Tracheal stenosis is a rare, potentially life-threatening condition described as innate narrowing of the tracheal lumen. The causes of tracheal stenosis vary widely. The most common forms result from prolonged intubation, although congenital causes usually involve complete tracheal rings or compression from cardiovascular malformations. The condition historically has harbored a poor prognosis, but significant advances in radiologic diagnosis, cardiac bypass, and endoscopic and surgical treatments have led to a range of options, better overall survival, and reduced morbidity. The complex, long-term manifestations of tracheal stenosis point to the need for individualized treatment as well as multidisciplinary care.
Congenital tracheal stenosis is characterized by structural tracheal constriction. It encompasses a wide range of manifestations, can involve short or long segments, and is associated with pulmonary, cardiovascular, and gastrointestinal malformations. The condition is infrequent, with incidence estimated to be 1 in 64,500 , and represents only 0.3% to 1% of all laryngotracheal stenosis . Most are severe in nature: before the advent of current surgical techniques, mortality was reported to be as high as 79% , mainly because of acute airway obstruction and the lack of effective medical treatment. Tracheal resection and re-anastomosis existed as a solution as early as the late nineteenth century but was contraindicated for stenotic segments longer than 2 cm because of the risk of excess tension. Tracheal release maneuvers developed in the 1950s later extended the resectable length to 25% to 30% of the trachea , and the introduction of cardiopulmonary bypass and the Montgomery T-tube (Boston Medical Products, Westborough, Massachusetts) (used as a stent as well as tracheostomy tube) began to address the intra- and postoperative complications frequently seen with tracheal stenosis. By 1982, Kimura and colleagues introduced the costal cartilage tracheoplasty for long stenotic segments. Their work was followed in 1984 by Idriss and colleagues , who described the pericardial patch tracheoplasty. Problems with granulation formation and prolonged postoperative intubation were addressed when the slide tracheoplasty was proposed in 1989 by Tsang and colleagues and modified by Grillo . The evolution of these surgical techniques has improved outcomes significantly for previously inoperable patients. In addition, better understanding of postoperative care and management of complications has led to improved reported mortality rates ranging from 9% to 21% .
Anatomy/embryology
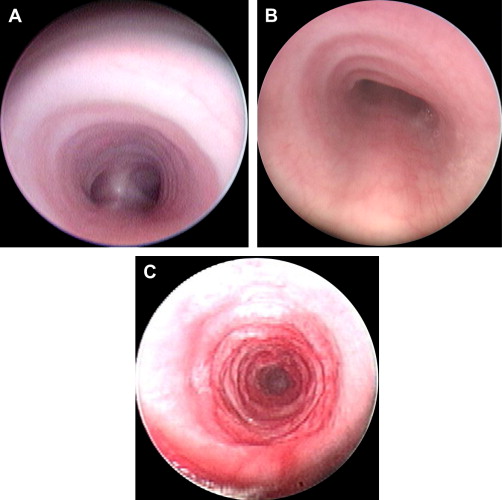
The trachea consists of a fibromuscular sheath supported by approximately 15 to 20 C-shaped cartilaginous rings and the trachealis muscle. It extends from the cricoid cartilage to the carina and is divided into cervical and thoracic segments. The posterior membranous portion of the trachea is absent in the complete tracheal ring variant of congenital tracheal stenosis and is widened in tracheomalacia ( Fig. 1 A–C). Beginning in week 4 of gestation, the respiratory primordium evaginates from the foregut, expanding caudally to form lung buds and differentiating ventrally from the anterior esophagus . The trachea extends caudally along with the esophagus, maturing into the epithelial lining and tracheal glands; separate mesenchymal cells invest around the tube and form cartilage, muscle, and connective tissue by week 8. In the classical theory of development, lateral ridges or folds develop along the tube longitudinally, fusing at the midline to create the tracheoesophageal septum. Improper fusion and inappropriate timing lead to unequal partitioning between the maturing trachea and esophagus , resulting in anomalies including tracheoesophageal fistula. It is hypothesized that developmental lesions occurring by week 4 of gestation result in more severe manifestations of disease, such as tracheal agenesis or abnormalities involving the cardiovasculature. Accordingly, lesions that occur after week 8 may affect only more peripheral structures such as the developing cartilaginous rings .