3.2 Pathological Findings: Stomach Overview of Pathological Findings in the Stomach Acute Gastritis: Differential Diagnosis and Treatment Chronic Gastritis: Clinical Aspects and Classification Chronic Gastritis: Diagnosis, Giant Fold Gastritis, and Ménétrier Disease Gastric Ulcer: Clinical Aspects and Diagnosis Gastric Ulcer: Helicobacter pylori Mass, Tumor, Malignancy: Overview Mass, Tumor, Malignancy: Diagnosis Mass, Tumor, Malignancy: Intramural Tumors Polypoid Lesions: Benign Tumors Polypoid Lesions: Differential Diagnostic Criteria Polypoid Lesions: Elster Glandular Cysts and Hyperplastic Polyps Polypoid Lesions: Focal Hyperplasia and Chronic Erosions Polypoid Lesions: Adenoma and Rare Findings Malignant Diseases of the Stomach: Gastric Carcinoma, Early Carcinoma Malignant Diseases of the Stomach: Advanced Gastric Carcinoma Malignant Diseases of the Stomach: Diagnosis of Gastric Carcinoma Malignant Diseases of the Stomach: Gastric Lymphoma Malignant Diseases of the Stomach: Gastric Lymphoma, Treatment Portal Hypertension and Hypertensive Gastropathy: Clinical Aspects Portal Hypertension and Hypertensive Gastropathy: Diagnosis The Operated Stomach: Endoscopically Identifiable Lesions and Diseases Partial Gastrectomy: Types and Findings Partial Gastrectomy: Examination Diverticula, Abnormal Gastric Contents Fig. 3.70 Acute gastritis Fig. 3.71 Chronic gastritis Fig. 3.72 Gastric ulcer Fig. 3.730 Gastric polyp Fig. 3.74 Gastric carcinoma Fig. 3.75 Fundic varices Fig. 3.76 Billroth II gastroenterostomy Fig. 3.77 Angiodysplasias Acute and chronic gastritis are reactions of the gastric mucosa to various noxious agents. They are entirely different conditions, each presenting its own clinical, endoscopic, and histological features (Table 3.10). Both conditions, especially the chronic form, pose a special challenge to the endoscopist because the endoscopic findings correlate very poorly with the histological findings and clinical presentation. Acute gastritis can be caused by a variety of exogenous and endogenous agents (Table 3.11). More often than in chronic gastritis, endoscopy reveals signs that point to the correct diagnosis (Table 3.12; Fig. 3.78). The endoscopic features do not suggest a specific causative agent of the gastritis, however. The diagnosis of acute gastritis often relies on the clinical presentation (upper abdominal pain, anorexia, nausea, vomiting) plus the endoscopic findings, with histology showing little or no evidence of