Bilateral vocal cord paralysis in children with its many causes presents a challenging problem to the pediatric otolaryngologist. Traditionally, management of bilateral vocal cord paralysis includes securing the airway with a tracheotomy and waiting for spontaneous recovery. Surgeons have tried a variety of surgical procedures in lieu of or in addition to tracheotomy, but none are perfect solutions to the problem. This article reviews the current surgical procedures for bilateral vocal cord paralysis in the pediatric population with a particular focus on the senior author’s experience with the endoscopic posterior costal cartilage grafting procedure.
Vocal cord paralysis (VCP) is the second most common congenital laryngeal abnormality found in the pediatric population after laryngomalacia, accounting for 10% of all congenital laryngeal lesions . In recent years, pediatric VCP, although rare, is being diagnosed more frequently. The authors attribute this increasing incidence to more advanced diagnostic techniques and to the improved survival of premature infants and of infants who have complex congenital abnormalities . VCP results from dysfunction of the nerve supply to the laryngeal muscles and should not be confused with anatomic fixation of the vocal cord. The term that encompasses both paralysis and fixation is “vocal cord immobility.” Unilateral and bilateral VCP are different entities with varying presenting symptoms, causes, and treatments. This article focuses on bilateral VCP. Although 30% to 62% of cases of VCP in children are bilateral , the incidence is much lower in the authors’ experience. In most series, a majority of children who have bilateral VCP require placement of tracheotomy to ensure an adequate and safe airway. Forty-eight percent to 62% of children who have bilateral VCP have spontaneous recovery of vocal cord function, avoiding the need for tracheotomy or becoming viable candidates for decannulation if a tracheotomy was performed .
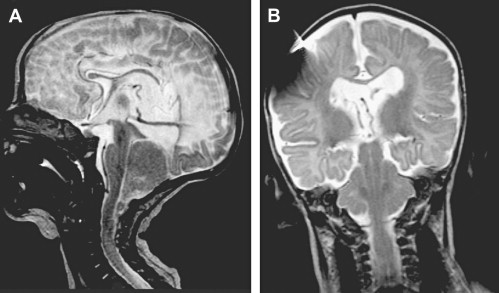
The causes of bilateral VCP differ in adults and children. Most adult cases of bilateral VCP result from total thyroidectomy or malignancy and have very little hope for spontaneous recovery. In infants and children who present with stridor and are discovered to have bilateral VCP, the most common causes are neurologic, traumatic, iatrogenic, or idiopathic . Arnold-Chiari (Chiari II) malformation with associated myelomeningocele and hydrocephalus is the most common neurologic finding, usually diagnosed with an MRI scan revealing cerebellar ectopia below the foramen magnum and a small posterior fossa ( Fig. 1 ). The protrusion of the cerebellar tonsils, medulla, and brainstem through the foramen magnum and into the spinal canal causes stretching and compression of the vagus nerve. This stretching results in bilateral vocal cord dysfunction that usually presents as inspiratory stridor. Intubation and birth trauma related to breach or vertex delivery or the use of forceps can lead to compression or stretching of both recurrent laryngeal nerves in the neck . Iatrogenic causes of VCP include postsurgical complications . Cardiovascular surgery (ie, patent ductus arteriosus ligation and repair of tracheo-esophageal fistula) is a common cause . Idiopathic causes make up a significant proportion of pediatric VCP . In recent years, with better immunizations and antibiotics, inflammatory and infectious causes of VCP are found rarely .
In their excellent overview Rosin and colleagues emphasized the difference between unilateral and bilateral VCP. Of 51 children, 29 had bilateral VCP. Of these 29, 15 had neurologic causes, 6 of which were related to Arnold-Chiari malformation. Six had traumatic causes including intubation injury and birth trauma; 1 had an infectious cause; and in 12 the causes were not identified. The most common cause of unilateral VCP was cardiac surgery. Children who had either bilateral or unilateral VCP presented with stridor and feeding problems. Those who had bilateral VCP were more likely to present also with cyanosis and apnea, whereas those who had unilateral VCP were more likely to present with hoarse voice and cry changes. Nineteen of 29 children (66%) who had bilateral VCP required tracheotomy. In this series of patients, only 16% of children who had bilateral VCP had spontaneous recovery allowing decannulation.
