Pediatric Ophthalmology
Edited by P. F. Gallin
Thieme Medical Publishers, Inc.
New York ©2000

21

Pediatric Retinal Examination and Diseases
The safe and informative retinal examination of children under 18 years of age is one of the most difficult challenges facing both the pediatric ophthalmologist and the general ophthalmologist caring for children. This chapter will focus on the indications and techniques for such examinations and will briefly cover important entities that need to be considered any time a child complains of a decrease or change in vision or unusual visual behaviors are noted. An exhaustive treatise on all pediatric retinal diseases is beyond the scope of this work, and can be found elsewhere.1–3
 Retinal Examinations in Children
Retinal Examinations in Children
When Should Children Have Dilated Fundus Examinations?
The indications, frequencies, and techniques of general pediatric examinations are covered elsewhere.1–3 Some clues to the need for an especially careful and detailed retinal examination include a family history of progressive visual loss or blindness, night blindness, nystagmus or strabismus, or enucleation. Consanguinity, maternal drug or alcohol use, prenatal exposure to viruses (including HIV if known) and other serious infections, or therapeutic medication use during pregnancy indicate a high risk of retinal problems. Low birth weight, difficult labor and delivery with asphyxia, and a prolonged stay in the hospital after birth indicate serious medical problems. A history of a lack of early visual behaviors or peculiar eye position or movements is also important. Children in the foster care system may be seen without a complete or accurate medical or social history of either mother or child; these children should be considered high risk and examined promptly and thoroughly.
The indications for retinal examination vary considerably by the age of the child. An infant who has clear media, an abnormal Bruckner test (see below), and nystagmus requires urgent evaluation. A toddler manifesting a change in visual behavior, inattention to formerly attractive objects, or loss of previously attained developmental milestones needs a retinal evaluation. A school-aged child with falling grades, difficulty with reading or seeing the blackboard, and poor attention should be thoroughly examined for retinal pathology. At least one dilated fundus examination along with a retinoscopic manifest in all children prior to starting school has been advocated by many specialists and is certainly the ideal protocol to recommend. Fewer than 5% of children in the United States ever receive such an evaluation.
How Do I Examine a Child’s Retina When He Won’t Sit Still?
Although adults recognize the advantages in putting up with the inconvenience of a retinal examination, the benefits are often lost on children. A few strategies can be tried before arranging for an examination under anesthesia (EUA). First, do not rush into putting drops in the eye and beginning scleral depression immediately after entering the office. Spend a few moments speaking to the child and parents in a normal tone about nonthreatening subjects. Allow the family a few moments to become comfortable with you. If necessary, let the child play in the exam room or waiting room to calm down and become bored.
Second, plan a strategy appropriate for the child’s age. Infants may be wrapped in blankets like a papoose for quick peeks in the eye. Alternatively, a mother’s lap with the child’s legs under her elbows and the child’s elbows pinned to his ears works as well as a papoose board. Infants will tolerate a great deal if they are fed during the examination. Teenagers can frequently be persuaded to go along with an examination to get away from your office. Children between these two age groups can be nearly impossible to examine. Attractive loud toys or interesting videos can be helpful. Keeping the examiner’s head out of the line of sight of the unexamined eye is important if you are trying to distract the child. If necessary, employ fathers, grandparents, or other accompanying adults if strong-arm tactics are used—your office personnel should be reserved for other tasks such as drops, vision testing, and assistance with later exams. Use a 28- or 30-diopter lens and low light intensity to scan the retina quickly and determine whether further evaluation is needed. Unfortunately, bribery, threats, or distractions are often attempted with limited success. Some pediatricians may try sedation with benzodiazepines, intramuscular DPT (Demerol, Phenergan, Thorazine), or chloral hydrate for younger children with some success; this strategy should be used with caution as sedatives may have dangerous side effects.
Third, plan an examination at quiet times when the office is empty; examining a retina in a minimally cooperative child is time consuming at best. The added stimulation of a crowded office, ringing telephones, and your impatience to move on to another patient will affect any child. If you have tried your best and cannot see the retina well enough to accurately localize and draw a lesion in the retina, perform the EUA.
What Dilating Drops Do I Use?