cellular infiltrate. The main role of biopsy is to distinguish between the various specific forms of gastritis (due to Crohn disease, infection, etc.). Fig. 3.78 Endoscopic features of acute gastritis Fig. 3.79 Criteria for acute gastritis Fig. 3.80 Differential diagnosis of acute gastritis Acute gastritis is often referable to a time-limited cause that can be identified in the patient’s history (gastroenteritis, alcohol ingestion, medications, stress, etc.). Specific treatment is often unnecessary, but the offending substance must be avoided. Dietary measures are also recommended. If medical treatment is needed, proton pump inhibitors (PPI) are used. Eradication therapy should be considered for severe cases of Helicobacter pylori-positive gastritis. Whereas acute gastritis is usually symptomatic and is responsive to dietary and pharmacological therapy, chronic gastritis frequently causes few or no complaints and shows a limited response to treatment (e.g., eradication therapy). The diagnosis of chronic gastritis can only be established histologically. There is no correlation between the endoscopic appearance and histological findings. In the past, numerous efforts were made to categorize the phenomenon of chronic gastritis. A widely used classification was based on etiological criteria, subdividing the disease into types A, B, and C. “Special forms” were added as a separate category (Table 3.13). Today a modified version of the Sidney classification (1990, 1996) is most commonly used. It takes into account etiological and histological parameters and the location of the gastritis (Table 3.14). Fig. 3.81 Chronic gastritis. Chronic inflammation with subtle histological findings Fig. 3.82a, b Chronic atrophic gastritis Fig. 3.83 Candidal gastritis in a patient with hepatic cirrhosis Fig. 3.84 Chronic gastritis. Prominent vascular pattern Fig. 3.85a, b Mucosal atrophy in chronic gastritis Fig. 3.86 Chronic gastritis. Histology: intestinal metaplasia Giant fold gastritis refers to the presence of gastric folds more than 10 mm thick that are not effaced when the stomach is inflated with air. These folds are located in the body and fundus of the stomach. They are occasionally seen without discernible cause but also occur in the setting of H. pylori infection, Zollinger-Ellison syndrome, lymphoma, and Ménétrier disease. Ménétrier disease is characterized by a hyperplasia of mucus-producing cells combined with gastric protein loss. Endoscopically, the rugal