons, is that pediatric retinal detachments have a worse prognosis for reattachment and therefore vision, perhaps partly due to severe reproliferation rates. In some series, pediatric retinal detachment is often found in association with some congenital retinal changes that may have an associated retinal or, perhaps even more importantly, vitreous abnormality that predisposes the patient to the retinal detachment.4 In a 1972 study of pediatric aphakic patients in whom a small-wound closed-eye technique was used, 1.5% were found to have retinal detachment at a mean follow-up of 5.5 years.5 In two-thirds of these cases of retinal detachments, there was a coexistent anomaly. Other series on retinal detachment, especially those involving children or trauma, also have reported continuing cicatrization and late retinal detachment.6,7
The 1.5% incidence of retinal detachment reported in the 1972 study5 is much reduced from earlier series, which have shown a 3% to 10% incidence of retinal detachments.8,9 The mechanical difference of using a vitreous cutting system to remove a child’s soft lens versus the older aspiration technique seem to have led to a more controlled cutting of lens and vitreous. This technique is less likely to transmit the cutting and sucking forces from the lens material to the vitreous base, thus avoiding the creation of retinal tears.
Anatomic Considerations
The most obvious anatomic consideration in pediatric retinal surgery is the relatively smaller size of the child’s globe and orbit compared with the adult’s. There are, however, several other important anatomic considerations in pediatric cataract extraction:
The attachment between the vitreous cortex and retina is very firm.
The soft lens and anterior vitreous are attached.
The secondary vitreous in the term infant without ocular disease consists of a very dense collagenous gel. Some authors believe that in term infants, there is no hyaluronic acid present until 4 years of age.10,11 There are, however, many diseases that are associated with a lack of densely formed vitreous (e.g., myopia, retinitis pigmentosa, ROP, familial exudative vitreoretinopathy, Goldmann-Favre disease, congenital retinoschisis, Stickler’s syndrome). Because of the well-formed vitreous and its greater adhesion to the retina disinsertion of the hyaloid and complete removal of the vitreous is often times not possible. Attempts to remove the hyaloid may result in mechanical damage to the retina and even create retinal tears.
A term infant does not have a well-developed pars plana, limiting where the surgeon can safely enter his or her eye for vitreous surgery. As a rule of thumb, an infant 8 months post term has a pars plana approximately 2 mm wide.12 Thus, for vitrectomy, it is necessary to enter much more anterior than the usual adult entry site. Because of the relatively larger size of the lens in relation to the anterior segment in children compared with adults, special care is required if the eye is to be entered without removing the lens.
Rhegmatogenous Retinal Detachment
Although rhegmatogenous idiopathic retinal detachment is less common in the pediatric population, it is important to consider in the primary repair of pediatric retinal detachments. Rhegmatogenous retinal detachments in children are often found accompanying other vitreoretinal pathology or trauma and has been reported in cases of Marfan’s syndrome, Stickler’s syndrome, cataract extraction, and trauma.13,14,15
Scleral Buckling
A child’s eye is prone to more vigorous reproliferation than an adult’s. This can be attributed to (1) a biochemistry that supports cell growth more actively or (2) a tendency toward a longer delay between the time of detachment and the determination of a diagnosis and therapy. This has led us to suggest the use of a higher scleral buckle in children than in adults. For primary rhegmatogenous retinal detachments, we use a sculpted 5 × 7 mm sponge with an encircling 2.5-mm solid silicone band. It is often assumed that the child’s orbit cannot accommodate a large sponge, but we have found that this type of exoplant is well tolerated. Drainage of subretinal fluid is always controversial. We tend to drain subretinal fluid if the retina is highly detached and minimal retinal traction is present. If fluid is quickly drained while extensive traction remains, other retinal tears can occur. In primary rhegmatogenous detachments, however, drainage is often helpful. When drainage is performed we use a scleral cut down with a Beaver blade and retract the scleral flaps with diathermy. A 8.0 silk suture is preplaced between the scleral flaps for closure following the drainage. Children may have extension of the sclerotomy if the flaps are not secured with a suture. The choroid is perforated with a 27-gauge needle or a cold 23-gauge diathermy tip. We use nylon sutures to secure the buckle element. A detailed conversation with the parents should include discussion of a second surgery to divide the scleral buckle. This will allow for continued eye growth and will lessen the anisometropic amblyopia. We generally treat the retinal tear with cryotherapy, as this allows for treatment in detached retina.
Complications
Postoperative complications of scleral buckling in children range from limitation of eye growth to development of an amblyopic loss of vision due to cycloplegic use of eyedrops. To avoid these pitfalls as much as possible, approximately 3 months after the scleral buckling operation we divide the encircling band in all children who are less than 2 years of age or whose eye growth is retarded. We choose to divide rather than to remove the element because we believe that continued support is given to the retina by the encapsulated exoplant. To reduce the chance of amblyopia development in the postoperative period, we tend to prescribe 1% atropine drops for 5 days; if both eyes have good visual potential, we often prescribe the drops for use in both eyes. In addition to amblyopia therapy, refractive error, which can usually be pursued leisurely in adults, needs to be aggressively treated.