In infants use Cyclogyl 0.5%, one drop twice in the eye; see the infant 30 to 40 minutes later. In toddlers, apply Cyclogyl 0.5% (light iris) or Cyclogyl 1% (dark iris) combined with Neosynephrine 2.5%, one drop of each twice in each eye; see the child 30 to 40 minutes later. Older children and teenagers may be dilated in the same manner as adults. Dilation may be difficult in premature infants with pulmonary disease in the hospital; the doses mentioned for infants may be doubled, but the child needs to be watched closely for increased body warmth and irritability.
How Do I Do an Exam under Anesthesia?
The risks of EUA when done by an experienced anesthesiologist familiar with pediatric patients and techniques are low.4 In many large hospitals, anesthesiologists boarded in both disciplines are available for this purpose. The examination is performed under general anesthesia given by mask without prior sedation and without an in-dwelling intravenous line.
When Do I Do a Fluorescein Angiogram?
Fluorescein angiography5 is performed when one of three concerns exists: (1) when retinal or choroidal ischemia is suspected, (2) when abnormal blood vessel growth or anatomy is noted, and (3) when abnormal vascular permeability exists, such as with macular edema. In children, diseases that lead to ischemia in the retina are uncommon but include important disorders such as familial exudative vitreoretinopathy, incontinentia pigmenti, sickle cell disease, and retinopathy of prematurity (ROP). Abnormal blood vessel growth may occur in the setting of retinal ischemia or in retinoblastoma or other tumors, or they may exist in hamartomatous lesions occurring in the phakomatoses or Coats’ disease. Usually these conditions are confirmed with ophthalmoscopy alone. However, angiography may help to differentiate one type of lesion from another based on filling pattern and presence of leakage in late phase images. Third, permeable retinal vasculature may occur in any condition causing an abnormality of vessels. This is most critical when it causes macular edema, commonly in patients with intermediate uveitis or long-standing juvenile onset diabetes mellitus. Characteristic angiographic appearance also helps in the diagnosis of conditions such as Stargardt’s or Best’s diseases.
Intravenous bolus injections of fluorescein sodium are required to accurately assess the arteriovenous transit in an eye as well as imaging lesions such as microaneurysms, which are best seen in early phase pictures before leakage obscures them. In school-aged and adolescent children, minimal dose adjustment may be made on adult dosing schedules. In younger children and those unable to tolerate or cooperate with intravenous injections, several studies suggest protocols for oral administration of dye. With computerized imaging systems and software, image enhancement allows accurate visualization of abnormal vessels, ischemic retina, and macular edema with reasonable accuracy. The transit of dye is, however, gradual and delayed.
When Should I Obtain Electrophysiologic Studies?
Useful clues to the need for electrophysiologic studies include family histories of visual loss with a normal retinal exam and obvious decreased vision, attenuation of the retinal vasculature in any child with unexplained visual problems, or a suspected storage disease with a retinal component (e.g., Batten-Vogt-Spielmayer family). Two other types of pediatric patients are also referred for electrophysiologic testing. The first group is children suspected of having an inherited retinal dystrophy such as retinitis pigmentosa (RP) or a vitreoretinopathy and related systemic syndromes. The second broad category is children with apparent subnormal vision with strabismus or nystagmus without obvious retinal abnormalities on examination.
In any patient with congenital nystagmus, after ruling out a sensory etiology such as cataract, a thorough battery of tests must be done to diagnose the cause. More than 90% of patients with congenital nystagmus have been found to have one of a group of diagnoses affecting retinal function: albinism, Leber’s congenital amaurosis and related RP, achromatopsia, or congenital stationary night blindness (CSNB). In each case, early fundus examination may be normal, and in all cases visual behaviors and responses are minimal or absent. The use of electrophysiologic testing may differentiate these entities from each other and from delayed visual maturation in which physiologically normal eyes fail to maintain fixation. Serial use of electrophysiologic testing may also show improvement in retinal function from infancy to early childhood, as expected in albinism, achromatopsia, and CSNB.
Electroretinography (ERG) measures the responses of rods and cones to light stimuli (Fig. 21-1). Standardized protocols allow selective evaluation of each photoreceptor; cone dystrophies can be distinguished from early RP with appropriate ERG testing. ERG testing is performed serially to distinguish progressive loss of photoreceptor function, usually hereditary, from nonprogressive pigmentary retinopathies. The ERG measured in response to pattern stimuli can provide one measure of visual acuity and function in young children. A good ERG requires a well-sedated child; an excellent technician may be able to talk a cooperative child through a single eye ERG without sedation.