folds appear thickened and show increased tortuosity. Six-month endoscopic follow-ups are recommended initially, mainly to aid differentiation from lymphoma. Later, yearly follow-ups are scheduled due to the risk of malignant change. Gastric ulcer is an epithelial defect that penetrates the muscularis mucosae and extends into the submucosa. Many precipitating factors have been identified, the most important of which are colonization of the gastric mucosa by H. pylori and the ingestion of nonsteroidal anti-inflammatory drugs (NSAIDs). There are no specific ulcer symptoms. Complaints range from immediate pain after eating and nonspecific epigastric discomfort to a complete absence of symptoms. The latter is particularly common with NSAID ulcers. Gastric ulcer is an endoscopic diagnosis, therefore. Endoscopy also allows tissue sampling to differentiate benign and malignant ulcers and permits H. pylori detection as a basis for causal ulcer therapy. Gastric ulcers can occur throughout the stomach. Eighty percent are located on the lesser curvature, usually in the antrum or at the angulus. The fundus, body, and greater curvature are less commonly affected. Basically any ulcer is suspicious for malignancy, and the likelihood of malignant transformation increases with the size of the ulcer. Multiple ulcers are usually seen in association with NSAID use. The endoscopic appearance of an ulcer depends on its stage. Three stages are distinguished: active, healing, and scar: Fig. 3.87 Gastric ulcer – Ulcer margin: one specimen per quadrant – Ulcer base: one specimen per quadrant – Ulcer center: one specimen – Tests for detecting H. pylori (see p. 104) – Histological examination – Rapid urease test – Breath test – Serological testing – Culture method PPI are administered. If H. pylori is detected, the following regimen is used for eradication: Irritants, nicotine, and NSAIDs should be withdrawn. Endoscopy is repeated at four to six weeks, and new specimens are obtained. Additional follow-ups are scheduled according to the progression of healing. Fig. 3.88 Gastric ulcer Fig. 3.89 Histological detection of H. pylori a Low-grade, inactive gastritis b With Warthin–Starry staining, even a relatively low-power view shows H. pylori organisms (black) densely colonizing the ridgesummits and pit epithelium (from: Hahn and Riemann, Klinische Gastroenterologie. Vol. I, 3rd ed. Stuttgart: Thieme 1996) When distended by air insufflation, the stomach wall assumes a uniform