Giant Retinal Tears
Giant retinal tears in adults have been discussed widely in the literature.16 Giant tears in children, however, have received less attention. The problems in treating pediatric giant tears often revolve around positioning of the patient for weeks after surgery as well as complicated surgical techniques. Delay in diagnosis and the fact that pediatric giant retinal tears are often concurrent with other ocular problems or trauma make these retinal tears even more challenging in children than they are in adults. Thus children often have lower anatomic and visual success rates.4 Children’s level of physical activity and inability to position postoperatively make the consideration of a long-acting tamponade (e.g., silicone oil) very appealing. This may free the child and caretaker from a rigorous positioning regimen. All of the complications of silicone oil must also be considered, such as cataract, glaucoma, corneal decompensation, and reoperation for removal.4,17 We believe that the advantages of silicone oil far outweigh the disadvantages in this population and will usually use it as our first-line tamponade in giant retinal tears in children.
Vitreous Surgery
Over the last decade vitreous surgery in children has become increasingly useful in managing a variety of retinal diseases. Vitreous surgery has the distinct advantage of directly addressing intraocular pathology. This is very useful when the retinal pathology involves vitreous traction and fibrotic membranes. A two-port or three-port system may be used. The two-port system has the advantage of fewer entry sites and less risk of iatrogenic retinal tears, and is the system favored by the authors. Instrumentation consists of a high-flow light pipe, irrigating spatula, intraocular forcep (with or without irrigation), and the 20-gauge vitrector. Smaller gauge vitrectors may be used for simple cases that do not require bimanual dissection, anterior vitreous base work, or removal of fibrotic membranes.
Retinopathy of Prematurity
ROP accounts for a large number of retinal detachments in the pediatric population. The International Classification of Retinopathy of Prematurity helped greatly to improve communication about, and consequently treatment of, ROP. It describes affected eyes in terms of stage, zone, and absence or presence of plus disease18 (Figs. 72.1, 72.2, and 72.3). Screening of premature infants is an important feature in the care of ROP, which is perhaps the most significant and enduring finding of the Cryotherapy for Retinopathy of Prematurity Study (Cryo-ROP Study)19 and has been further supported by the Early Treatment-ROP study.20 We follow the recommendations of the ETROP with early and frequent screening of premature infants. Included in ROP screening are infants weighing 1,500 g or less, and born at 32 weeks gestation or less. The first exam is 4 weeks after birth or at a postmenstrual age of 31 weeks, whichever is latest. The infants are followed every 2 weeks until they reach retinal vascular maturity, which is when nasal vessels in the horizontal meridian have grown to within 1 disc diameter of the ora serrata. Exams should be increased to weekly if the infant’s vacsularity has not matured into zone 2, or if there is stage 1 without Plus disease in zone 2. Twice-weekly exams are recommended for stage 2 zone 2 eyes without Plus disease, or stage 1 or 2 in zone 1 without Plus disease. Eyes require laser ablation when they have Plus disease or stage 3 in zone 1, or stage 2 with Plus disease in zone 2. Consider treatment if there is stage 3 without Plus disease in zone 2. The zone 1 eyes requiring treatment are very high risk and frequently need 2 or more laser treatments to appropriately treat the avascular retina. In particular, zone 1 eyes with stage 3 ROP have “flat” neovascularization, which regresses after laser treatment, revealing underlying avascular retina requiring laser ablation. Additionally, the persistent tunica vasculosa lentis will regress after laser treatment and result in improved pupil dilation and improved view of the anterior retina. Any “skip” lesions should be laser ablated.21 The child who fails to respond to peripheral ablation may require further surgical intervention.
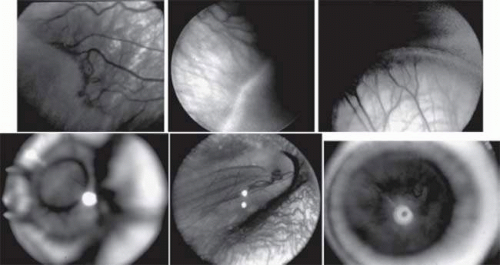 FIGURE 72.1. Stages of retinopathy of prematurity. A: Stage 1, showing a small white line visible between the avascular and vascularized retina. B: Stage 2, with the junction showing a wider white line between avascular and vascularized retina. C: Stage 3, with frank neovascularization extending into the vitreous cavity from the area posterior to the retinal ridge. D: Stage 4A, showing peripheral retinal detachment with the macula attached. E: Stage 4B, with a partial retinal detachment with the macula detached. F: Stage 5, showing total retinal detachment.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|