Leber’s congenital amaurosis (LCA, Fig. 21-2) early-onset RP, and related systemic syndromes show normal or nearly normal fundus appearances early in life with an extinguished ERG. Although other diseases such as achromatopsia or CSNB may have barely recordable ERGs, these typically improve with age. The deficit in LCA and RP will not improve. Delayed visual maturation will also show normal fundi and poor or absent fixation responses, with normal ERG on testing. Distinguishing rod and cone responses will assist in diagnosis; the absence of rods is consistent with early-onset RP, and the absence of cones is consistent with achromatopsia and variants (Fig. 21-3). Thus, ERGs and other electrophysiologic tests are crucial in diagnosing the cause of poor visual development in young children.

FIGURE 21-1. Normal ERG in a child with single flash rod, single flash mixed rod-cone, and single flash cone and flicker response labeled.
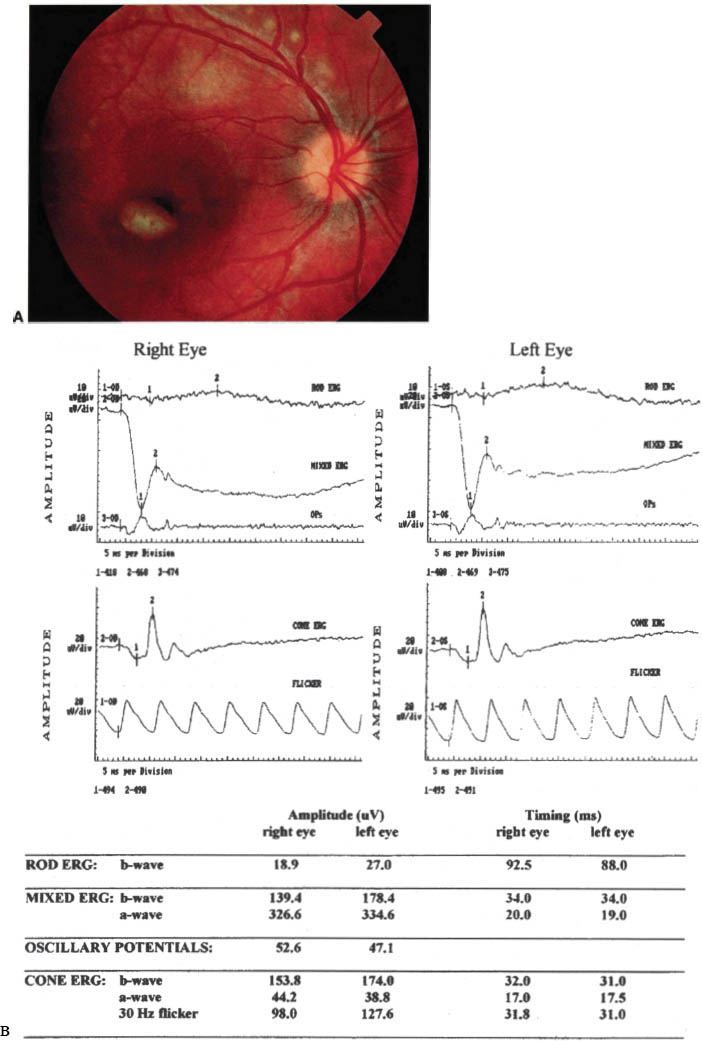
FIGURE 21-2. Extinguished ERG, both rod and cone responses in Leber’s congenital amaurosis.
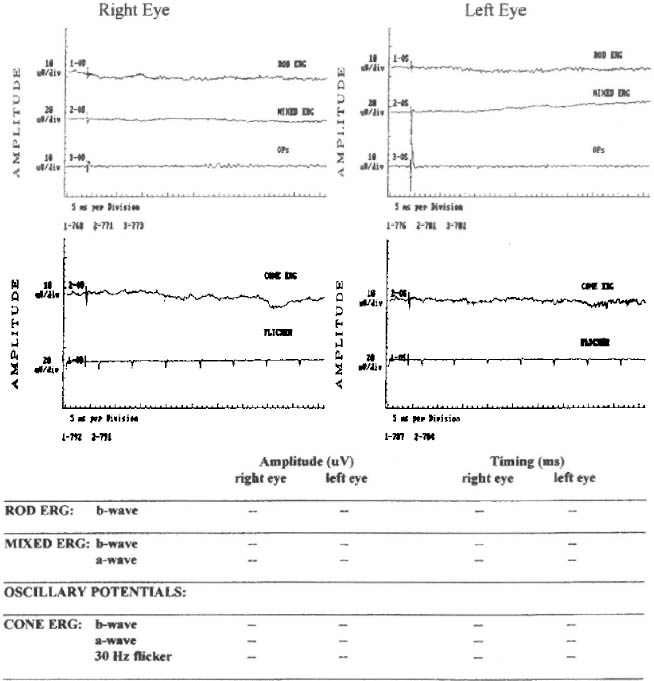
FIGURE 21-3. ERG in congenital achromatopsia (rod monochromatism) demonstrating intact rod response and absent cone response.