appearance in which normal gastric folds are easily distinguished from the conspicuous mass effect produced by an extrinsic indentation, an intramural process, or a lesion in the mucosa (Table 3.15; Fig. 3.90). Masses that bulge into the gastric lumen from the smooth or regularly folded surface often present the examiner with serious difficulties. Endoscopy has a pivotal role in the definitive investigation of these findings. Fig. 3.90 Location of masses in the stomach
Overview of Pathological Findings in the Stomach
 Acute gastritis
Acute gastritis
 Chronic gastritis
Chronic gastritis
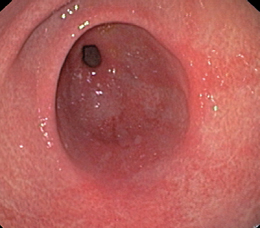
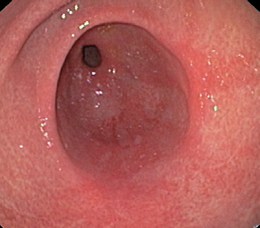
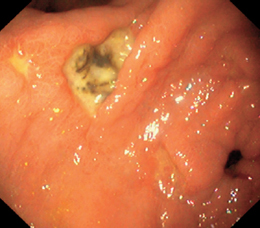
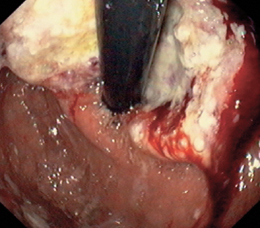
 Gastric ulcer
Gastric ulcer
 Masses
Masses
 Malignancies
Malignancies
 Portal hypertension
Portal hypertension
 Postoperative changes
Postoperative changes
 Rare findings
Rare findings


Gastritis: Clinical Aspects
 Acute Gastritis
Acute Gastritis
 Erosive and hemorrhagic gastritis (acute gastritis)
Erosive and hemorrhagic gastritis (acute gastritis)
 Chronic gastritis
Chronic gastritis
 Special forms (specific gastritides)
Special forms (specific gastritides)
 Bacteria (e.g., Helicobacter pylori)
Bacteria (e.g., Helicobacter pylori)
 Medications (NSAIDs)
Medications (NSAIDs)
 Intoxication (alcohol)
Intoxication (alcohol)
 Reflux (stress) Trauma
Reflux (stress) Trauma
 Mechanical lesion (foreign body, nasogastric tube)
Mechanical lesion (foreign body, nasogastric tube)
 Vasculopathies
Vasculopathies
 Idiopathic
Idiopathic
Acute Gastritis: Diagnosis
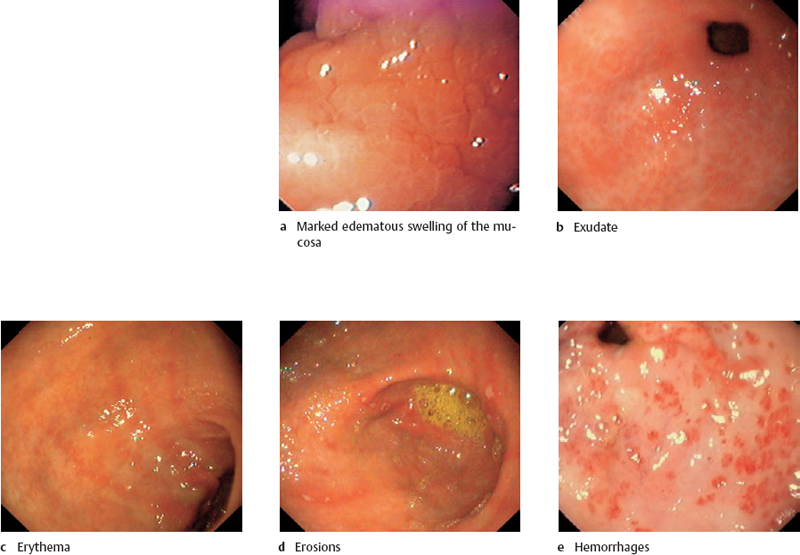
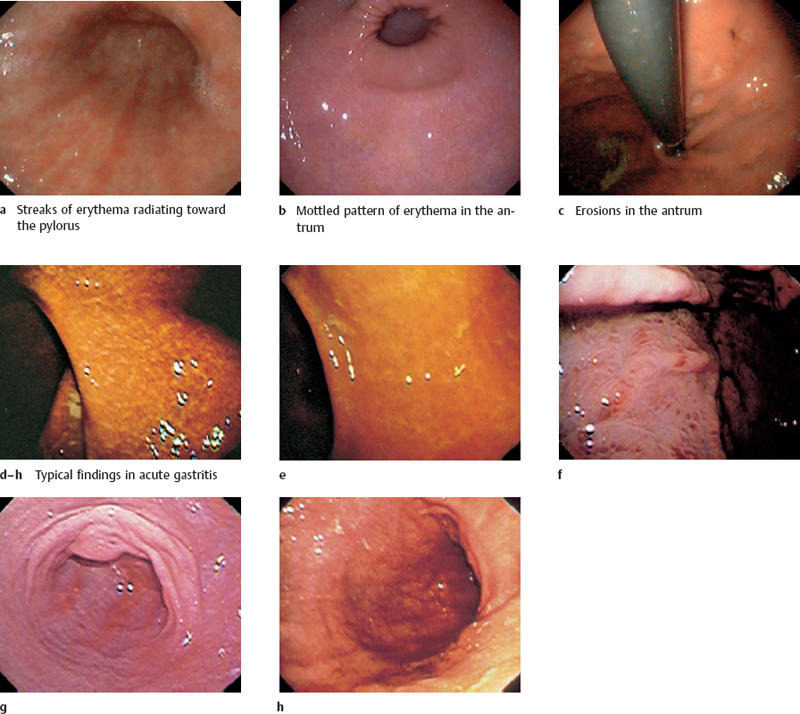
![]() Endoscopic diagnostic criteria (Fig. 3.79)
Endoscopic diagnostic criteria (Fig. 3.79)
 Mucosa may appear normal in some cases
Mucosa may appear normal in some cases
 Edema
Edema
 Exudate
Exudate
 Erythema
Erythema
 Erosion
Erosion
 Bleeding
Bleeding
Acute Gastritis: Differential Diagnosis and Treatment
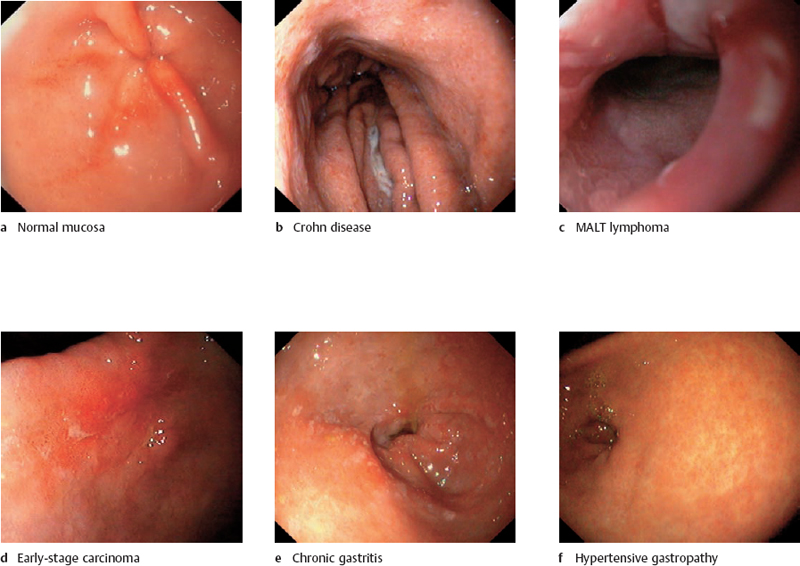
![]() Differential diagnosis (Fig. 3.80)
Differential diagnosis (Fig. 3.80)
 Lymphoma
Lymphoma
 Early carcinoma (circumscribed lesion)
Early carcinoma (circumscribed lesion)
 Chronic gastritis
Chronic gastritis
 Hypertensive gastropathy
Hypertensive gastropathy
 Crohn disease
Crohn disease
 Artifact
Artifact
Checklist for endoscopic evaluation
 Morphology: morphology of individual lesions, distribution
Morphology: morphology of individual lesions, distribution