Anatomy
A brief review of the anatomy of the vagus nerve can aid in the differentiation of various causes of VCP . The motor efferent fibers of the vagus nerve originate in nucleus ambiguous and dorsal nucleus, both of which are located in the medulla oblongata. The nucleus ambiguous houses the cell bodies of the branchial or special motor efferent fibers. The dorsal nucleus contains visceral efferent fibers going to the thorax and abdomen. The vagus nerve exits the cranium through the jugular foramen. At the jugular or superior ganglion, sensory fibers to the posterior fossa (meningeal branch) and to the external auditory canal and posterior auricle (auricular branch) arise from the vagus nerve. When the vagus nerve exits the jugular foramen, it is joined by the cranial portion of the accessory nerve. As the nerve passes through the nodose or inferior ganglion, the superior branches join branches of the glossopharyngeus, hypoglossal, and sympathetic fibers to form the pharyngeal plexus serving pharynx musculature (except for the stylopharyngeus) and palate musculature (except for the tensor veli palatini). As the vagus nerve continues through the cervical region, first between the internal carotid artery and internal jugular vein and then between the common carotid artery and internal jugular vein, it gives off the superior laryngeal nerve. This nerve branches into an internal and an external division. The internal division enters the thyrohyoid membrane with the superior laryngeal vessels to provide sensory innervation to the pharyngeal and laryngeal mucosa above the true vocal fold. The external division travels to innervate the cricothyroid muscle.
The course of the vagus nerve into the thorax differs on the right and left side. The right vagus nerve travels in front of the subclavian artery into the thorax and abdomen. The right recurrent laryngeal nerve branches off the vagus and travels posteriorly behind the subclavian artery back superiorly into the neck along the tracheoesophageal groove. It enters the larynx at the cricothyroid joint and provides motor innervation to all the laryngeal muscles except the cricothyroid muscle as well as sensory innervation to the laryngeal mucosa below the vocal fold. The left vagus nerve takes a similar course in front of the arch of the aorta continuing into the thorax and abdomen. The left recurrent laryngeal nerve arises behind the aorta near the remnant of the ductus arteriosus and ascends to the larynx in the tracheoesophageal groove. Its longer course makes it more susceptible to injury.
VCP is caused by injury to the vagus nerve from its nuclei intracranially to its peripheral branches. Central lesions such as cerebral agenesis or nucleus ambiguous agenesis or dysgenesis can cause VCP . Any traction or compression injury along the path of the vagus nerve may result in vocal cord dysfunction. A high injury to the vagus nerve can result in devastating sequelae involving swallowing, speech, voice, and airway.
Presentation and diagnosis
Laryngeal paralysis manifests in accordance with the dysfunction of the three main roles of the larynx, namely, airway, voice, and deglutination. The most common presenting symptom in children who have bilateral VCP is stridor. Children who have bilateral VCP are more likely to present with stridor and dyspnea than with dysphonia and aspiration. In fact, they often have a normal voice, because their vocal cords usually are in a paramedian position with abductor paralysis. Although patients who have unilateral VCP also may present with stridor, they more often have voice and deglutination problems .
The authors believe that any child who presents with inspiratory stridor should undergo endoscopic examination of the larynx. Flexible fiberoptic endoscopy can be performed in clinic or at the bedside. Although flexible fiberoptic endoscopy is the reference standard for the diagnosis of VCP, flexible endoscopy has its drawbacks including technical difficulties resulting from the neonatal and infant anatomy (particularly overhang of the apices of the arytenoids and aryepiglottic folds obscuring the view of the posterior glottis and vocal cords), the lack of suction to address secretions, and the need for some degree of cooperation from patient. Pediatric flexible endoscopes with diameters less than 3 mm can be passed transnasally easily in most infants. An awake patient gives the best examination of vocal cord mobility, but to rule out vocal cord fixation, microdirect suspension laryngoscopy must be performed in the operating room. Direct palpation of the arytenoids to assess for fixation can be done using the laryngeal suction device. Pitfalls of the microdirect rigid laryngoscopy include tethering the true vocal cords by inserting the rigid endoscope too deeply into the endolarynx and failing to find the small window of the depth of anesthesia that allows vocal cord mobility with spontaneous ventilation without laryngospasm. While the patient is under general anesthesia, comorbid conditions, such as subglottic stenosis and tracheomalacia, should be sought. If possible, documentation with digital photographs and videos should be obtained to allow serial comparisons by the otolaryngologist performing the examination and by colleagues who may review the examination in consultation and for confirmation ( Fig. 2 ).