The visual evoked potential (VEP) measures the electroencephalogram during repetitive visual stimulation; a tracing averaging many VEPs, the visual evoked response, will detect posterior visual pathway diseases, even in the presence of normal ERG results. The latency of the wave form indicates the state of conduction along the optic nerve; the amplitude of the wave indicates visual acuity. Along with the ERG, the VER can provide useful information about visual function in infants and preverbal children as well as diagnose neurologic causes of poor visual function.
Electrooculography (EOG) measures an electrical potential existing between retinal pigment epithelium (RPE) cells and photoreceptors; the difference between the voltage measured in light- and dark-adapted conditions is expressed as a ratio. A subnormal ratio is observed in 100% of patients with visual loss due to Best’s disease (Fig. 21-4). The EOG, even with normal vision and ERG studies, is the best test for this disease.
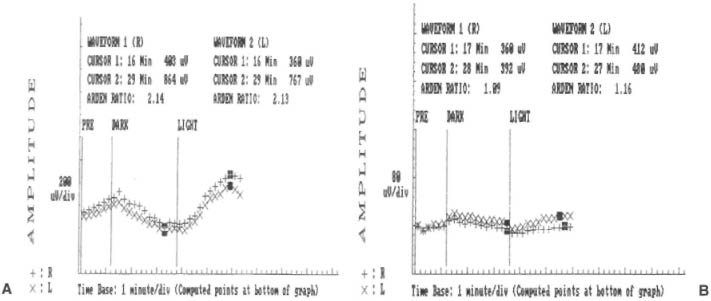
FIGURE 21-4. EOG tracing (A) showing abnormal (>2) light-dark ratio in a case of Best’s Disease (B).
In no instance is electrophysiologic testing6 ordered in isolation. Along with a thorough history and a good ophthalmic examination and genetic and laboratory testing where appropriate, this methodology is combined with visual field, color testing, and dark adaptometry to diagnose the causes of poor vision in children.
When Should I Get an Ultrasound?
A B-scan ultrasound is appropriate to evaluate all eyes in which the posterior pole and retina cannot be directly viewed due to media opacity. In children, corneal opacity and cataract limiting the view of the posterior pole are the most common reasons for ultrasonographic imaging. Often the exam done through closed lids in a drowsy child or hungry infant provides all the information needed without general anesthesia. In most cases, the retina is imaged to rule out retinal detachment in the presence of trauma, hyphema, or vitreous hemorrhage. Thickening of the choroid or choroidal effusions can be evaluated in children with chronic uveitis and hypotony. With extreme care an ultrasound probe can be used in a cooperative child to rule out an intraocular foreign body, althoughthis technique is dangerous with any suspected ruptured globe and is not generally recommended. In addition, details of orbital and intraconal anatomy, such as the echo-free “T-sign” of fluid behind the globe in posterior scleritis or orbital pseudotumor, or the presence of enlarged rectus muscles in various diseases may be imaged. In each case, an ultrasound is obtained relatively rapidly in situations in which computed tomography (CT) scanning or magnetic resonance imaging (not for metallic foreign bodies) can also provide valuable information.
In certain diseases, most typically in retinoblastoma causing leukocoria (Fig. 21-5) or in choroidal osteoma, the ultrasound characteristics of the lesion may provide a clue as to its identity. The presence of echoes typical of calcification assist in diagnosing each of these tumors.
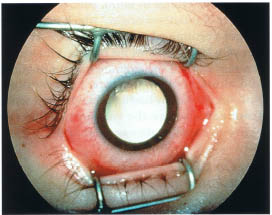
FIGURE 21-5. Leukocoria from a massive intraocular retinoblastoma.
What Abnormalities Should be Referred to Specialists?