 Location and extent: antrum, body, fundus, pangastritis
Location and extent: antrum, body, fundus, pangastritis
 Subjective grading of severity: mild, moderate, severe
Subjective grading of severity: mild, moderate, severe
Additional Studies
 Histological examination of biopsies taken from normal-appearing antral and body mucosa and from grossly abnormal mucosa
Histological examination of biopsies taken from normal-appearing antral and body mucosa and from grossly abnormal mucosa
 Rapid urease test of biopsy specimens from the antrum and body
Rapid urease test of biopsy specimens from the antrum and body
 Treatment
Treatment
Chronic Gastritis: Clinical Aspects and Classification
 Clinical Features
Clinical Features
 Classifications
Classifications
 Edema
Edema
 Exudate
Exudate
 Erythema
Erythema
 Erosion
Erosion
 Hemorrhage
Hemorrhage
Type
Cause
Frequency
Type A
Autoimmune gastritis
approximately 5%
Type B gastritis
Bacterial gastritis
approximately 85%
Type C
Toxic chemical gastritis
Toxic chemical gastritis
Special forms
Type of gastritis
Causative factors
Synonyms
 Nonatrophic
Nonatrophic
H. pylori, other factors
Type B gastritis
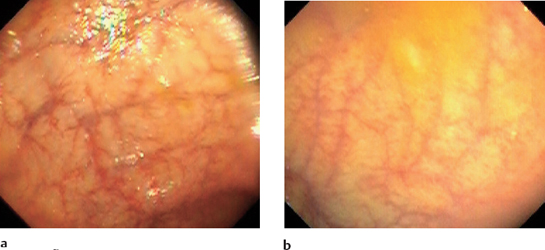
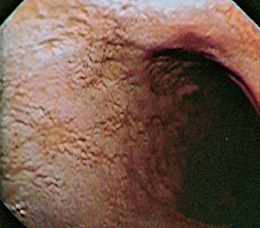
 Atrophic(Fig. 3.82)
Atrophic(Fig. 3.82)
Autoimmune process
Type A gastritis
H. pylori, nutrition,
Type B gastritis
environmental factors
 Special forms
Special forms
Chemical irritation
Type C gastritis
Reflux gastritis
NSAID gastropathy
Radiogenic
Radiation-induced changes
Idiopathic, immunological, gluten-rich diet, medications, H.pylori
Crohn disease
Sarcoidosis, Wegener
matous
disease, vasculitides, foreign bodies, idiopathic
Food sensitivity, other allergens
Bacteria other than H. pylori, viruses, fungi (Fig. 3.83), parasites
Chronic Gastritis: Diagnosis, Giant Fold Gastritis, and Ménétrier Disease
 Diagnosis of Chronic Gastritis
Diagnosis of Chronic Gastritis
![]() Endoscopic diagnostic criteria (Figs. 3.81–3.86)
Endoscopic diagnostic criteria (Figs. 3.81–3.86)
 Endoscopic appearance does not correlate with histological findings.
Endoscopic appearance does not correlate with histological findings.
Differential diagnosis
 Acute gastritis
Acute gastritis
 Early carcinoma (with circumscribed changes)
Early carcinoma (with circumscribed changes)
 Lymphoma
Lymphoma
Checklist for endoscopic evaluation
 Lesion morphology (see above)
Lesion morphology (see above)
 Location: antrum, body, fundus, ubiquitous