In addition to laryngoscopy, additional studies can aid in securing the diagnosis of vocal cord immobility. Noninvasive studies including CT scan and ultrasound have been studied in children but are not standard practice for diagnosis of VCP . Vats and colleagues did show that ultrasound diagnosis of VCP was 81.8% concordant with endoscopic diagnosis in 55 children age 3 days to 12 years. They found ultrasound to be safe, noninvasive, well tolerated, easy to perform and to interpret, and readily available.
The role of laryngeal electromyography (EMG) in contributing to the diagnosis and prognosis of vocal cord immobility in children has been debated, in part because the standard awake, percutaneous technique used in adults is not practical. Jacobs and Finkel proposed using laryngeal EMG as an adjuvant procedure for unclear diagnosis of VCP versus fixation or combined pathologies. This group described their EMG technique performed in the operating room under general anesthesia with spontaneous ventilation. In the study, the authors placed the electrodes directly into the posterior cricoarytenoid muscle and thyroarytenoid muscles via a direct laryngoscopic approach. Normal EMG with posterior cricoarytenoid muscle activity during inspiration and thyroarytenoid muscle activity in expiration is found in vocal cord immobility secondary to arytenoid fixation, and electromyographic evidence of denervation is expected in VCP. The reliability of laryngeal EMG in children is highly dependent on the placement of the electrodes by the otolaryngologist and the interpretation of the data by an experienced electromyographer. Because of the larynx in children is smaller, even a small amount of postprocedure edema may precipitate airway compromise. Until EMG studies are performed on larger numbers of children and show advantages over standard endoscopy, this technique remains investigational.
Presentation and diagnosis
Laryngeal paralysis manifests in accordance with the dysfunction of the three main roles of the larynx, namely, airway, voice, and deglutination. The most common presenting symptom in children who have bilateral VCP is stridor. Children who have bilateral VCP are more likely to present with stridor and dyspnea than with dysphonia and aspiration. In fact, they often have a normal voice, because their vocal cords usually are in a paramedian position with abductor paralysis. Although patients who have unilateral VCP also may present with stridor, they more often have voice and deglutination problems .
The authors believe that any child who presents with inspiratory stridor should undergo endoscopic examination of the larynx. Flexible fiberoptic endoscopy can be performed in clinic or at the bedside. Although flexible fiberoptic endoscopy is the reference standard for the diagnosis of VCP, flexible endoscopy has its drawbacks including technical difficulties resulting from the neonatal and infant anatomy (particularly overhang of the apices of the arytenoids and aryepiglottic folds obscuring the view of the posterior glottis and vocal cords), the lack of suction to address secretions, and the need for some degree of cooperation from patient. Pediatric flexible endoscopes with diameters less than 3 mm can be passed transnasally easily in most infants. An awake patient gives the best examination of vocal cord mobility, but to rule out vocal cord fixation, microdirect suspension laryngoscopy must be performed in the operating room. Direct palpation of the arytenoids to assess for fixation can be done using the laryngeal suction device. Pitfalls of the microdirect rigid laryngoscopy include tethering the true vocal cords by inserting the rigid endoscope too deeply into the endolarynx and failing to find the small window of the depth of anesthesia that allows vocal cord mobility with spontaneous ventilation without laryngospasm. While the patient is under general anesthesia, comorbid conditions, such as subglottic stenosis and tracheomalacia, should be sought. If possible, documentation with digital photographs and videos should be obtained to allow serial comparisons by the otolaryngologist performing the examination and by colleagues who may review the examination in consultation and for confirmation ( Fig. 2 ).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