If you are confident of your diagnosis and the suspected condition has no specialized treatment, there is no real need for a specialist referral. If you are in doubt about the diagnosis or if your diagnosis carries genetic, social, or familial implications (e.g., Tay-Sach’s or congenital syphilis), it is wise to refer to a specialist for a confirmatory opinion. Retinoblastoma and ROP are two conditions for which specific treatments exist, which occur at sufficiently low frequency that an individual general ophthalmologist may see few cases in a clinical lifetime. Because of the complexity of management these diseases are best left to specialists. Given the significant risks of legal liability to those caring for children with ROP, retinoblastoma, or similar diseases, referral to specialists may be regarded as self-preservation.
What Abnormalities Must I Report to Child Protective Services?
The best advice is better to overcall than undercall, to avoid learning belatedly of the death of an infant whom you had seen. A nonverbal or preverbal child with little or no history, an eccentric pupil, a cataract, retinal or subhyaloid hemorrhages, and retinal tears or dialyses are usual subjects for referrals. The “blood and thunder” fundus or Terson’s pattern of bleeding signifies a mortal injury and is the result of a gradual buildup of violence by the perpetrator; such findings are rare. It is important to keep unexpected settings in mind, such as a consult for “fever of unknown origin,” which may be the result of a beating administered by a clever caregiver who leaves no obvious bruises. Older children may not tell the examiner about ongoing child abuse, even under direct questioning. Thus, the art lies in having a heightened sense of awareness before the violence reaches the stage of irreversible damage and death.
How Do I Tell Parents about Abnormal Findings?
Telling the truth, as simply and honestly as possible and as quickly as possible, is the only policy. More harm and misery are caused by failing to confront reality than by facing it explicitly. A clinician can note an abnormality and if uncertain about its significance simply say, “I don’t know, but I know where to send you to find out.” Misinformation, false hopes, and deliberate equivocation will rebound to your ultimate discredit.
 Specific Conditions
Specific Conditions
Retinopathy of Prematurity
ROP is a disease that affects preterm and low-birth-weight infants receiving supplemental oxygen administration after birth.7 The Multicenter Trial of Cryotherapy for Retinopathy of Prematurity defines high-risk infants as those with birth weights of 1250 g or less. The study concluded that, the lower the birth weight, the higher the risk of developing ROP; a 90% risk of ROP was noted for infants weighing less than 750 g. The pathology of ROP reaches its peak at 1 to 3 months after birth, with retinal detachment and other blinding complications following thereafter. Because treatment has been found effective in preventing the blinding effects of ROP, examination of all low-birth-weight infants and infants receiving supplemental oxygen at birth is mandatory.
The vessels of the retina grow from the optic nerve to the periphery, reaching the ora on the temporal retina after birth. To find and stage the pathology in infants with ROP, an examiner must see the retina beyond the equator for 360 degrees. The committee of ophthalmologists developing the International Classification of Retinopathy of Prematurity found three parameters significant: location of the process (zone), extent in clock hours of pathology, and the severity or appearance of the abnormal vessels. The CRYO-ROP study defined threshold disease requiring cryotherapy as more than five contiguous or eight cumulative (total) clock hours of (stage 3) neovascular proliferation extending from a ridge of issue at the demarcation of vascularized and nonvascular retina in zone I or II with plus disease. Zone I is a circle centered on the disc with radius of twice the distance from the optic disc to the macula. Zone II is a circle extending from zone I to the nasal ora, leaving a small residual temporal crescent (zone III). Plus disease is defined as dilatation and tortuosity of vessels in the posterior pole as well as adjacent to the ridge of developing blood vessels. Retinal lesions are categorized by the highest stage of disease observed in each clock hour. Treatment of threshold disease with cryopexy or laser via indirect ophthalmoscopy significantly decreases progression to more advanced disease.
Regression of most nonthreshold disease without serious vascular or retinal sequelae is the most common outcome in eyes with ROP. Advanced ROP, if untreated or unsuccessfully treated, leads to retinal detachment on the basis of traction originating at the line of vascularizing tissue. This is defined as stage 4 disease if a partial detachment, with or without extension to the macula (A and B, respectively), exists. Stage 5 disease includes funnel detachments, staged further depending on the anatomy of the funnel. Because the visual outcomes of detachment surgery for stage 4B and stage 5 disease are often poor, prevention of progression is key.8 Surgery of complicated retinal detachments involves vitrectomy with adjunctive instrumentation and techniques and is best left to vitreoretinal surgeons specializing in this field. Visual rehabilitation, particularly after lensectomy, is a critical determinant of final visual function and is best handled by pediatric ophthalmologists working with a motivated family. Thus, the consequences of missed or delayed diagnosis of ROP for long-term visual recovery are grave.