Location: antrum, body, fundus, ubiquitous
 Subjective grading of severity: mild, moderate, severe
Subjective grading of severity: mild, moderate, severe
 Additional lesions: Ulcers? Hemorrhage?
Additional lesions: Ulcers? Hemorrhage?
Additional Studies
 Antral biopsy 2-3 cm from the pylorus
Antral biopsy 2-3 cm from the pylorus
 Biopsy from the gastric body
Biopsy from the gastric body
 Biopsy from grossly abnormal areas
Biopsy from grossly abnormal areas
 Rapid test for H. pylori
Rapid test for H. pylori
 Antibodies against parietal cells (type A gastritis)
Antibodies against parietal cells (type A gastritis)
 Vitamin B12 level (type A gastritis)
Vitamin B12 level (type A gastritis)

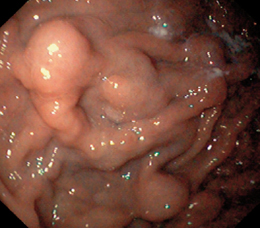
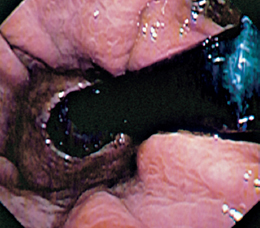
 Giant Fold Gastritis
Giant Fold Gastritis
 Ménétrier Disease
Ménétrier Disease
Gastric Ulcer: Clinical Aspects and Diagnosis
 Definition and Pathophysiology
Definition and Pathophysiology
 Clinical Features
Clinical Features
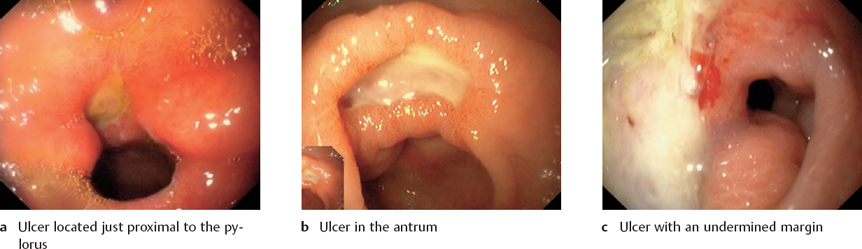
 Location
Location
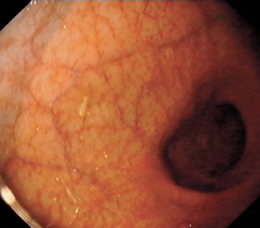
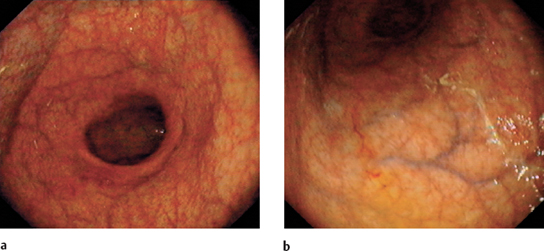
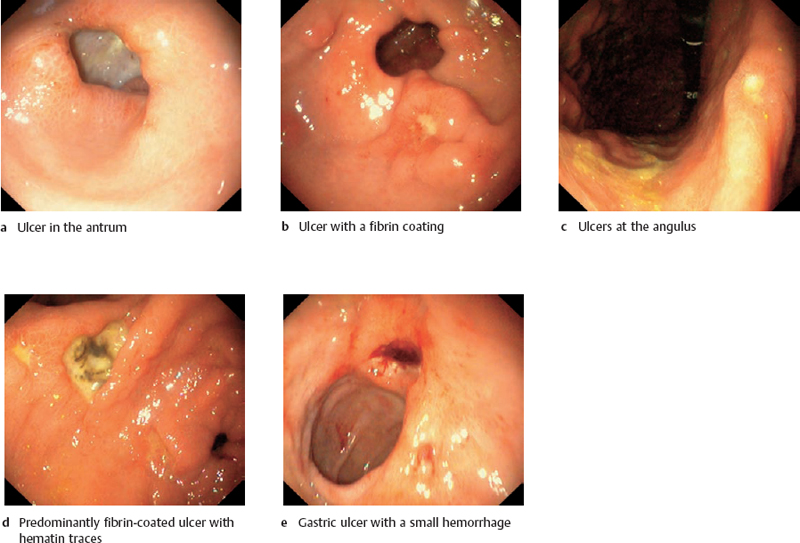
 Diagnosis
Diagnosis
![]() Endoscopic diagnostic criteria (Fig. 3.87, 3.88)
Endoscopic diagnostic criteria (Fig. 3.87, 3.88)
 Active stage
Active stage
 Healing stage
Healing stage
 Scar stage
Scar stage
Differential diagnosis
 Carcinoma
Carcinoma
 Lymphoma
Lymphoma
 Crohn disease
Crohn disease
 Boeck disease
Boeck disease
 Eosinophilic gastritis
Eosinophilic gastritis
 Amyloidosis
Amyloidosis
Checklist for endoscopic evaluation
 Location: prepyloric, antrum, angulus, body, fundus, lesser curvature, greater curvature, anterior wall, posterior wall
Location: prepyloric, antrum, angulus, body, fundus, lesser curvature, greater curvature, anterior wall, posterior wall
 Size: novices tend to overestimate ulcer size. Estimate size with an open biopsy forceps.
Size: novices tend to overestimate ulcer size. Estimate size with an open biopsy forceps.
 Number
Number
 Shape: round, oval, linear, bizarre, irregular
Shape: round, oval, linear, bizarre, irregular
 Ulcer margin: flat, raised
Ulcer margin: flat, raised
 Ulcer base: fresh blood, hematin, fibrin, visible vessel
Ulcer base: fresh blood, hematin, fibrin, visible vessel
 Assess need for endoscopic treatment. Stages I-IIa should be treated (see p. 145 f.).
Assess need for endoscopic treatment. Stages I-IIa should be treated (see p. 145 f.).