Initial screening examinations of low birth-weight infants always begin (often occur) in the neonatal intensive care unit. Although controversy exists about the indications and timing of initial examination, a screening examination at 4 to 6 weeks of age or 32 to 34 weeks after conception in infants weighing 1500 g or less at birth is reasonable. Eyes with zone II disease, which is less than stage 2, can be seen every 2 weeks. Any zone I or zone II disease that is more advanced than stage 2 but not yet threshold (prethreshold) should be examined weekly or more often. Examinations should occur on schedule until either threshold is reached or the retina vascularizes through zone III.
Infants are dilated with drops containing 0.5% cyclopentolate, 0.5% tropicamide, and 2.5% phenylephrine (see above) in dilute form. Drops are given two times, 5 to 10 minutes apart. Although systemic hypertension is a consideration with mydriatics, adequate pupillary dilation is critical toallow visualization beyond the equator. Alternatively, new technology has been developed that allows photographic visualization and computer storage of images through undilated pupils with a wide angle contact hand-held camera probe (Fig. 21-6). Indirect ophthalmoscopy is performed 30 to 60 minutes after drops are instilled, using a 28- or 30-diopter lens. A lid speculum is inserted after instillation of topical anesthetic; a lens loupe or small culture swab is used for scleral depression. Depression is used to rotate the peripheral retina into view while avoiding excessive pressure on the eye (causing pulsation of the cranial retinal artery or blanching of the optic nerve) or causing bradycardia (the oculocardiac reflex). A retinal drawing showing the extent and tabulatingthe severity of vascular changes is advisable even if the disease appears mild, both for your benefit and for other examiners who might be consulted in the future. Updated drawings should be made on each serial examination until all pathologic changes have stabilized or resolved. You should advise both the neonatal intensive care unit team and the family of your findings.
In the event that prethreshold or threshold disease is found, you must arrange for prompt referral and follow-up with a pediatric ophthalmologist specializing in treatment of ROP if you choose not to treat this yourself. It is prudent to call the family at home to insure that the follow-up recommendations are being complied with.
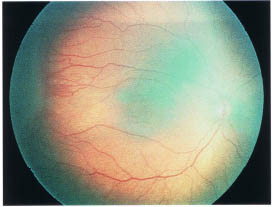
FIGURE 21-6. Digitized image of ROP taken with the wide-angle RET CAM 120¯.
Regressed ROP has a number of permanent sequelae that may be noted on examination of healthy children and adults. These include most commonly myopia, astigmatism, anisometropia, and strabismus. Less common are glaucoma, traction-rhegmatogenous retinal detachment, peripheral retinal folds, avascularity of the peripheral retina, lattice degeneration, macular ectopia, vascular tortuosity orstraightening, and myopia, among others.
Specific methods for treating the vascular lesions of ROP are beyond the scope of this chapter. Both cryopexy and laser applied to nonvascularized retina arrest the progression of ROP to retinal detachment and other blinding sequelae. Only prompt examination and appropriate recognition of the staging of ROP, as well as indications for therapy, will allow either treatment to benefit your patient.
Retinal Detachment
Retinal detachments in children9 are uncommon and usually due to underlying disease such as ROP or retinoblastoma, a syndrome such as Stickler’s syndrome, or trauma (Fig. 21-7). Retinal detachments may be serous, rhegmatogenous, or tractional. In each case, diagnosis of the underlying cause of the detachment is important to the child’s health and long-term visual function. Detailed reviews of the causes of retinal detachments in children can be found elsewhere.1–3
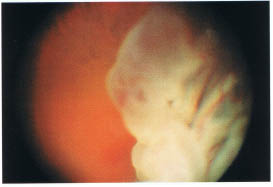
FIGURE 21-7. Giant retinal tear, which may occur in cases of trauma.
Detachment of the retina often occurs in the setting of obvious abnormality of the structure of the eye and body. Abnormalities of vitreous and retinal development will be reviewed briefly in the next section. Other abnormalities, typical of adults such as lattice degeneration or high myopia are correlated with an increased frequency of retinal detachments in children. Conditions may be inherited or occur sporadically and often occur together in the same eye; each may be signs of familial degenerative disorders.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