Gastric Ulcer: Management
Additional Studies
 Biopsy
Biopsy
 Radiography: Precede endoscopy with abdominal plain film if perforation is suspected.
Radiography: Precede endoscopy with abdominal plain film if perforation is suspected.
 Treatment and Follow-Up
Treatment and Follow-Up
Pharmacological Therapy
Complications
 Oozing hemorrhage
Oozing hemorrhage
 Massive hemorrhage (treatment, see p. 151 ff.)
Massive hemorrhage (treatment, see p. 151 ff.)
 Perforation
Perforation
 Gastric outlet stenosis
Gastric outlet stenosis
Follow-Ups
Problems
 Refractory ulcer
Refractory ulcer
 Dieulafoy ulcer (see p. 155)
Dieulafoy ulcer (see p. 155)
Gastric Ulcer: Helicobacter pylori
 Tests for Detection of Helicobacter pylori
Tests for Detection of Helicobacter pylori
Rapid Urease Test
Principle
 Based on the ability of the organism to convert urea into carbon dioxide and ammonia. A specimen of mucosa is placed into a test medium that contains urea and an indicator dye. If H. pylori is present, the pH rises, producing a characteristic color change, depending on the indicator used.
Based on the ability of the organism to convert urea into carbon dioxide and ammonia. A specimen of mucosa is placed into a test medium that contains urea and an indicator dye. If H. pylori is present, the pH rises, producing a characteristic color change, depending on the indicator used.
Sensitivity
 90-95%
90-95%
Specificity
 95%
95%
Advantages
 Economical
Economical
 Fast (15 minutes to three hours)
Fast (15 minutes to three hours)
Disadvantages
 Does not indicate degree of inflammation
Does not indicate degree of inflammation
Evaluation
 Fast, simple, low-cost test to detect or exclude H. pylori colonization
Fast, simple, low-cost test to detect or exclude H. pylori colonization
Histological Detection
Principle
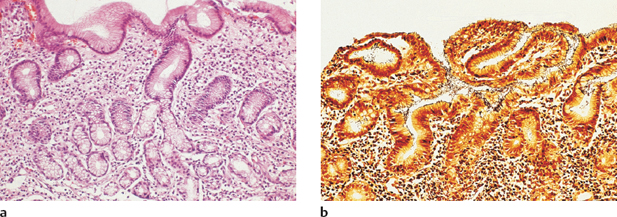
 Staining and direct histological identification of the organism in a tissue specimen (Fig. 3.89)
Staining and direct histological identification of the organism in a tissue specimen (Fig. 3.89)
Sensitivity
 85-95%
85-95%
Specificity
 95-100%
95-100%
Advantages
 Standard method
Standard method
Provides information on inflammatory activity
Disadvantages
 Invasive
Invasive
Evaluation
 Standard method
Standard method
C13 Breath Test
Principle
 The breath test, like the rapid urease test, is based on the ability of H. pylori to break down urea. The patient consumes a test meal containing C13-labeled urea. The H. pylori urease splits the urea, and C13-labeled carbon dioxide is exhaled. The exhaled air is collected and analyzed by mass or infrared spectroscopy.
The breath test, like the rapid urease test, is based on the ability of H. pylori to break down urea. The patient consumes a test meal containing C13-labeled urea. The H. pylori urease splits the urea, and C13-labeled carbon dioxide is exhaled. The exhaled air is collected and analyzed by mass or infrared spectroscopy.
Sensitivity
 90%
90%
Specificity
 95%
95%
Advantages
 Noninvasive
Noninvasive
Disadvantages
 High cost
High cost
Does not indicate degree of inflammation
Evaluation
 Ideal for confirming eradication
Ideal for confirming eradication
Serological Testing
Principle
 Serological tests are based on the detection of IgG and IgA antibodies against H. pylori in the serum. High titers of these antibodies are found during or immediately after a florid infection.
Serological tests are based on the detection of IgG and IgA antibodies against H. pylori in the serum. High titers of these antibodies are found during or immediately after a florid infection.
Sensitivity
 85%
85%
Specificity
 75-80%
75-80%
Advantages
 Noninvasive
Noninvasive
Disadvantages
 Not useful for confirming eradication
Not useful for confirming eradication
 Relatively low sensitivity and specificity
Relatively low sensitivity and specificity
 Does not indicate degree of inflammation
Does not indicate degree of inflammation
Evaluation
 Very useful for epidemiological studies
Very useful for epidemiological studies
 Not useful for planning treatment or evaluating response
Not useful for planning treatment or evaluating response
Culture Method
Principle
 It is possible to culture and identify H. pylori in special laboratories.
It is possible to culture and identify H. pylori in special laboratories.
Sensitivity
 70-90%
70-90%
Specificity
 100%
100%
Advantages
 Can be used to test antibiotic sensitivity
Can be used to test antibiotic sensitivity
Disadvantages
 Invasive
Invasive
 very costly
very costly
 Relative Not a routine method, should be reserved for special investigations
Relative Not a routine method, should be reserved for special investigations
Evaluation
 Not a routine method, should be reserved for special investigations
Not a routine method, should be reserved for special investigations
Mass, Tumor, Malignancy: Overview
 Classification
Classification
 The endoscopic diagnosis is frequently uncertain.
The endoscopic diagnosis is frequently uncertain.
 The nomenclature of these changes, especially polyps, is confusing.
The nomenclature of these changes, especially polyps, is confusing.
 Role of Endoscopy
Role of Endoscopy
 First the mass is visualized endoscopically and its morphology is described.
First the mass is visualized endoscopically and its morphology is described.
 Endoscopy makes it possible to obtain tissue samples, although some limitations apply (see Leiomyoma).
Endoscopy makes it possible to obtain tissue samples, although some limitations apply (see Leiomyoma).
 Based on the endoscopic findings, the need for further testing is assessed. Endosonography is particularly rewarding in equivocal cases.
Based on the endoscopic findings, the need for further testing is assessed. Endosonography is particularly rewarding in equivocal cases.
 Synopsis
Synopsis
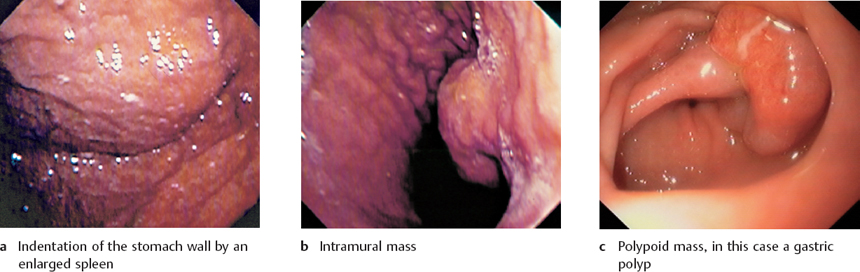
Indentations
Intramural processes
Polypoid lesions
 Sternum
Sternum
 Liver
Liver
 Spleen
Spleen
 Pancreas
Pancreas
 Duodenum
Duodenum
 Intraabdominal metastasis
Intraabdominal metastasis
 Leiomyoma
Leiomyoma
 Hemangioma
Hemangioma
 Lipoma
Lipoma
 Neurofibroma
Neurofibroma
 Intramural gastric carcinoma
Intramural gastric carcinoma
 Leiomyosarcoma
Leiomyosarcoma
 Hyperplastic polyp
Hyperplastic polyp
 Focal foveolar hyperplasia
Focal foveolar hyperplasia
 Chronic erosions
Chronic erosions
 Elster glandular cyst
Elster glandular cyst
 Ectopic pancreatic tissue
Ectopic pancreatic tissue
 Carcinoid
Carcinoid
 Carcinoma
Carcinoma
 Lymphoma
Lymphoma
 Heterotopic Brunner glands
Heterotopic Brunner glands
Mass, Tumor, Malignancy: Diagnosis
![]() Checklist for endoscopic evaluation
Checklist for endoscopic evaluation
 Location
Location
 Size
Size
 Shape and relation to substrate (Fig. 3.91)
Shape and relation to substrate (Fig. 3.91)
 Number
Number
 Mucosal surface
Mucosal surface
 Relation to gastric wall (requires examination with biopsy forceps)
Relation to gastric wall (requires examination with biopsy forceps)
 Lesion morphology should permit a fairly accurate classification
Lesion morphology should permit a fairly accurate classification
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


